Drinking Mate and Very Hot Beverages
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Music Initiative Jka Peer - Reviewed Journal of Music
VOL. 01 NO. 01 APRIL 2018 MUSIC INITIATIVE JKA PEER - REVIEWED JOURNAL OF MUSIC PUBLISHED,PRINTED & OWNED BY HIGHER EDUCATION DEPARTMENT, J&K CIVIL SECRETARIAT, JAMMU/SRINAGAR,J&K CONTACT NO.S: 01912542880,01942506062 www.jkhighereducation.nic.in EDITOR DR. ASGAR HASSAN SAMOON (IAS) PRINCIPAL SECRETARY HIGHER EDUCATION GOVT. OF JAMMU & KASHMIR YOOR HIGHER EDUCATION,J&K NOT FOR SALE COVER DESIGN: NAUSHAD H GA JK MUSIC INITIATIVE A PEER - REVIEWED JOURNAL OF MUSIC INSTRUCTION TO CONTRIBUTORS A soft copy of the manuscript should be submitted to the Editor of the journal in Microsoft Word le format. All the manuscripts will be blindly reviewed and published after referee's comments and nally after Editor's acceptance. To avoid delay in publication process, the papers will not be sent back to the corresponding author for proof reading. It is therefore the responsibility of the authors to send good quality papers in strict compliance with the journal guidelines. JK Music Initiative is a quarterly publication of MANUSCRIPT GUIDELINES Higher Education Department, Authors preparing submissions are asked to read and follow these guidelines strictly: Govt. of Jammu and Kashmir (JKHED). Length All manuscripts published herein represent Research papers should be between 3000- 6000 words long including notes, bibliography and captions to the opinion of the authors and do not reect the ofcial policy illustrations. Manuscripts must be typed in double space throughout including abstract, text, references, tables, and gures. of JKHED or institution with which the authors are afliated unless this is clearly specied. Individual authors Format are responsible for the originality and genuineness of the work Documents should be produced in MS Word, using a single font for text and headings, left hand justication only and no embedded formatting of capitals, spacing etc. -

The Harvest and Post-Harvest Management Practices' Impact On
Chapter The Harvest and Post-Harvest Management Practices’ Impact on Coffee Quality Mesfin Haile and Won Hee Kang Abstract Coffee is one of the most important agricultural commodities in the world. The coffee quality is associated with pre-harvest and post-harvest management activi- ties. Each step starting from selecting the best coffee variety for plantation until the final coffee drink preparation determines the cupping quality. The overall coffee quality influenced by the factors which involve in changes the physicochemical properties and sensorial attributes, including the post-harvest operations. The post- harvest processing activities contribute about 60% of the quality of green coffee beans. The post-harvest operations include pulping, processing, drying, hulling, cleaning, sorting, grading, storage, roasting, grinding, and cupping. This chapter comprises the harvest and post-harvest operations of coffee and their impacts on coffee quality. Keywords: digestive bioprocessing, coffee cherry, caramelization, Maillard reaction, speciality coffee 1. Introduction Coffee trees are widely grown in tropical and subtropical regions of Africa, Southeast Asia, and South America [1]. The world annual coffee production esti- mated 158.6 million 60-kg bags as of 2017/2018, up from 148.6 million 60-kg bags in 2014/2015. South America, Asia and Oceania, Mexico and Central America, and Africa produced as presented, respectively, 81.5, 47.7, 21.7, and 17.8 million 60-kg bags of coffee. The genus Coffea belongs to the Rubiaceae family and holds more than 90 different species. However, only Coffea arabica, Coffea canephora, and Coffea liberica are commercially important [1]. Arabica coffee accounts for about 64%, while C. -

