Primary Care Clinical Quality Rolling 12 Months MAP and Sliding Fee Scale Patients
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2005 Programmers Handbook
Table of Contents History ......................................................................................................... 2 Mission Statement............................................................................................ 2 Organization Structure ...................................................................................... 2 KAZI Goals and General Policies...................................................................... 3 Non Compete Policy ................................................................................ 3 On-Air Rules ........................................................................................... 5 Food ...................................................................................................... 5 Personnel ............................................................................................... 5 Logs ...................................................................................................... 5 Open Mike Guidelines .............................................................................. 6 Equipment ............................................................................................. 6 Security.................................................................................................. 6 Format ................................................................................................... 7 Play lists................................................................................................. 7 PSA Promo on Program Log -

Alamo Alamo Heights Alice Alpine Amarillo Arlington Athens Atlanta
KWKC(AM) -June 19. 1948: 1340 khz; 1 kw -D. 250 KBUY -FM -Co -owned with KDJW(AM). March 1946: Texas Radio w -N, DA -1. 2449 S. Treadaway (79604). (915) 94.1 mhz; 54 kw. Ant 700 ft. (CP: 100 kw). Prog sep 673-2545. Adams -Shelton Communications (acq from AM. Dups AM 25 %. Stereo. Mark Meredith, prog 12- 23 -80). Net: NBC, TSN. Rep: Hillier; Newmark & mgr; Gary Lee & Darlene Austin. mus dirs. Rates: Wechsler. Format: C &W. Spec prog: Farm 3 hrs wkly S24; 24; 24; 18. Keith Adams, pres; Terry L. Bettis. gen mgr; Dave Mar- tin. coml mgr; Kevin Wasner mus dir; Randy Wyles, KGNC(AM) -May 19.1922: 710 khz: 10 kw -U, DA -2. new dir; Gary Smith, chief engr. Rates: $14; 12; 14; Box 710 (79189). (806) 355 -9801. Stauffer Com- Format: Rel. Jimmy 12. munications Inc. (group owner). Net: CBS, Tex State Radio, acq 6.11 -76). Net: APR. Net. Rep: Katz. Format: Adult contemp, farm. Spec Swaggart, pres; Jack Rabito, gen & gen sis mgr; Paul KORQ(FM) -Co-owned with KWKC(AM). September progs: C &W 6 hrs, farm 23 hrs wkly. Jerry Holley, VP; Hughes, prod mgr; Barbara Bates, traff & mus dir; Kim 1974: 100.7 mhz; 100 kw. Ant 1,260 ft. Prog sep from Royce Bodiford, gen mgr; Rick Neves, sis mgr; John Willis, prom mgr; Mal Couch, news dir; John Allison, AM. Stereo. Mark Connell, coml mgr: Pat Whitehead, Dawson, prog dir; Greg Phillips, mus dir; Dean Taylor, chief engr. Rates: 532; 28; 30; 22. prog & mus dir. -
KAZI Weekly Program Schedule
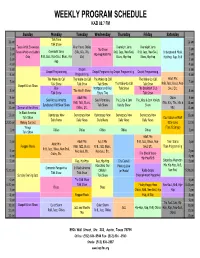
WEEKLY PROGRAM SCHEDULE KAZI 88.7 FM Sunday Monday Tuesday Wednesday Thursday Friday Saturday Talk Time 12 am 12 am Talk Show Texas Artist Showcase After Hours Oldies Overnight Jams Overnight Jams 1 am The Show 1 am Texas Artists and Labels Overnight Jams (50s, 60s, 70s, RnB, Jazz, Neo-Soul, RnB, Jazz, Neo-Soul, Underground Music 2 am Hip-Hop/RnB Mix 2 am Only RnB, Jazz, Neo-Soul, Blues, Hip- 80s) Blues, Hip-Hop Blues, Hip-Hop Hip-Hop, Rap, RnB 3 am 3 am Hop 4 am 4 am 5 am Gospel 5 am Gospel Programming Gospel Programming Gospel Programming Gospel Programming 6 am Programming 6 am The Wake-Up Call The Wake-Up Call The Wake-Up Call The Wake-Up Call Adult Mix 7 am 7 am The Wake-Up Call RnB, Jazz, Blues, Neo- Gospel Music Show Talk Show Talk Show Talk Show Talk Show Rise Mortgage and Real Talk Show The Breakfast Club Soul, Etc. 8 am The Health Show 8 am Talk Show Estate Tips Talk Show 9 am Adult Mix Oldies 9 am Soul Across America Soul Vibrations The Juice & Jam The Juice & Jam Variety 10 am RnB, Jazz, Blues, (50s, 60s, 70s, 80s & 10 am Syndicated Old Skool Show Talk Show Variety Show Show 11 am Sermon of the Week Oldies, Etc. 90s) 11 am In Black America 12 pm Democracy Now Democracy Now Democracy Now Democracy Now Democracy Now 12 pm Talk Show Countdown w/Walt Daily News Daily News Daily News Daily News Daily News 12:30 pm Making Contact Baby Love 12:30 Wings (Top 25 Songs) 1 pm Oldies Oldies Oldies Oldies Oldies 1 pm Talk Show Adult Mix 2 pm Adult Mix Adult Mix RnB, Jazz, Blues, Neo- Teen Scene 2 pm Adult Mix Reggae Music RnB, Jazz, Blues, RnB, Jazz, Blues, Soul, Etc. -
Page 1 Aug 31
Presorted Standard U.S. Postage Paid Austin, Texas Permit No. 01949 TPA TEXAS PUBLISHERS ASSOCIATION TheAustinVillager.com This paper can be recycled Vol. 40 No. 16 Phone: 512-476-0082 Email: [email protected] August 31, 2012 KAZI STILL GOING STRONG INSIDE AFTER 30 YEARS 27 year volunteer is one of the on-line personalities. She said a lot of stations have not existed for as long as KAZI. RAPPIN’ “People in Austin may not Want To Earn $1,250 realize what a gold mine All You Need Is to Tommy Wyatt KAZI is,” she stated. She Decrease Outdoor Irrigation features the Hot Pepper Find Out If You Are Eligible New Ruling See AUSTIN WATER Show on Saturdays from Page 3 in Redistricting 6pm-9pm. Case Pepper was very proud of the fact that her co- The NAACP and volunteers are dedicated and Black Political Leaders are passionate about what they elated over the ruling of a are able to bring to the lis- 3 judge panel in D.C this teners. She knows they week in the Texas Redis- could take their talents and tricting case. wishes elsewhere, and she’s The panel was a bi- With More Than 1/2 of By Shirley A. Hammond glad that they don’t. In her partisan one that put indi- tion kept going into the night Listeners in Japan and Aus- Texas Public Schools Special to The Villager th view, the mix of volunteers vidual and partisan interest on Saturday, August 25 . tin hear the same content. Failing Yearly Benchmarks, and workers bring something aside in fashioning this opin- And The Beat Jan Warfield, one of the This is a departure from the A Change Comes With unique to the community of lis- Newly Annouced Educator ion. -

