Computational Study of Therapeutic and ADME Associated Proteins
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Supplemental Table S1
Entrez Gene Symbol Gene Name Affymetrix EST Glomchip SAGE Stanford Literature HPA confirmed Gene ID Profiling profiling Profiling Profiling array profiling confirmed 1 2 A2M alpha-2-macroglobulin 0 0 0 1 0 2 10347 ABCA7 ATP-binding cassette, sub-family A (ABC1), member 7 1 0 0 0 0 3 10350 ABCA9 ATP-binding cassette, sub-family A (ABC1), member 9 1 0 0 0 0 4 10057 ABCC5 ATP-binding cassette, sub-family C (CFTR/MRP), member 5 1 0 0 0 0 5 10060 ABCC9 ATP-binding cassette, sub-family C (CFTR/MRP), member 9 1 0 0 0 0 6 79575 ABHD8 abhydrolase domain containing 8 1 0 0 0 0 7 51225 ABI3 ABI gene family, member 3 1 0 1 0 0 8 29 ABR active BCR-related gene 1 0 0 0 0 9 25841 ABTB2 ankyrin repeat and BTB (POZ) domain containing 2 1 0 1 0 0 10 30 ACAA1 acetyl-Coenzyme A acyltransferase 1 (peroxisomal 3-oxoacyl-Coenzyme A thiol 0 1 0 0 0 11 43 ACHE acetylcholinesterase (Yt blood group) 1 0 0 0 0 12 58 ACTA1 actin, alpha 1, skeletal muscle 0 1 0 0 0 13 60 ACTB actin, beta 01000 1 14 71 ACTG1 actin, gamma 1 0 1 0 0 0 15 81 ACTN4 actinin, alpha 4 0 0 1 1 1 10700177 16 10096 ACTR3 ARP3 actin-related protein 3 homolog (yeast) 0 1 0 0 0 17 94 ACVRL1 activin A receptor type II-like 1 1 0 1 0 0 18 8038 ADAM12 ADAM metallopeptidase domain 12 (meltrin alpha) 1 0 0 0 0 19 8751 ADAM15 ADAM metallopeptidase domain 15 (metargidin) 1 0 0 0 0 20 8728 ADAM19 ADAM metallopeptidase domain 19 (meltrin beta) 1 0 0 0 0 21 81792 ADAMTS12 ADAM metallopeptidase with thrombospondin type 1 motif, 12 1 0 0 0 0 22 9507 ADAMTS4 ADAM metallopeptidase with thrombospondin type 1 -

Functions of Nogo Proteins and Their Receptors in the Nervous System
REVIEWS Functions of Nogo proteins and their receptors in the nervous system Martin E. Schwab Abstract | The membrane protein Nogo-A was initially characterized as a CNS-specific inhibitor of axonal regeneration. Recent studies have uncovered regulatory roles of Nogo proteins and their receptors — in precursor migration, neurite growth and branching in the developing nervous system — as well as a growth-restricting function during CNS maturation. The function of Nogo in the adult CNS is now understood to be that of a negative regulator of neuronal growth, leading to stabilization of the CNS wiring at the expense of extensive plastic rearrangements and regeneration after injury. In addition, Nogo proteins interact with various intracellular components and may have roles in the regulation of endoplasmic reticulum (ER) structure, processing of amyloid precursor protein and cell survival. Nogo proteins were discovered, and have been exten- The amino-terminal segments of the proteins sively studied, in the context of injury and repair of fibre encoded by the different RTN genes have differing tracts in the CNS1 — a topic of great research interest lengths and there is no homology between them3,5. The and clinical relevance. However, much less in known N termini of the RTN4 products Nogo-A and Nogo-B are about the physiological functions of Nogo proteins in identical, consisting of a 172-amino acid sequence that development and in the intact adult organism, including is encoded by a single exon (exon 1) that is followed by in the brain. Through a number of recent publications, a short exon 2 and, in Nogo-A, by the very long exon Nogo proteins have emerged as important regulators of 3 encoding 800 amino acids2,6 (FIG. -

Recombinant Mouse Ngr (C-6His) Derived from Human Cells