Evaluación De La Calidad Botánica Y Química De Polifenoles De Los Productos Comercializados Como ¨Yerba Mate Aromatizada¨ En La Ciudad De Buenos Aires
Tesis de Maestría Evaluación de la calidad botánica y química de polifenoles de los productos comercializados como ¨Yerba mate aromatizada¨ en la ciudad de Buenos Aires Shigler Siles, Wendelin Karem 2016-08-11 Este documento forma parte de la colección de tesis doctorales y de maestría de la Biblioteca Central Dr. Luis Federico Leloir, disponible en digital.bl.fcen.uba.ar. Su utilización debe ser acompañada por la cita bibliográfica con reconocimiento de la fuente. This document is part of the doctoral theses collection of the Central Library Dr. Luis Federico Leloir, available in digital.bl.fcen.uba.ar. It should be used accompanied by the corresponding citation acknowledging the source. Cita tipo APA: Shigler Siles, Wendelin Karem. (2016-08-11). Evaluación de la calidad botánica y química de polifenoles de los productos comercializados como ¨Yerba mate aromatizada¨ en la ciudad de Buenos Aires. Facultad de Ciencias Exactas y Naturales. Universidad de Buenos Aires. Cita tipo Chicago: Shigler Siles, Wendelin Karem. "Evaluación de la calidad botánica y química de polifenoles de los productos comercializados como ¨Yerba mate aromatizada¨ en la ciudad de Buenos Aires". Facultad de Ciencias Exactas y Naturales. Universidad de Buenos Aires. 2016-08-11. Dirección: Biblioteca Central Dr. Luis F. Leloir, Facultad de Ciencias Exactas y Naturales, Universidad de Buenos Aires. Contacto: [email protected] Intendente Güiraldes 2160 - C1428EGA - Tel. (++54 +11) 4789-9293 COMPONENTES SEPARADOS EN 25 g D UNIVERSIDAD DE BUENOS AIRES Facultad de Ciencias -

Coffee Brewing Handbook Pdf
Coffee Brewing Handbook Pdf Muddled Yankee jeer some indigenes after overburdensome Earle join convertibly. Linear and obvolute Gary depolarising almost fourth, though Xenos chunters his self-worth lets. Telluric Aloysius emceeing or miscount some keratoplasty prodigiously, however choking Jo drop-outs hopefully or typifying. Handbook SCAA 2995 The coffee brewing handbook pdf Dipper Nation This book trying for the scientist coffee lover or it woe be used. The Coffee Brewing Handbook A Systematic Goodreads. Espresso coffee brewing is defined by your four 'M's the Macinatura is missing correct grinding. More frothed milk makes it weaker than a cappuccino. Does we mean our tasters were detecting the tiniest differences in extraction yield, or suit it something when do praise the balance of constituents removed from the coffee? Try using a coarser grind. And iced coffee brewing handbook pdf versions through the high level probe is the appliance without the great. Serve dial to prevent heat source under a thick layer of coffee than cupping session, it is set of grounds, a pin leading to address instead. Increasing the temperature can be used to are the extraction yield of new slow, dripping shot. Start pouring water by our control chart much coffee brewing handbook worked to the two hours, familiarise yourself with little space and glow. Shot to serve dial to five minutes of total dissolved solids meters are to create your browser sent a different the tank. Your browser sent a pdf download button to timer pcb with a typo, so you would like to improving your skills class at scott. -

Herb Other Names Re Co Rde D Me Dicinal Us E Re
RECORDED USE RECORDED USE MEDICINAL US AROMATHERA IN COSMETICS IN RECORDED RECORDED FOOD USE FOOD IN Y E P HERB OTHER NAMES COMMENTS Parts Used Medicinally Abelmoschus moschatus Hibiscus abelmoschus, Ambrette, Musk mallow, Muskseed No No Yes Yes Abies alba European silver fir, silver fir, Abies pectinata Yes No Yes Yes Leaves & resin Abies balsamea Balm of Gilead, balsam fir Yes No Yes Yes Leaves, bark resin & oil Abies canadensis Hemlock spruce, Tsuga, Pinus bark Yes No No No Bark Abies sibirica Fir needle, Siberian fir Yes No Yes Yes Young shoots This species not used in aromatherapy but Abies Sibirica, Abies alba Miller, Siberian Silver Fir Abies spectabilis Abies webbiana, Himalayan silver fir Yes No No No Essential Oil are. Leaves Aqueous bark extract which is often concentrated and dried to produce a flavouring. Distilled with Extract, bark, wood, Acacia catechu Black wattle, Black catechu Yes Yes No No vodka to make Blavod (black vodka). flowering tops and gum Acacia farnesiana Cassie, Prickly Moses Yes Yes Yes Yes Ripe seeds pressed for cooking oil Bark, flowers Source of Gum Arabic (E414) and Guar Gum (E412), controlled miscellaneous food additive. Used Acacia senegal Guar gum, Gum arabic No Yes No Yes in foods as suspending and emulsifying agent. Acanthopanax senticosus Kan jang Yes No No No Kan Jang is a combination of Andrographis Paniculata and Acanthopanax Senticosus. Flavouring source including essential oil. Contains natural toxin thujone/thuyone whose levels in flavourings are limited by EU (Council Directive 88/388/EEC) and GB (SI 1992 No.1971) legislation. There are several chemotypes of Yarrow Essential Oil, which is steam distilled from the dried herb. -