List of Radio Stations in Texas
Texas portal List of radio stations in Texas From Wikipedia, the free encyclopedia The following is a list of FCC-licensed AM and FM radio stations in the U.S. state of Texas, which can be sorted by their call signs, broadcast frequencies, cities of license, licensees, or programming formats. Call City of [3] Frequency [1][2] Licensee Format sign License KACU 89.7 FM Abilene Abilene Christian University Public Radio KAGT 90.5 FM Abilene Educational Media Foundation Contemporary Christian KAQD 91.3 FM Abilene American Family Association Southern Gospel KEAN- Townsquare Media Abilene 105.1 FM Abilene Country FM License, LLC Townsquare Media Abilene KEYJ-FM 107.9 FM Abilene Modern Rock License, LLC KGNZ 88.1 FM Abilene Christian Broadcasting Co., Inc. News, Christian KKHR 106.3 FM Abilene Canfin Enterprises, Inc. Tejano Townsquare Media Abilene KMWX 92.5 FM Abilene Adult Contemporary License, LLC Townsquare Media Abilene KSLI 1280 AM Abilene License, LLC Townsquare Media Abilene KULL 100.7 FM Abilene Classic Hits License, LLC Call City of [3] Frequency [1][2] Licensee Format sign License KVVO-LP 94.1 FM Abilene New Life Temple KWKC 1340 AM Abilene Canfin Enterprises, Inc. News/Talk Townsquare Media Abilene KYYW 1470 AM Abilene News/Talk License, LLC KZQQ 1560 AM Abilene Canfin Enterprises, Inc. Sports Talk KDLP-LP 104.7 FM Ace Ace Radio Inc. BPM RGV License Company, KJAV 104.9 FM Alamo Adult Hits L.P. KDRY 1100 AM Alamo Heights KDRY Radio, Inc. Christian Teaching & Preaching KQOS 91.7 FM Albany La Promesa Foundation KIFR 88.3 FM Alice Family Stations, Inc. -