Catalog # CM42 Recombinant Mouse NgR (C-6His) Derived from Human Cells Recombinant Mouse Nogo-66 Receptor/Reticulon 4 Receptor is produced by our Mammalian expression system and the target gene encoding Cys27-Ser447 is expressed with a 6His tag at the C-terminus. DESCRIPTION Accession Q99PI8 Known as Reticulon-4 Receptor; Nogo Receptor; NgR; Nogo-66 Receptor; RTN4R; NOGOR Mol Mass 46.6kDa AP Mol Mass 75-85 kDa, reducing conditions. QUALITY CONTROL Purity Greater than 95% as determined by reducing SDS-PAGE. Endotoxin Less than 0.1 ng/µg (1 EU/µg) as determined by LAL test. FORMULATION Lyophilized from a 0.2 μm filtered solution of PBS, pH 7.4. Always centrifuge tubes before opening. Do not mix by vortex or pipetting. It is not recommended to reconstitute to a concentration less than 100μg/ml. RECONSTITUTION Dissolve the lyophilized protein in distilled water. Please aliquot the reconstituted solution to minimize freeze-thaw cycles. The product is shipped at ambient temperature. SHIPPING Upon receipt, store it immediately at the temperature listed below. Lyophilized protein should be stored at < -20°C, though stable at room temperature for 3 weeks. STORAGE Reconstituted protein solution can be stored at 4-7°C for 2-7 days. Aliquots of reconstituted samples are stable at < -20°C for 3 months. Nogo Receptor (NgR) is a glycosylphosphoinositol (GPI)-anchored protein that belongs to the Nogo recptor family. Human NgR is predominantly expressed in neurons and their axons in the central nervous systems. As a receptor for myelin-derived proteins Nogo, myelin-associated glycoprotein (MAG) and myelin BACKGROUND oligodendrocyte glycoprotein (OMG), NgR mediates axonal growth inhibition and may play a role in regulating axonal regeneration and plasticity in the adult central nervous system. -
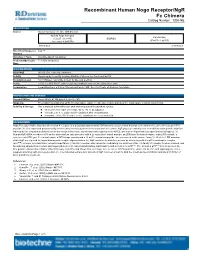
Recombinant Human Nogo Receptor/Ngr Fc Chimera
Recombinant Human Nogo Receptor/NgR Fc Chimera Catalog Number: 1208-NG DESCRIPTION Source Mouse myeloma cell line, NS0derived Human Nogo Receptor Human IgG (Cys27 Ser 447) IEGRMD 1 (Pro100 Lys330) Accession # Q9BZR6 Nterminus Cterminus Nterminal Sequence Cys27 Analysis Structure / Form Disulfidelinked homodimer Predicted Molecular 71.8 kDa (monomer) Mass SPECIFICATIONS SDSPAGE 95105 kDa, reducing conditions Activity Measured by its ability to bind rrMAG/Fc Chimera in a functional ELISA. Endotoxin Level <0.01 EU per 1 μg of the protein by the LAL method. Purity >95%, by SDSPAGE under reducing conditions and visualized by silver stain. Formulation Lyophilized from a 0.2 μm filtered solution in PBS. See Certificate of Analysis for details. PREPARATION AND STORAGE Reconstitution Reconstitute at 100 μg/mL in sterile PBS. Shipping The product is shipped at ambient temperature. Upon receipt, store it immediately at the temperature recommended below. Stability & Storage Use a manual defrost freezer and avoid repeated freezethaw cycles. l 12 months from date of receipt, 20 to 70 °C as supplied. l 1 month, 2 to 8 °C under sterile conditions after reconstitution. l 3 months, 20 to 70 °C under sterile conditions after reconstitution. BACKGROUND Nogo Receptor (NgR), also named reticulon 4 receptor, is a glycosylphosphoinositol (GPI)anchored protein that belongs to the family of leucinerich repeat (LRR) proteins (1). It is expressed predominantly in the central nervous systems in neurons and their axons. NgR plays an essential role in mediating axon growth inhibition induced by the structurally distinct myelinderived proteins Nogo, myelinassociated glycoprotein (MAG), and myelin oligodendrocyte glycoprotein (Omgp) (2, 3). -

Limiting Neuronal Nogo Receptor 1 Signaling During Experimental Autoimmune Encephalomyelitis Preserves Axonal Transport and Abrogates Inflammatory Demyelination
