Virtual Exploration of Safe Entry Zones in the Brainstem: Comprehensive Definition And
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Telovelar Approach to the Fourth Ventricle: Microsurgical Anatomy
J Neurosurg 92:812–823, 2000 Telovelar approach to the fourth ventricle: microsurgical anatomy ANTONIO C. M. MUSSI, M.D., AND ALBERT L. RHOTON, JR., M.D. Department of Neurological Surgery, University of Florida, Gainesville, Florida Object. In the past, access to the fourth ventricle was obtained by splitting the vermis or removing part of the cere- bellum. The purpose of this study was to examine the access to the fourth ventricle achieved by opening the tela cho- roidea and inferior medullary velum, the two thin sheets of tissue that form the lower half of the roof of the fourth ven- tricle, without incising or removing part of the cerebellum. Methods. Fifty formalin-fixed specimens, in which the arteries were perfused with red silicone and the veins with blue silicone, provided the material for this study. The dissections were performed in a stepwise manner to simulate the exposure that can be obtained by retracting the cerebellar tonsils and opening the tela choroidea and inferior medullary velum. Conclusions. Gently displacing the tonsils laterally exposes both the tela choroidea and the inferior medullary velum. Opening the tela provides access to the floor and body of the ventricle from the aqueduct to the obex. The additional opening of the velum provides access to the superior half of the roof of the ventricle, the fastigium, and the superolater- al recess. Elevating the tonsillar surface away from the posterolateral medulla exposes the tela, which covers the later- al recess, and opening this tela exposes the structure forming -

Auditory and Vestibular Systems Objective • to Learn the Functional
Auditory and Vestibular Systems Objective • To learn the functional organization of the auditory and vestibular systems • To understand how one can use changes in auditory function following injury to localize the site of a lesion • To begin to learn the vestibular pathways, as a prelude to studying motor pathways controlling balance in a later lab. Ch 7 Key Figs: 7-1; 7-2; 7-4; 7-5 Clinical Case #2 Hearing loss and dizziness; CC4-1 Self evaluation • Be able to identify all structures listed in key terms and describe briefly their principal functions • Use neuroanatomy on the web to test your understanding ************************************************************************************** List of media F-5 Vestibular efferent connections The first order neurons of the vestibular system are bipolar cells whose cell bodies are located in the vestibular ganglion in the internal ear (NTA Fig. 7-3). The distal processes of these cells contact the receptor hair cells located within the ampulae of the semicircular canals and the utricle and saccule. The central processes of the bipolar cells constitute the vestibular portion of the vestibulocochlear (VIIIth cranial) nerve. Most of these primary vestibular afferents enter the ipsilateral brain stem inferior to the inferior cerebellar peduncle to terminate in the vestibular nuclear complex, which is located in the medulla and caudal pons. The vestibular nuclear complex (NTA Figs, 7-2, 7-3), which lies in the floor of the fourth ventricle, contains four nuclei: 1) the superior vestibular nucleus; 2) the inferior vestibular nucleus; 3) the lateral vestibular nucleus; and 4) the medial vestibular nucleus. Vestibular nuclei give rise to secondary fibers that project to the cerebellum, certain motor cranial nerve nuclei, the reticular formation, all spinal levels, and the thalamus. -

Pediatric Hydrocephalus; a Statistical and Historical Approach by R
Global Journal of Medical Research: A Neurology and Nervous System Volume 15 Issue 1 Version 1.0 Year 2015 Type: Double Blind Peer Reviewed International Research Journal Publisher: Global Journals Inc. (USA) Online ISSN: 2249-4618 & Print ISSN: 0975-5888 Pediatric Hydrocephalus; A Statistical and Historical Approach By R. Omidi-Varmezani University of Spital Buelach- Zurich, Switzerland Abstract- Purpose: The purpose of this study was to determine the clinical statistical collection of pediatric hydrocephalus with emphasis on pathology to investigate the epidemiology of pediatric hydrocephalus. Materials and Methods: We performed respectively analysis of the pediatric patients younger than 18 years with or suspected of hydrocephalus in our neuropediatric centre since 2001. Data were obtained from our neuropediatric centre database and from hospital admission records of the university hospital of Homburg. After the patient selection procedure and sort out the hydrocephalus patients were a total of 193 children registered at the University Hospital of Homburg Children Medical Centre, between June 2001 and March 2009. The patients were under age and mechanism of hydrocephalus distributed. Keywords: hydrocephalus, peditric neuroradiology, intracerebral pressure. GJMR-A Classification : NLMC Code: WM 170 PediatricHydrocephalusAStatisticalandHistoricalApproach Strictly as per the compliance and regulations of: © 2015. R. Omidi-Varmezani. This is a research/review paper, distributed under the terms of the Creative Commons Attribution- Noncommercial 3.0 Unported License http://creativecommons.org/licenses/by-nc/3.0/), permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. Pediatric Hydrocephalus; A Statistical and Historical Approach R. Omidi-Varmezani Abstract- Purpose: The purpose of this study was to determine can flow from the 4th ventricle into the subarachnoidal the clinical statistical collection of pediatric hydrocephalus with space through two apertures. -