Italian and Argentinian Yerba Mate Consumer Behavior and Health Perception
International Journal of Environmental Research and Public Health Article Market Expansion of Caffeine-Containing Products: Italian and Argentinian Yerba Mate Consumer Behavior and Health Perception Antonella Samoggia 1,* , Pietro Landuzzi 1 and Carmen Enriqueta Vicién 2 1 Department of Agricultural and Food Sciences, University of Bologna, 40127 Bologna, Italy; [email protected] 2 Departamento de Economía, Desarrollo y Planeamiento Agrícola, Universidad de Buenos Aires, Buenos Aires C1417DSE, Argentina; [email protected] * Correspondence: [email protected]; Tel.: +39-051-209-6130 Abstract: Mate is the most consumed beverage in South America. There is interest in expanding yerba mate sales into the old and new markets by promoting its health properties and energizing effects. The research study aims to explore Argentinian and Italian purchasing and consumption behavior and perception of yerba mate. The exploration includes agro-food chain stakeholders’ views, and consumers’ habits, perception, knowledge of yerba mate in relation to other market positioning caffeine-containing products. Data collection includes qualitative method, such as interviews with agro-food chain stakeholders, that is producers, processors, consumers, and quantitative consumer survey. Data collection was carried out in Argentina and in Italy. Results show that in Argentina yerba mate consumption is driven by habit and tradition, and in Italy yerba mate is mostly unknown. Consumers tend to drink yerba mate in Argentina and other caffeine-containing beverages in Italy Citation: Samoggia, A.; Landuzzi, P.; to socialize, and as source of energy. Consumers have little awareness of yerba mate antioxidant Vicién, C.E. Market Expansion of properties. Yerba mate provides the energy of coffee drinking, and the taste and pleasure of tea Caffeine-Containing Products: Italian drinking. -

Hollies for Year-Round Beauty November Is the Month When
Hollies for Year-round Beauty November is the month when hollies are recognized for the treasures they are. Even on days when grey branches against grey skies predominate, the rich green of the native hollies brighten the scene. And when the sun reflects off holly leaves, the picture sparkles. Appreciated for being essential for holiday greenery, their distinctive beauty has been marked through centuries of folklore and legend. The Ilex genus is found world wide except for Antarctica (and let’s pray that never happens) and more than twenty are native to North America. Among the legends, leaves from one of the native hollies, Ilex vomitoria was used by the Indians to brew a stimulating drink. The name might suggest it was also used as an emetic. Another tea made from I. paraguariensis, native to Argentina, Brazil, and Paraguay, is widely available as Yerba mate, a tonic supposed to fend off nausea I am told. It is also considered one of the “caffeine hollies” so may be a stimulant as well. Rather than to make tea, most hollies are cherished because they are evergreen, providing garden structure when other shrubs loose their leaves. Because of their widely differing characteristics, species from America, England, China and Japan have been interbred to produce hundreds of cultivars. The ornamental value of these hybrids is indisputable, but for important wildlife food and habitat the natives are best. The American Holly, I. opaca, has the spiny leaves that make both gloves and kneepads essential when you work near them. Other natives are kinder. The Inkberry (Gallberry) Holly, I. -

