World Bank Document
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Department of Medical & Health Government of Uttar Pradesh
Department of Medical & Health Government of Uttar Pradesh LIST OF KEY MODIFICATIONS (PART OF CORRIGENDUM) FOR RFP for Selection of Free Diagnostic Service Providers For Select Locations in Uttar Pradesh Bid Ref. No. : SPMU/NHM/Procure./FDS/2016-17/21/03 16th September 2016 List of Key Modifications in Revised RFP for Selection of Free Diagnostics Service Provider in Select Locations of Uttar Pradesh Refer Change S. No. Existing Clause Modified Clause ence Description 1. IFB-3, Procedure to Bids will be invited on the basis of discount-percentage Bids will be invited on the basis of discount-percentage Page be followed contract based on the Central Government Health Scheme contract based on the Central Government Health Scheme 3 in case CGHS (CGHS) Delhi-NCR Circle, 2014 rates for NABL (CGHS) Delhi-NCR Circle, 2014 rates for NABL rates are not investigations. investigations. available or multiple • If the rates for some tests are not available in CGHS CGHS rates rate list, then the rates of such pathology tests in are available SGPGI/ KGMU/ any other medical college will be considered in that sequence. • It was decided that if any test appears in the CGHS list more than once, the lowest rate will be considered. CGHS rate list of Delhi and NCR for 2014 will be taken as authentic for reference value. The above clause is also applicable for: • BDS Clause 1.2 • BDS Clause 14 • BDS Clause 30 • Service Provider’s Bid • Letter of Acceptance • Form of Contract 2. IFB-6, Change of Contract signing and payment authority will be: Contract signing and payment authority will be: Page contract a. -

Ayodhya Page:- 1 Cent-Code & Name Exam Sch-Status School Code & Name #School-Allot Sex Part Group 1003 Canossa Convent Girls Inter College Ayodhya Buf
DATE:27-02-2021 BHS&IE, UP EXAM YEAR-2021 **** FINAL CENTRE ALLOTMENT REPORT **** DIST-CD & NAME :- 62 AYODHYA PAGE:- 1 CENT-CODE & NAME EXAM SCH-STATUS SCHOOL CODE & NAME #SCHOOL-ALLOT SEX PART GROUP 1003 CANOSSA CONVENT GIRLS INTER COLLEGE AYODHYA BUF HIGH BUF 1001 SAHABDEENRAM SITARAM BALIKA I C AYODHYA 73 F HIGH BUF 1003 CANOSSA CONVENT GIRLS INTER COLLEGE AYODHYA 225 F 298 INTER BUF 1002 METHODIST GIRLS INTER COLLEGE AYODHYA 56 F OTHER THAN SCICNCE INTER BUF 1003 CANOSSA CONVENT GIRLS INTER COLLEGE AYODHYA 109 F OTHER THAN SCICNCE INTER BUF 1003 CANOSSA CONVENT GIRLS INTER COLLEGE AYODHYA 111 F SCIENCE INTER CUM 1091 DARSGAH E ISLAMI INTER COLLEGE AYODHYA 53 F ALL GROUP 329 CENTRE TOTAL >>>>>> 627 1004 GOVT GIRLS I C GOSHAIGANJ AYODHYA AUF HIGH AUF 1004 GOVT GIRLS I C GOSHAIGANJ AYODHYA 40 F HIGH CRF 1125 VIDYA DEVIGIRLS I C ANKARIPUR AYODHYA 11 F HIGH CRM 1140 SARDAR BHAGAT SINGH HS BARAIPARA DULLAPUR AYODHYA 20 F HIGH CRM 1208 M D M N ARYA HSS R N M G GANJ AYODHYA 7 F HIGH CUM 1265 A R A IC K GADAR RD GOSAINGANJ AYODHYA 32 F HIGH CRM 1269 S S M HSS K G ROAD GOSHAINGANJ AYODHYA 26 F HIGH CRM 1276 IMAMIA H S S AMSIN AYODHYA 15 F HIGH AUF 5004 GOVT GIRLS I C GOSHAIGANJ AYODHYA 18 F 169 INTER AUF 1004 GOVT GIRLS I C GOSHAIGANJ AYODHYA 43 F OTHER THAN SCICNCE INTER CRF 1075 MADHURI GIRLS I C AMSIN AYODHYA 91 F OTHER THAN SCICNCE INTER CRF 1125 VIDYA DEVIGIRLS I C ANKARIPUR AYODHYA 7 F OTHER THAN SCICNCE INTER CRM 1138 AMIT ALOK I C BODHIPUR AMSIN AYODHYA 96 F OTHER THAN SCICNCE INTER CUM 1265 A R A IC K GADAR RD GOSAINGANJ AYODHYA 74 -