Lipoma of the Midbrain
LIPOMA OF THE MIDBRAIN POST-MORTEM FINDING IN A PATIENT WITH BREAST CANCER VERÔNICA MAIA GOUVEA * — MYRIAM DUMAS HAHN ** — LEILA CHIMELLI ** SUMMARY — Intracranial lipomas are rare, usually do not have clinical expression and are located mare frequently in the corpus callosum. Other locations include the spinal cord, midbrain tectum, superior vermis, tuber cinereum, infundibulum and more rarely cerebello pontine angle, hypothalamus, superior medullary velum and insula. We report the case of a lipoma of the left inferior colliculus which was a post-mortem finding in a woman who died of breast cancer. Although there are reports of intracranial lipomas in patients with malignant tumors there is no explanation for the co-existence of the two tumors. The present tumor also includes a segment of a nerve which is not uncommon, but a less common finding was the presence of nests of Schwann cells within it, shown by immunohistochemistry. Lipoma do mesencéfalo: achado de necrópsia, em paciente com câncer da mama. RESUMO — Lipomas intracranianos são raros, em geral sem expressão clínica, localizados mais freqüentemente no corpo caloso. Outras localizações incluem medula espinhal, teto mesencefálico, vermis superior, tuber cinereum, infundibulum e mais raramente o ângulo ponto-cerebelar, hipotálamo, véu medular superior e insula. Relatamos o achado de necrópsia de um lipoma do colículo inferior esquerdo em uma mulher com câncer de mama. Embora haja relatos de lipomas intracranianos em pacientes com tumores malignos não há explicação para a co-existência dos dois tumores. O presente tumor também inclui o segmento de um nervo, o que não é incomum, mas um achado menos comum foi a presença de ninhos de células de Schwann no tumor, mostradas por imuno-histoquímica. -
Locus Coeruleus Complex of the Family Delphinidae
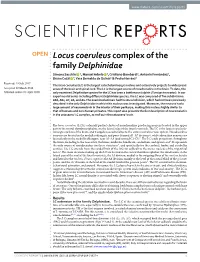
www.nature.com/scientificreports OPEN Locus coeruleus complex of the family Delphinidae Simona Sacchini 1, Manuel Arbelo 1, Cristiano Bombardi2, Antonio Fernández1, Bruno Cozzi 3, Yara Bernaldo de Quirós1 & Pedro Herráez1 Received: 19 July 2017 The locus coeruleus (LC) is the largest catecholaminergic nucleus and extensively projects to widespread Accepted: 22 March 2018 areas of the brain and spinal cord. The LC is the largest source of noradrenaline in the brain. To date, the Published: xx xx xxxx only examined Delphinidae species for the LC has been a bottlenose dolphin (Tursiops truncatus). In our experimental series including diferent Delphinidae species, the LC was composed of fve subdivisions: A6d, A6v, A7, A5, and A4. The examined animals had the A4 subdivision, which had not been previously described in the only Delphinidae in which this nucleus was investigated. Moreover, the neurons had a large amount of neuromelanin in the interior of their perikarya, making this nucleus highly similar to that of humans and non-human primates. This report also presents the frst description of neuromelanin in the cetaceans’ LC complex, as well as in the cetaceans’ brain. Te locus coeruleus (LC) is a densely packed cluster of noradrenaline-producing neurons located in the upper part of the rostral rhombencephalon, on the lateral edge of the fourth ventricle. Te LC is the largest catechola- minergic nucleus of the brain, and it supplies noradrenaline to the entire central nervous system. Noradrenaline neurons are located in the medulla oblongata and pons (termed A1-A7 divisions), while adrenaline neurons are located only in the medulla oblongata, near A1-A3 (and termed C1-C3)1. -