5562 • The Journal of Neuroscience, July 10, 2019 • 39(28):5562–5580 Neurobiology of Disease Limiting Neuronal Nogo Receptor 1 Signaling during Experimental Autoimmune Encephalomyelitis Preserves Axonal Transport and Abrogates Inflammatory Demyelination Jae Young Lee,1,4* Min Joung Kim,1* Speros Thomas,1 XViola Oorschot,5 Georg Ramm,6 XPei Mun Aui,1 Yuichi Sekine,7 X Devy Deliyanti,2 XJennifer Wilkinson-Berka,2 Be’eri Niego,3 XAlan R. Harvey,8,9 Paschalis Theotokis,10 X Catriona McLean,11 XStephen M. Strittmatter,7 and XSteven Petratos1 Departments of 1Neuroscience, 2Diabetes, 3Australian Centre of Blood Diseases, Central Clinical School, Monash University, Prahran, Victoria 3004, Australia, 4ToolGen Inc., Gasan Digital-Ro, Geumcheon, 08501, Seoul, Korea, 5Monash Ramaciotti Centre for Cryo Electron Microscopy, 6Department of Biochemistry and Molecular Biology, Biomedicine Discovery Institute and Monash Ramaciotti Centre for Cryo Electron Microscopy, Monash University, Melbourne, Victoria 3800, Australia, 7Program in Cellular Neuroscience, Neurodegeneration and Repair, Yale University School of Medicine, New Haven, Connecticut 06536, 8School of Human Sciences, The University of Western Australia, Nedlands, Washington 6009, Australia, 9Perron Institute for Neurological and Translational Science, Washington, Australia, 10B’ Department of Neurology, Laboratory of Experimental Neurology and Neuroimmunology, AHEPA University Hospital, 54636, Thessaloniki, Macedonia, Greece, and 11Department of Anatomical Pathology, Alfred Hospital, Prahran, Victoria 3004, Australia We previously identified that ngr1 allele deletion limits the severity of experimental autoimmune encephalomyelitis (EAE) by preserving axonal integrity. However, whether this favorable outcome observed in EAE is a consequence of an abrogated neuronal-specific patho- physiological mechanism, is yet to be defined. Here we show that, Cre-loxP-mediated neuron-specific deletion of ngr1 preserved axonal integrity, whereas its re-expression in ngr1؊/؊ female mice potentiated EAE-axonopathy. -

Pooled Extracellular Receptor-Ligand Interaction Screening Using CRISPR Activation Zheng-Shan Chong1, Shuhei Ohnishi2, Kosuke Yusa2 and Gavin J
Chong et al. Genome Biology (2018) 19:205 https://doi.org/10.1186/s13059-018-1581-3 METHOD Open Access Pooled extracellular receptor-ligand interaction screening using CRISPR activation Zheng-Shan Chong1, Shuhei Ohnishi2, Kosuke Yusa2 and Gavin J. Wright1* Abstract Extracellular interactions between cell surface receptors are necessary for signaling and adhesion but identifying them remains technically challenging. We describe a cell-based genome-wide approach employing CRISPR activation to identify receptors for a defined ligand. We show receptors for high-affinity antibodies and low-affinity ligands can be unambiguously identified when used in pools or as individual binding probes. We apply this technique to identify ligands for the adhesion G-protein-coupled receptors and show that the Nogo myelin- associated inhibitory proteins are ligands for ADGRB1. This method will enable extracellular receptor-ligand identification on a genome-wide scale. Keywords: Cell surface receptors, Cell signaling, CRISPR activation, Extracellular protein interactions, Flow cytometry, Genome-wide screening, G-protein-coupled receptor, Monoclonal antibodies Background captured in addressed arrays and tested for direct bind- Identifying cell surface receptors for ligands such as pro- ing with prey proteins that are oligomerized to increase teins, small molecules, or whole pathogens, is an import- local avidity and permit the detection of even very weak ant step towards