FM-1949-07.Pdf
MM partl DIRECTORY BY OPL, SYSTEMS COUNTY U POLICE 1S1pP,TE FIRE FORESTRYOpSp `p` O COMPANIES TO REVISED LISTINGS 1, 1949 4/ka feeZ means IessJnterference ... AT HEADQUARTERS THE NEW RCA STATION RECEIVER Type CR -9A (152 -174 Mc) ON THE ROAD THE NEW RCA CARFONE Mobile 2 -way FM radio, 152 -174 Mc ...you get the greatest selectivity with RCA's All -New Communication Equipment You're going to hear a lot about selectivity from potentially useful channels for mobile radio communi- now on. In communication systems, receiver selectiv- cation systems. ity, more than any other single factor, determines the For degree of freedom from interference. complete details on the new RCA Station Re- This is impor- ceiver type CR -9A, tant both for today and for the future. and the new RCA CARFONE for mobile use, write today. RCA engineers are at your Recognizing this fact, RCA has taken the necessary service for consultation on prob- steps to make its all -new communication equipment lems of coverage, usage, or com- the most selective of any on the market today. To the plex systems installations. Write user, this means reliable operation substantially free Dept. 38 C. from interference. In addition, this greater selectivity Free literature on RCA's All -New now rhakes adjacent -channel operation a practical Communication Equipment -yours possibility - thereby greatly increasing the number of for the asking. COMMUN /CAT/ON SECT/ON RADIO CORPORATION of AMERICA ENGINEERING PRODUCTS DEPARTMENT, CAMDEN, N.J. In Canada: R C A VICTOR Company limited, Montreal Á#ofher s with 8(11(011' DlNews ERIE'S FIRST TV STATION Says EDWARD LAMB, publisher of "The Erie Dis- telecasting economics. -

For Public Inspection Comprehensive
REDACTED – FOR PUBLIC INSPECTION COMPREHENSIVE EXHIBIT I. Introduction and Summary .............................................................................................. 3 II. Description of the Transaction ......................................................................................... 4 III. Public Interest Benefits of the Transaction ..................................................................... 6 IV. Pending Applications and Cut-Off Rules ........................................................................ 9 V. Parties to the Application ................................................................................................ 11 A. ForgeLight ..................................................................................................................... 11 B. Searchlight .................................................................................................................... 14 C. Televisa .......................................................................................................................... 18 VI. Transaction Documents ................................................................................................... 26 VII. National Television Ownership Compliance ................................................................. 28 VIII. Local Television Ownership Compliance ...................................................................... 29 A. Rule Compliant Markets ............................................................................................ -

FY 2004 AM and FM Radio Station Regulatory Fees
FY 2004 AM and FM Radio Station Regulatory Fees Call Sign Fac. ID. # Service Class Community State Fee Code Fee Population KA2XRA 91078 AM D ALBUQUERQUE NM 0435$ 425 up to 25,000 KAAA 55492 AM C KINGMAN AZ 0430$ 525 25,001 to 75,000 KAAB 39607 AM D BATESVILLE AR 0436$ 625 25,001 to 75,000 KAAK 63872 FM C1 GREAT FALLS MT 0449$ 2,200 75,001 to 150,000 KAAM 17303 AM B GARLAND TX 0480$ 5,400 above 3 million KAAN 31004 AM D BETHANY MO 0435$ 425 up to 25,000 KAAN-FM 31005 FM C2 BETHANY MO 0447$ 675 up to 25,000 KAAP 63882 FM A ROCK ISLAND WA 0442$ 1,050 25,001 to 75,000 KAAQ 18090 FM C1 ALLIANCE NE 0447$ 675 up to 25,000 KAAR 63877 FM C1 BUTTE MT 0448$ 1,175 25,001 to 75,000 KAAT 8341 FM B1 OAKHURST CA 0442$ 1,050 25,001 to 75,000 KAAY 33253 AM A LITTLE ROCK AR 0421$ 3,900 500,000 to 1.2 million KABC 33254 AM B LOS ANGELES CA 0480$ 5,400 above 3 million KABF 2772 FM C1 LITTLE ROCK AR 0451$ 4,225 500,000 to 1.2 million KABG 44000 FM C LOS ALAMOS NM 0450$ 2,875 150,001 to 500,000 KABI 18054 AM D ABILENE KS 0435$ 425 up to 25,000 KABK-FM 26390 FM C2 AUGUSTA AR 0448$ 1,175 25,001 to 75,000 KABL 59957 AM B OAKLAND CA 0480$ 5,400 above 3 million KABN 13550 AM B CONCORD CA 0427$ 2,925 500,000 to 1.2 million KABQ 65394 AM B ALBUQUERQUE NM 0427$ 2,925 500,000 to 1.2 million KABR 65389 AM D ALAMO COMMUNITY NM 0435$ 425 up to 25,000 KABU 15265 FM A FORT TOTTEN ND 0441$ 525 up to 25,000 KABX-FM 41173 FM B MERCED CA 0449$ 2,200 75,001 to 150,000 KABZ 60134 FM C LITTLE ROCK AR 0451$ 4,225 500,000 to 1.2 million KACC 1205 FM A ALVIN TX 0443$ 1,450 75,001 -