Anatomy of the Brainstem
Anatomy of the Brainstem Neuroanatomy block-Anatomy-Lecture 5 Editing file Objectives At the end of the lecture, students should be able to: 01 List the components of brain stem. 02 Describe the site of brain stem 03 Describe the relations between components of brain stem & their relations to cerebellum. 04 Describe the external features of both ventral & dorsal surfaces of brain stem Color guide 05 List cranial nerves emerging from brain stem 06 Describe the site of emergence of each cranial nerve ● Only in boys slides in Green ● Only in girls slides in Purple ● important in Red ● Notes in Grey Development of Brain Brain stem ● The brain develops from the cranial part of neural tube. ● The brainstem is the region of the brain that connects the ● The cranial part is divided into 3 parts: cerebrum with the spinal cord. ● Site: It lies on the basilar part of occipital bone (clivus). - Subdivided into: ● Parts from above downwards : 1. Telencephalon: (cavities: 2 lateral ventricles) 1. Midbrain Two cerebral hemispheres. Forebrain 2. Pons 2. Diencephalon: (cavity: 3rd ventricle) 3. Medulla oblongata thalamus, hypothalamus, epithalamus & subthalamus ● Connection with cerebellum: Each part of the brain stem is connected to the Midbrain - (cavity: cerebral aqueduct) cerebellum by cerebellar peduncles (superior, middle & inferior). - (cavity: 4th ventricle) - Subdivided into: Hindbrain 1. Pons 2. Cerebellum 3. Medulla oblongata 3 Sagittal section of Brain 4 Functions of the Brain Stem Pathway of tracts between cerebral cortex & spinal cord (ascending and descending tracts). 1 Site of origin of nuclei of cranial nerves (from 3rd to 12th). 2 Site of emergence of cranial nerves (from 3rd to 12th). -

Brainstem and Its Associated Cranial Nerves
Brainstem and its Associated Cranial Nerves Anatomical and Physiological Review By Sara Alenezy With appreciation to Noura AlTawil’s significant efforts Midbrain (Mesencephalon) External Anatomy of Midbrain 1. Crus Cerebri (Also known as Basis Pedunculi or Cerebral Peduncles): Large column of descending “Upper Motor Neuron” fibers that is responsible for movement coordination, which are: a. Frontopontine fibers b. Corticospinal fibers Ventral Surface c. Corticobulbar fibers d. Temporo-pontine fibers 2. Interpeduncular Fossa: Separates the Crus Cerebri from the middle. 3. Nerve: 3rd Cranial Nerve (Oculomotor) emerges from the Interpeduncular fossa. 1. Superior Colliculus: Involved with visual reflexes. Dorsal Surface 2. Inferior Colliculus: Involved with auditory reflexes. 3. Nerve: 4th Cranial Nerve (Trochlear) emerges caudally to the Inferior Colliculus after decussating in the superior medullary velum. Internal Anatomy of Midbrain 1. Superior Colliculus: Nucleus of grey matter that is associated with the Tectospinal Tract (descending) and the Spinotectal Tract (ascending). a. Tectospinal Pathway: turning the head, neck and eyeballs in response to a visual stimuli.1 Level of b. Spinotectal Pathway: turning the head, neck and eyeballs in response to a cutaneous stimuli.2 Superior 2. Oculomotor Nucleus: Situated in the periaqueductal grey matter. Colliculus 3. Red Nucleus: Red mass3 of grey matter situated centrally in the Tegmentum. Involved in motor control (Rubrospinal Tract). 1. Inferior Colliculus: Nucleus of grey matter that is associated with the Tectospinal Tract (descending) and the Spinotectal Tract (ascending). Tectospinal Pathway: turning the head, neck and eyeballs in response to a auditory stimuli. 2. Trochlear Nucleus: Situated in the periaqueductal grey matter. Level of Inferior 3. -