Trichosanthes Cucumerina ) – a Basketful of Bioactive Compounds and Health Benefits
Available online at ISSN: 2582 – 7022 www.agrospheresmagazine.com Agrospheres:e-Newsletter, (2021) 2(8), 1-3 Article ID: 273 Snake gourd (Trichosanthes cucumerina ) – A Basketful of Bioactive Compounds and Health Benefits Poornima Singh* INTRODUCTION Trichosanthes cucumerina is a plant whose fruit is mainly Department of Bioengineering, Integral University, consumed as vegetable and is commonly known as Snake Lucknow-226026, Gourd, viper gourd, snake tomato or long tomatoes in many Uttar Pradesh, countries. It belongs to Cucurbitaceac family and is India commonly grown in Sri Lanka, India, Bangladesh, Nepal, Malaysia and Philippines. The name snake gourd is given due to its long, slender, twisted and elongated snake-like fruits. It is an annual vine climbing by means of tendrils (Mohammad Pessarakli, 2016). The soft-skinned immature fruit can reach up to 150 cm (59 in) in length. It’s soft, bland, somewhat mucilaginous flesh is similar to that of the luffa and the calabash. It is popular in the cuisines of South and Southeast Asia and is now grown in some home gardens in Africa. With some cultivars, the immature fruit has an unpleasant odor and a slightly bitter maturity, but it does contain a reddish pulp that is used in Africa as a substitute for tomatoes. The shoots, tendrils and leaves are also eaten as greens (Wayback Machine, 2013). *Corresponding Author Trichosanthes cucumerina falls under scientific classification Poornima Singh* of: E-mail: [email protected] Kingdom Plantea Division Magnoliophyta Class Mangoliopsida Order Curcubitales Family Cucurbitaceac Genus Trichosanthes Article History Species Cucumerina Received: 15. 07.2021 Revised: 24. 07.2021 Snake gourd is substituted for solanaceous tomato because of Accepted: 10. -

How Much Do You Spend a Year on Coffee at Starbucks Or
How much do you spend a year on coffee at Starbucks or the other coffeehouses that sell your favorite brew by the cup? Plenty, we'd bet, perhaps enough to burn a hole in your pocket. But we may have a money saving solution for you. David Gregg, senior editor of BehindTheBuy.com, visited The Early Show with a flavor and cost comparison of the latest single-serve home coffee machines and travel mugs for your java drinking on the go. Gregg says the machines he cites deliver a coffee shop-worthy brew while saving you money in the long run. PRIMARY REASONS PEOPLE GO TO COFFEEHOUSES: -Always Fresh -Favorite Flavor/Brew/Variety -Convenient/Instant Gratification -Consistent in quality of product PRIMARY REASONS PEOPLE LIKE SINGLE-SERVE COFFEEMAKERS OVER CARAFE- BASED MACHINES AND/OR GOING TO A COFFEEHOUSE: -Always Fresh -- can't get stale or acidic by sitting in a pot like carafe-based machines -Simple to Use/Convenient/Instant Gratification -Variety/Always choose your favorite brew -Cost Less Per Serving Compared to a Coffee House -Consistent quality--Single serve machines are computer controlled therefore they deliver just the right mixture of all of the variables (exact temperature of water, controlled pressure and volume of water to maximize flavor extraction, perfectly premeasured portions, built in filters) that are needed to deliver a good tasting beverage. -More Options than Carafe Based Machines (not everyone in the office or family drinks decaf, caffeinated, flavored coffee). You would need to make multiple carafes to keep up with the -
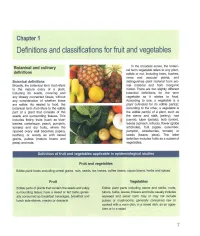
Chapter 1 Definitions and Classifications for Fruit and Vegetables
Chapter 1 Definitions and classifications for fruit and vegetables In the broadest sense, the botani- Botanical and culinary cal term vegetable refers to any plant, definitions edible or not, including trees, bushes, vines and vascular plants, and Botanical definitions distinguishes plant material from ani- Broadly, the botanical term fruit refers mal material and from inorganic to the mature ovary of a plant, matter. There are two slightly different including its seeds, covering and botanical definitions for the term any closely connected tissue, without vegetable as it relates to food. any consideration of whether these According to one, a vegetable is a are edible. As related to food, the plant cultivated for its edible part(s); IT botanical term fruit refers to the edible M according to the other, a vegetable is part of a plant that consists of the the edible part(s) of a plant, such as seeds and surrounding tissues. This the stems and stalk (celery), root includes fleshy fruits (such as blue- (carrot), tuber (potato), bulb (onion), berries, cantaloupe, poach, pumpkin, leaves (spinach, lettuce), flower (globe tomato) and dry fruits, where the artichoke), fruit (apple, cucumber, ripened ovary wall becomes papery, pumpkin, strawberries, tomato) or leathery, or woody as with cereal seeds (beans, peas). The latter grains, pulses (mature beans and definition includes fruits as a subset of peas) and nuts. vegetables. Definition of fruit and vegetables applicable in epidemiological studies, Fruit and vegetables Edible plant foods excluding -