Primary & Secondary Sources
Primary & Secondary Sources Brands & Products Agencies & Clients Media & Content Influencers & Licensees Organizations & Associations Government & Education Research & Data Multicultural Media Forecast 2019: Primary & Secondary Sources COPYRIGHT U.S. Multicultural Media Forecast 2019 Exclusive market research & strategic intelligence from PQ Media – Intelligent data for smarter business decisions In partnership with the Alliance for Inclusive and Multicultural Marketing at the Association of National Advertisers Co-authored at PQM by: Patrick Quinn – President & CEO Leo Kivijarv, PhD – EVP & Research Director Editorial Support at AIMM by: Bill Duggan – Group Executive Vice President, ANA Claudine Waite – Director, Content Marketing, Committees & Conferences, ANA Carlos Santiago – President & Chief Strategist, Santiago Solutions Group Except by express prior written permission from PQ Media LLC or the Association of National Advertisers, no part of this work may be copied or publicly distributed, displayed or disseminated by any means of publication or communication now known or developed hereafter, including in or by any: (i) directory or compilation or other printed publication; (ii) information storage or retrieval system; (iii) electronic device, including any analog or digital visual or audiovisual device or product. PQ Media and the Alliance for Inclusive and Multicultural Marketing at the Association of National Advertisers will protect and defend their copyright and all their other rights in this publication, including under the laws of copyright, misappropriation, trade secrets and unfair competition. All information and data contained in this report is obtained by PQ Media from sources that PQ Media believes to be accurate and reliable. However, errors and omissions in this report may result from human error and malfunctions in electronic conversion and transmission of textual and numeric data. -

Texas Media Outlets
Texas Media Outlets Newswire’s Media Database provides targeted media outreach opportunities to key trade journals, publications, and outlets. The following records are related to traditional media from radio, print and television based on the information provided by the media. Note: The listings may be subject to change based on the latest data. ________________________________________________________________________________ Radio Stations 27. KAZI-FM [KAZI 88.7] 1. "Taste of Texas" with Lisa Christi 28. KBCY-FM [99.7FM KBCY] 2. Adam Bomb Nights 29. KBIM-FM [94.9 the Country Giant] 3. ALL REQUEST MUSIC FEED 30. KBNJ-FM [Life Changing] 4. BACK STAGE OL 31. KBNL-FM [Radio Manantial] 5. BANDYT BOY EMPIRE 32. KBPA-FM [103.5 Bob FM] 6. BEYOND THE BOOK 33. KBSO-FM [Texas Radio 94.7] 7. Bob Kingsley's Country Top 40 34. KBST-AM [K-Best AM 1490] 8. Bstraw & PaulyG Show 35. KBUK-FM [K-Buck] 9. CHILL OUT JAZZ 36. KBYG-AM [Big 1400 AM] 10. Chip Howard's Sports Talk 37. KCIX-FM [Mix 106] 11. Country Gold 38. KCKM-AM 12. Cyberline 39. KCPS-AM [KCPS 1150] 13. Datum Line w/ Bruce McCarthy 40. KCRS-FM [103.3 Kiss FM] 14. El Show de Raúl Brindis 41. KCUL-FM 15. Elvis Duran and The Morning Show 42. KCYY-FM [Y100] 16. Fishbowl Radio Network 43. KDET-AM [Community Radio] 17. High Plains Public Radio 44. KDKR-FM [KDKR 91.3] 18. JJ Show 45. KDRP-LP 19. K206CD-FM 46. KEOM-FM [Mesquite Schools Radio] 20. KAAM-AM [Legends 770: 47. KESN-FM [ESPN Dallas 103.3 FM] K-Double-AM] 48. -