understanding how intercellular interactions. While this approach has enabled the con- signaling events are initiated and discovering new drug struction of extracellular protein-protein interaction net- targets. Because the extracellular regions of receptors – are directly accessible to systemically delivered therapeu- works [4 6], creating comprehensive libraries containing tics, particularly monoclonal antibodies, these proteins thousands of different recombinant proteins is impracti- and their interactions are highly valued targets and cal for most laboratories. -

Transdifferentiation of Human Mesenchymal Stem Cells
Transdifferentiation of Human Mesenchymal Stem Cells Dissertation zur Erlangung des naturwissenschaftlichen Doktorgrades der Julius-Maximilians-Universität Würzburg vorgelegt von Tatjana Schilling aus San Miguel de Tucuman, Argentinien Würzburg, 2007 Eingereicht am: Mitglieder der Promotionskommission: Vorsitzender: Prof. Dr. Martin J. Müller Gutachter: PD Dr. Norbert Schütze Gutachter: Prof. Dr. Georg Krohne Tag des Promotionskolloquiums: Doktorurkunde ausgehändigt am: Hiermit erkläre ich ehrenwörtlich, dass ich die vorliegende Dissertation selbstständig angefertigt und keine anderen als die von mir angegebenen Hilfsmittel und Quellen verwendet habe. Des Weiteren erkläre ich, dass diese Arbeit weder in gleicher noch in ähnlicher Form in einem Prüfungsverfahren vorgelegen hat und ich noch keinen Promotionsversuch unternommen habe. Gerbrunn, 4. Mai 2007 Tatjana Schilling Table of contents i Table of contents 1 Summary ........................................................................................................................ 1 1.1 Summary.................................................................................................................... 1 1.2 Zusammenfassung..................................................................................................... 2 2 Introduction.................................................................................................................... 4 2.1 Osteoporosis and the fatty degeneration of the bone marrow..................................... 4 2.2 Adipose and bone -

Oligodendrocytes Remodel the Genomic Fabrics of Functional Pathways in Astrocytes
1 Article 2 Oligodendrocytes remodel the genomic fabrics of 3 functional pathways in astrocytes 4 Dumitru A Iacobas 1,2,*, Sanda Iacobas 3, Randy F Stout 4 and David C Spray 2,5 5 Supplementary Material 6 Table S1. Genes whose >1.5x absolute fold-change did not meet the individual CUT criterion. 7 Red/green background of the expression ratio indicates not significant (false) up-/down-regulation. Gene Description X CUT Acap2 ArfGAP with coiled-coil, ankyrin repeat and PH domains 2 -1.540 1.816 Adamts18 a disintegrin-like and metallopeptidase -1.514 1.594 Akr1c12 aldo-keto reductase family 1, member C12 1.866 1.994 Alx3 aristaless-like homeobox 3 1.536 1.769 Alyref2 Aly/REF export factor 2 -1.880 2.208 Ankrd33b ankyrin repeat domain 33B 1.593 1.829 Ankrd45 ankyrin repeat domain 45 1.514 1.984 Ankrd50 ankyrin repeat domain 50 1.628 1.832 Ankrd61 ankyrin repeat domain 61 1.645 1.802 Arid1a AT rich interactive domain 1A -1.668 2.066 Artn artemin 1.524 1.732 Aspm abnormal spindle microtubule assembly -1.693 1.716 Atp6v1e1 ATPase, H+ transporting, lysosomal V1 subunit E1 -1.679 1.777 Bag4 BCL2-associated athanogene 4 1.723 1.914 Birc3 baculoviral IAP repeat-containing 3 -1.588 1.722 Ccdc104 coiled-coil domain containing 104 -1.819 2.130 Ccl2 chemokine -1.699 2.034 Cdc20b cell division cycle 20 homolog B 1.512 1.605 Cenpf centromere protein F 2.041 2.128 Cep97 centrosomal protein 97 -1.641 1.723 COX1 mitochondrially encoded cytochrome c oxidase I -1.607 1.650 Cpsf7 cleavage and polyadenylation specific factor 7 -1.635 1.891 Crct1 cysteine-rich -