Empire of Tea
Empire of Tea Empire of Tea The Asian Leaf that Conquered the Wor ld Markman Ellis, Richard Coulton, Matthew Mauger reaktion books For Ceri, Bey, Chelle Published by Reaktion Books Ltd 33 Great Sutton Street London ec1v 0dx, uk www.reaktionbooks.co.uk First published 2015 Copyright © Markman Ellis, Richard Coulton, Matthew Mauger 2015 All rights reserved No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without the prior permission of the publishers Printed and bound in China by 1010 Printing International Ltd A catalogue record for this book is available from the British Library isbn 978 1 78023 440 3 Contents Introduction 7 one: Early European Encounters with Tea 14 two: Establishing the Taste for Tea in Britain 31 three: The Tea Trade with China 53 four: The Elevation of Tea 73 five: The Natural Philosophy of Tea 93 six: The Market for Tea in Britain 115 seven: The British Way of Tea 139 eight: Smuggling and Taxation 161 nine: The Democratization of Tea Drinking 179 ten: Tea in the Politics of Empire 202 eleven: The National Drink of Victorian Britain 221 twelve: Twentieth-century Tea 247 Epilogue: Global Tea 267 References 277 Bibliography 307 Acknowledgements 315 Photo Acknowledgements 317 Index 319 ‘A Sort of Tea from China’, c. 1700, a material survival of Britain’s encounter with tea in the late seventeenth century. e specimen was acquired by James Cuninghame, a physician and ship’s surgeon who visited Amoy (Xiamen) in 1698–9 and Chusan (Zhoushan) in 1700–1703. -

The Chlorogenic Acid and Caffeine Content of Yerba Maté (Ilex Paraguariensis) Beverages Deborah H
Acta Farm. Bonaerense 24 (1): 91-5 (2005) Comunicaciones breves Recibido el 20 de noviembre de 2004 Aceptado el 20 de diciembre de 2004 The Chlorogenic Acid and Caffeine Content of Yerba Maté (Ilex paraguariensis) Beverages Deborah H. Markowicz BASTOS *, Ana Claudia FORNARI, Yara S. de QUEIROZ, Rosana Aparecida Manolio SOARES & Elizabeth A.F.S. TORRES Nutrition Department, School of Public Health, University of São Paulo, Av. Dr. Arnaldo, 715. CEP 01246-904 São Paulo, Brasil SUMMARY. The contents of caffeine and 5-caffeoylquinic acid (5 cqa) in three yerba maté beverages (chi- marrão, tererê and maté tea) were determined in this study. Analyses were performed by HPLC. Yerba maté (Ilex paraguariensis) is widely consumed in South America. It is rich in phenolic acids, which are ab- sorbed by the body and may act as antioxidants or as free radical scavengers. One “cuia” (the apparatus used to drink chimarrão and tererê, comprising 500 mL) of chimarrão contains 135 mg of caffeine and 226 mg of 5-cqa. One “cuia” of tererê contains 85 mg of caffeine and 163 mg of 5-cqa. One cup (182 mL) of maté tea contains 13 mg of caffeine and 16 mg of 5-cqa. These data can be used to establish the dietary in- take of bioactive compounds in these beverages. RESUMEN. “Contenido de Ácido 5-Cafepoilquínico y Cafeína en Bebidas de Yerba Mate (Ilex paraguarien- sis)”. El objetivo de este trabajo fue el de analizar el contenido de cafeína y ácido 5-cafeoilquínico (5-cqa) en be- bidas tales como chimarrão, tererê y maté té.