Morphometric Assesment of the External Anatomy of Fourth Ventricle and Dorsal Brainstem in Fresh Cadavers
DOI: 10.5137/1019-5149.JTN.24942-18.1 Turk Neurosurg 29(3):445-450, 2019 Received: 26.09.2018 / Accepted: 20.11.2018 Published Online: 19.12.2018 Original Investigation Morphometric Assesment of the External Anatomy of Fourth Ventricle and Dorsal Brainstem in Fresh Cadavers Veysel ANTAR1, Okan TURK1, Salim KATAR2, Mahmut OZDEN3, Balkan SAHIN4, Sahin YUCELI5, Erdogan KARA6, Ayse YURTSEVEN6 1Istanbul Training and Research Hospital, Department of Neurosurgery, Istanbul, Turkey 2Selahattin Eyyubi City Hospital, Department of Neurosurgery, Diyarbakir, Turkey 3Bahcesehir University, Department of Neurosurgery, Istanbul, Turkey 4Sultan Abdulhamit Han Training and Research Hospital, Department of Neurosurgery, Istanbul, Turkey 5Erzincan Neon Hospital, Department of Neurosurgery, Erzincan, Turkey 6Ministry of Justice, Council of Forensic Medicine, Istanbul, Turkey Corresponding author: Veysel ANTAR [email protected] ABSTRACT AIM: To investigate the external anatomy of the fourth ventricle and dorsal brainstem using morphometric data, which could be useful for preoperative surgical planning. MATERIAL and METHODS: Between January 2017 and December 2017, 42 fresh adult cadavers were investigated for the measurements of the cadaver brainstems and fourth ventricle, and they were recorded by photography. Measurements were evaluated according to body mass indexes (BMIs) of the patients. We also investigate the visualization of facial colliculus and stria medullaris on brainstem. RESULTS: A total of 42 fresh cadavers with a mean age of 45.38 ± 16.41 years old were included in this research. We found no statistically significant difference between measurements and BMIs. Facial colliculus was visualized in 92.9% (n=39), but it could not visualized in 7.1% (n=3) of the subjects. -

NIH Public Access Author Manuscript Neuromodulation
NIH Public Access Author Manuscript Neuromodulation. Author manuscript; available in PMC 2015 June 01. NIH-PA Author ManuscriptPublished NIH-PA Author Manuscript in final edited NIH-PA Author Manuscript form as: Neuromodulation. 2014 June ; 17(4): 312–319. doi:10.1111/ner.12141. Surgical Neuroanatomy and Programming in Deep Brain Stimulation for Obsessive Compulsive Disorder Takashi Morishita, M.D., Ph.D.1, Sarah M. Fayad, M.D.2, Wayne K. Goodman, M.D.3, Kelly D. Foote, M.D.1, Dennis Chen, B.S.2, David A. Peace, M.S., CMI1, Albert L. Rhoton Jr.1, and Michael S. Okun, M.D.1,2 1Department of Neurosurgery, University of Florida College of Medicine/Shands Hospital, Center for Movement Disorders and Neurorestoration, McKnight Brain Institute, Gainesville, FL Corresponding Author: Takashi Morishita, M.D., Ph.D., Department of Neurosurgery, Mcknight Brain Institute Room L2-100, 1149 South Newell Drive, Gainesville, FL 32611, 352-273-9000, 352-392-8413 FAX, [email protected]. Authorship Statement: Drs. Morishita and Okun deigned and conducted the study, including patient recruitment, data collection and data analysis. Drs. Morishita and Fayad prepared the manuscript draft with important intellectual input from Drs. Okun, Rhoton, Goodman and Foote. Mr. Peace provided his illustration into this manuscript. Mr. Chen contributed to collect the data. All authors approved the final manuscript. Author disclosures 1. Takashi Morishita, M.D., Ph.D. Disclosures: Dr. Morishita has received grant support from Nakatomi foundation, St. Luke’s Life Science Institute of Japan, and Japan Society for Promotion of Science in Japan. 2. Sarah M. -