Continuously Active Transcriptional Programs Are Required to Build Expansive Serotonergic Axon Architectures
CONTINUOUSLY ACTIVE TRANSCRIPTIONAL PROGRAMS ARE REQUIRED TO BUILD EXPANSIVE SEROTONERGIC AXON ARCHITECTURES By LAUREN JANINE DONOVAN Submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy Dissertation Advisor: Evan S. Deneris Department of Neurosciences CASE WESTERN RESERVE UNIVERSITY January 2020 CASE WESTERN RESERVE UNIVERSITY SCHOOL OF GRADUATE STUDIES We hereby approve the thesis/dissertation of Lauren Janine Donovan candidate for the degree of Doctor of Philosophy*. Committee Chair Jerry Silver, Ph.D. Committee Member Evan Deneris, Ph.D. Committee Member Heather Broihier, Ph.D. Committee Member Ron Conlon, Ph.D. Committee Member Pola Philippidou, Ph.D. Date of Defense August 29th, 2019 *We also certify that written approval has been obtained for any proprietary material contained therein. ii TABLE OF CONTENTS List of Figures……………………………………………………………………….….vii Abstract………………………………………….………………………………..….…1 CHAPTER 1. INTRODUCTION………………………………………………...……..3 GENERAL INTRODUCTION TO SEROTONIN………………………………….….4 Serotonin: Discovery and function………………………….……………...4 Serotonin Biosynthesis…………………………..…………………………..6 Manipulation of the serotonin system in humans……………………….6 Human mutations in 5-HT related genes………………………………….9 SEROTONIN NEURON NEUROGENESIS……………..………………………….11 5-HT neuron specification……………..………………………………...…11 Development of 5-HT neurons……………..………………………………13 NEUROANATOMY……………..……………………………………………………..13 Cytoarchitecture ……………..………………………………………………13 Adult Ascending 5-HT axon projection system ………………………..14 -

Goat Anti-Nogo 66 Receptor Antibody Peptide-Affinity Purified Goat Antibody Catalog # Af1737a
10320 Camino Santa Fe, Suite G San Diego, CA 92121 Tel: 858.875.1900 Fax: 858.622.0609 Goat Anti-Nogo 66 receptor Antibody Peptide-affinity purified goat antibody Catalog # AF1737a Specification Goat Anti-Nogo 66 receptor Antibody - Product Information Application WB Primary Accession Q9BZR6 Other Accession NP_075380, 65078 Reactivity Human Predicted Mouse, Rat, Pig, Dog Host Goat Clonality Polyclonal Concentration 100ug/200ul Isotype IgG Calculated MW 50708 Goat Anti-Nogo 66 receptor Antibody - Additional Information AF1737a (0.3 µg/ml) staining of Human Brain lysate (35 µg protein in RIPA buffer) with (B) Gene ID 65078 and without (A) blocking with the immunising peptide. Primary incubation was 1 hour. Other Names Detected by chemiluminescence. Reticulon-4 receptor, Nogo receptor, NgR, Nogo-66 receptor, RTN4R, NOGOR Goat Anti-Nogo 66 receptor Antibody - Format Background 0.5 mg IgG/ml in Tris saline (20mM Tris pH7.3, 150mM NaCl), 0.02% sodium azide, This gene encodes the receptor for reticulon 4, with 0.5% bovine serum albumin oligodendrocyte myelin glycoprotein and myelin-associated glycoprotein. This receptor Storage mediates axonal growth inhibition and may Maintain refrigerated at 2-8°C for up to 6 play a role in regulating axonal regeneration months. For long term storage store at and plasticity in the adult central nervous -20°C in small aliquots to prevent system. freeze-thaw cycles. Goat Anti-Nogo 66 receptor Antibody - Precautions References Goat Anti-Nogo 66 receptor Antibody is for research use only and not for use in Distinct DNA methylation profiles between diagnostic or therapeutic procedures. adenocarcinoma and squamous cell carcinoma of human uterine cervix. -
Sheep Shearing and Epigenetic Change