Download Austin File Alphabetic List
Austin File Alphabetic List 13th Floor Elevators--See: BIOGRAPHY FILE - Roky Erickson M9300 16 S0300 1800 Restaurant & Bar R3800 (E) 1880s P7300 1886 Room H3200 (8) 1938 Radio Script P1400 (12) 1977 Bond Issue P7100 (3) 1980-1989 P8660 2-J's R3800 (T) 23rd Street Artists Market P1400 (39) 26 Doors S2300 (21) 311 Club S0300 (102) 35th & Jefferson Retail/Office Center B6824 (5) 35th Street Festival C1900 (15) 3M Corporation M0900 (41) 5 AM Studio M9385 (52) 501 Studios M8460 (75) 5604 Manor N1875 (14) 612 West R3800 (S) 64 Beds H2010 (2) 8 ½ Souvenirs M9300 (E) A Bon Chat, Bon Rat I1200 (16) "A Nostalgic Evening at the Grand Ole Driskill" H3200 (4) "A Traditional San Jacinto Day Celebration" L2710 (29s) A-Perm-O-Green Lawn Company G0800 (3) A. Mozart Fest M9383 (7) A.C.O.R.N. N1900 (26) AAA Bonding Company C9200 (2) Aaron's B5070 (5) Abattoir M8640 (2) Abbey Wedding Chapel, The (in general folder) W2300 (1) Abbott Laboratories Corporation M0900 (11) Abendmusik M9380 (9) Aber-Schultz Auto Supply Company A9910 (26) Abernathy Furniture Company F5000 (16) Ablanedo, Ralph 1978 M8900 (41) Abortion F0520 (1) Academy for Educational Development E0600 (2) Academy Surplus D1100 (24) Accent Gallery A6400 (105) Accent Travel T7900 (6) ACCESS (Austin Collaborative of Cultural & Educational Sites & Schools) P8200 (83) Ace Custom Tailors C5230 (22) Achievement Scores P8200 (15) Achilles Grocery G4200 (91) Ackermann, Frieda and Hans W5700 (5) Acme Life Insurance Company I1150 (2) Acquisitions L2710 (29a) Acquisitions L2710 (29r) Act Against Violence Community -

ESTADOS UNIDOS MEXICANOS Y EL GOBIERNO DE LOS ESTADOS UNIDOS DE AMERICA RELATIVO AL SERVICIO DE RADIODIFUSION EN FM EN LA BANDA DE 88 a 108 Mhz
ACUERDO ENTRE EL GOBIERNO DE LOS ESTADOS UNIDOS MEXICANOS Y EL GOBIERNO DE LOS ESTADOS UNIDOS DE AMERICA RELATIVO AL SERVICIO DE RADIODIFUSION EN FM EN LA BANDA DE 88 A 108 MHz. El Gobierno de los Estados Unidos Mexicanos y el Gobierno de los Estados Unidos de América, las Partes, deseando continuar su mutuo entendimiento y cooperación concerniente a la radiodifusión en FM y reconociendo el derecho soberano de ambos países en el manejo de sus telecomunicaciones; tomando en cuenta las disposiciones del Artículo 31 del Convenio Internacional de Telecomunicaciones Nairobi, 1982, y el Artículo 7 del Reglamento de Radiocomunicaciones (Edición 1982), considerado como anexo al Convenio antes mencionado; a fin de proteger las estaciones de radiodifusión de los dos países; y deseando mejorar la utilización de la banda de frecuencias de 88 a 108 MHz atribuida a este servicio; Han acordado lo siguiente: ARTICULO 1 Definiciones Para el propósito de este Acuerdo, los términos definidos en el Reglamento de Radiocomunicaciones se aplicarán, excepto para las siguientes definiciones específicas: Administración: La Dirección General de Normas de Sistemas de Difusión de la Secretaría de Comunicaciones y Transportes de los Estados Unidos Mexicanos y la Federal Communications Commission, de los Estados Unidos de América; Acuerdo: Este Acuerdo y sus Anexos; Adjudicación: Provisión para el uso de un canal específico, identificado con una población o localidad en particular, la cual está protegida, sobre la base de sus parámetros máximos permitidos, de adjudicaciones