The Three-Dimensional Architecture of the Internal Capsule of the Human Brain Demonstrated by Fiber Dissection Technique
ARS Medica Tomitana - 2014; 3(78): 115 -122 10.2478/arsm-2014-0021 Goga Cristina1,2,3, Brinzaniuc Klara1, Florian I.S.2, Rodriguez Mena R.3 The three-dimensional architecture of the internal capsule of the human brain demonstrated by fiber dissection technique 1. University of Medicine and Pharmacy Tirgu Mures, Tirgu Mures, Romania, Department of Anatomy 2. Cluj County Emergency Hospital, Cluj Napoca, Romania, Department of Neurosurgery 3. Yeditepe University School of Medicine, Istanbul, Turkey, Department of Neurosurgery ABSTRACT Introduction The fiber dissection technique involves peeling away white matter fiber tracts of the brain to display its three-dimensional anatomic arrangement. The intricate three-dimensional configuration and structure of the internal capsule (IC) is not well defined. By using The white matter of the brain consists of the fiber dissection technique, our aim was to expose bundles of myelinated nerve fibers known as and study the IC to achieve a clearer conception of its fascicles or fiber tracts. There are three groups of configuration and relationships with neighboring white nerve fibers: association, connection and projection matter fibers and central nuclei. fibers. Association fibers connect neighboring The lateral and medial aspects of the temporal lobes of and distal cortical region in the same hemisphere. twenty, previously frozen, formalin-fixed human brains Commissural fibers connect homologues regions in were dissected under the operating microscope using the two hemispheres. Projection fibers connect the the fiber dissection technique. The details of the three-dimensional arrangement of the cerebral cortex with subcortical structures such as fibers within the IC were studied and a comprehensive thalamus, basal ganglia, brainstem and spinal cord. -
Internal Structure of the Brain Stem
INTERNAL STRUCTURE OF THE BRAIN STEM Done by: Lulwah Alturki Areej Alrajeh Revised by: Anjod Almuhareb هذا العمل ﻻ يعتبر مصدر رئيسي للمذاكرة وإنما للمرجعة فقط :تنويه [email protected] OBJECTIVES • Distinguish the internal structure of the components of the brain stem in different levels and the specific criteria of each level. • 1. Medulla oblongata (closed, mid and open medulla) • 2. Pons (caudal and rostral). • 3. Mid brain ( superior and inferior colliculi). • Describe the Reticular formation (structure, function and pathway) being an important content of the brain stem. Internal structures of medulla oblongata (closed) Medulla Mid Medulla (open) Medulla Caudal Rostral pyramid pyramid pyramid Spinal Nucleus of Gracile & Cuneate nuclei Inferior Olivary Nucleus Trigeminal (Trigeminal → Internal arcuate fibers Control of movement sensory nucleus): → sensory Decussation Medial longitudinal fasciculus continuation of Substantia Links vestibular nuclei with nuclei of extraocular ms.(3,4&6) to Gelatinosa help cordination head&eye movement Motor Decussation Medial leminiscus Lower part of floor of 4th ventricle By: pyramidal fibers ( ascending internal Inferior Cerebellar Peduncle arcuate fiber ) Connect M.O with cerebellum *un crossed fibers → thalamus Cochlear nuclei from the ventral Dorsal motor Nucleus of Vagus *Hypoglossal corticospinal tract. Nucleus Vestibular nuclei complex (equilibrium) Solitary Nucleus Receive taste sensation from tongue 7&9&10 medial lemniscus Nucleus Ambiguus :give motor f. to constrictor of pharynx & int.ms. Of larynx Internal structures of Pons CAUDAL PART ROSTRAL(cranial) PONS Trapezoid Body Superior Medullary Velum acoustic fibres from cochlear nuclei to ascend into midbrain as lateral lemniscus and terminate in inferior colliculus). pontocerebellar fibres pass to cerebllum through middle cerebellar peduncle pontine nuclei receive cortico pontine fibers. -

Seventh-And-A-Half Syndrome
Ophthalmology And Ophthalmic Surgery Open Access Case Report Seventh-and-a-Half Syndrome Ama Sadaka*, Shauna Berry and Andrew G Lee Department of Ophthalmology, Blanton Eye Institute, the Methodist Hospital, USA A R T I C L E I N F O A B S T R A C T Article history: Received: 04 September 2017 This is a case of a patient with right internuclear ophthalmoplegia and right Accepted: 05 October 2017 Published: 13 October 2017 peripheral seventh nerve palsy with no other neurologic deficits. Magnetic Keywords: resonance imaging showed a small localized right hemipons infarct involving Seven-and-a-half syndrome; INO facial motor nucleus and facial genu as well as the right medial longitudinal fasciculus. We introduce “Seven-and-a-half syndrome” as a new Copyright: ©2017 Sadaka A clinicoradiologic syndrome. Ophthalmol Ophthalmic Surg This is an open access article distributed Case Presentation under the Creative Commons Attribution License, which permits unrestricted use, A 68-year-old white female presented with sudden onset horizontal binocular distribution, and reproduction in any medium, provided the original work is diplopia and right-sided facial weakness involving the upper and lower face properly cited. consistent with a severe lower motor neuron seventh nerve palsy. Past medical Citation this article: Sadaka A, Berry S, Lee AG. Seventh-and-a-Half Syndrome. history was significant for uncontrolled hypertension and cerebral amyloid Ophthalmol Ophthalmic Surg. 2017; 1(1):112. angiopathy. No history of head trauma or infection. Visual acuity was 20/20 in both eyes. Pupils were equal and reactive with no relative afferent pupillary defect in either eye.