Project No. 18-025 Contract No. ON-00593 AWI Project Manager: Dr Carolina Diaz Contractor Name: The University of Queensland Prepared by: Dr Edward Narayan, Mr Gregory Sawyer, Mr Dylan Fox and Prof. Alan Tilbrook Publication date: June 2020 Sheep Shearing and Epigenetic Change Published by Australian Wool Innovation Limited, Level 6, 68 Harrington Street, THE ROCKS, NSW, 2000 This publication should only be used as a general aid and is not a substitute for specific advice. To the extent permitted by law, we exclude all liability for loss or damage arising from the use of the information in this publication. AWI invests in research, development, innovation and marketing activities along the global supply chain for Australian wool. AWI is grateful for its funding which is primarily provided by Australian woolgrowers through a wool levy and by the Australian Government which provides a matching contribution for eligible R&D activities © 2019 Australian Wool Innovation Limited. All rights reserved. Contents Executive Summary 1. Introduction 2. Literature Review 3. Project Objectives 4. Success in Achieving Objectives 5. Methodology 6. Results 7. Discussion 8. Impact of Wool Industry – Now & in 5 years’ time 9. Conclusions and Recommendations 10. Bibliography 11. List of abbreviations and/or glossary 12. Appendices a. Appendix 1 – AWI Communication Report Template (see attached) b. Appendix 2 – List of Milestones & Dates submitted c. Appendix 3 – Remaining Assets d. Appendix 4 – Any Project Intellectual Property e. Appendix 5 – Storage of Primary Research Data (Paper based and electronic) f. Appendix 6 – Animal Ethics Approval (if any) 2 | Page PROJECT FINAL REPORT Executive Summary The primary objective of this research was to test the influence of shearing frequency (twice shorn versus single shorn) on the epigenetic DNA methylation patterns in a Merino sheep flock over a period of 1 generation. -

RTN4RL2 Antibody (Pab)
21.10.2014RTN4RL2 antibody (pAb) Rabbit Anti-Human Reticulon 4 receptor-like 2 (NgR2, NGRH1, NGRL3, Nogo -66 receptor -related protein) Instruction Manual Catalog Number PK-AB718-7145 Synonyms RTN4RL2 Antibody: Reticulon 4 receptor-like 2, NgR2, NGRH1, NGRL3, Nogo receptor-like 3, Nogo-66 receptor homolog 1, Nogo-66 receptor-related protein Description Reticulon 4 receptor-like 2 (RTN4RL2), also known as NgR2and NgRH1, is a 60 kDa glycosylphosphatidylinositol-anchored protein that is expressed primarily in the brain. It contains eight leucine-rich repeats that are flanked by cysteine-rich sequences at both the N- and C-termini. The membrane anchored RTN4RL2 can be solubilized through the action of phospholipase or an unidentified MTMMP to generate a 46 kDa soluble receptor. It has been suggested that RTN4RL2 may play a role in regulating axonal regeneration and plasticity in the adult central nervous system. Quantity 100 µg Source / Host Rabbit Immunogen Rabbit polyclonal RTN4RL2 antibody was raised against an 18 amino acid peptide near the carboxy terminus of human RTN4RL2. Purification Method Affinity chromatography purified via peptide column. Clone / IgG Subtype Polyclonal antibody Species Reactivity Human Specificity Three alternatively spliced transcript variants have been observed. RTN4RL2 antibody is predicted to not cross-react with other Nogo receptor-like proteins. Formulation Antibody is supplied in PBS containing 0.02% sodium azide. Reconstitution During shipment, small volumes of antibody will occasionally become entrapped in the seal of the product vial. For products with volumes of 200 μl or less, we recommend gently tapping the vial on a hard surface or briefly centrifuging the vial in a tabletop centrifuge to dislodge any liquid in the container’s cap.