Village Name
Mission Antodaya Selected Villages List- 314 Faizabad S. No. Block Name GP Name Village Name 1 SOHAWAL BAIDRAPUR Gaura Kurmiyan 2 SOHAWAL BAIDRAPUR Bhawaniya Pur 3 SOHAWAL BAIDRAPUR Baidra Pur 4 SOHAWAL DHANNIPUR Budhauliya 5 SOHAWAL DHANNIPUR Dhannipur 6 SOHAWAL GOOPINATH PUR Gopinath Pur 7 SOHAWAL HARBANDHAN PUR Sarjupur Uparhar 8 SOHAWAL HARBANDHAN PUR Sarjupur Manjha 9 SOHAWAL HARBANDHAN PUR Thareru Uparhar 10 SOHAWAL HARBANDHAN PUR Thareru Manjha 11 SOHAWAL HARBANDHAN PUR Harbandhan Pur 12 SOHAWAL IBBRAHIMPUR KANDIE Ibrahimpur Kandie 13 SOHAWAL ISMAIL NAGAR SIHORA Ismil Nagar Siroha 14 SOHAWAL ISMAIL NAGAR SIHORA Dostpur Raghu Uparhar 15 SOHAWAL ISMAIL NAGAR SIHORA Dostpur Raghu Manjha 16 SOHAWAL ISMAIL NAGAR SIHORA Ismil Nagar Sirohi Uparhar 17 SOHAWAL KOLA Kola 18 SOHAWAL KOT DEEH SARAIYAN Kotdeeh Sarraiya 19 SOHAWAL PARANA PUR Parana Pur 20 SOHAWAL TAHSEENPUR Tahasin Pur 21 SOHAWAL DINKARPUR Dinkar Pur 22 MASODHA BHADARSA BAHAR Bhadersa Ta. Bahar 23 MASODHA KADIPUR Kadipur 24 MASODHA KADIPUR Bandi Daspur 25 MASODHA KAIL Kail 26 MASODHA KALLYAN PUR BHADRASSA Kaliyan Pur Bhaderash 27 MASODHA KHOJANPUR Khojn Pur (CT) 28 MASODHA MANA PUR Kharag Pur 29 MASODHA MANA PUR Manapur 30 MASODHA NANDI GRAM Nandigram 31 MASODHA PAHARGANJ Pahar Ganj (CT) 32 MASODHA PALIYA GOA Paliagoa 33 MASODHA PALYA SHAHVADI Paliya Shahzadi 34 MASODHA SARAIYA Saraiya 35 MASODHA SATHARI Sathri 36 MASODHA TONIYA Toniya 37 MASODHA FIROJPUR UPARHAR Firozpur Manjha 38 MASODHA FIROJPUR UPARHAR Firozpur Uparhar 39 MASODHA SAKHUPARA Sakhupara 40 PURA BAZAR ANJANA -
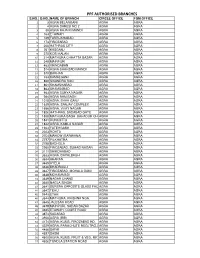
TOTAL PPF BRANCHES.Xlsx
PPF AUTHORISED BRANCHES S.NO. D.NO. NAME OF BRANCH CIRCLE OFFICE FGM OFFICE 1 3 AGRA BELANGANJ AGRA AGRA 2 4 AGRA DARESI NO 2 AGRA AGRA 3 30 AGRA RAJA KI MANDI AGRA AGRA 4 163 ETAWAH AGRA AGRA 5 169 FARRUKHABAD AGRA AGRA 6 173 FIROZABAD AGRA AGRA 7 200 HATHRAS CITY AGRA AGRA 8 261 KASGANJ AGRA AGRA 9 270 KOSI KALAN AGRA AGRA 10 314 MATHURA CHHATTA BAZAR AGRA AGRA 11 348 MAINPURI AGRA AGRA 12 463 VRINDABAN AGRA AGRA 13 514 AGRA SHAHZADI MANDI AGRA AGRA 14 570 BARHAN AGRA AGRA 15 733 KAMALGANJ AGRA AGRA 16 860 SIKANDRA RAO AGRA AGRA 17 861 SHAMSHABAD AGRA AGRA 18 863 SHAMSABAD AGRA AGRA 19 983 AGRA SURYA NAGAR AGRA AGRA 20 984 AGRA RAM BAGH AGRA AGRA 21 1018 AGRA, SHAH GANJ AGRA AGRA 22 1639 AGRA, SANJAY COMPLEX AGRA AGRA 23 1656 AGRA, VIJAY NAGAR AGRA AGRA 24 1826 HATHRAS, SADABAD GATE AGRA AGRA 25 1838 MATHURA BAGH BAHADUR CHOWKAGRA AGRA 26 1841 RUNKUTTA AGRA AGRA 27 1842 AGRA, KAMLA NAGAR AGRA AGRA 28 1934 FATEHGARH AGRA AGRA 29 2023 ROHTA AGRA AGRA 30 2754 MAHOW (BARWANA) AGRA AGRA 31 2797 PILKHATRA AGRA AGRA 32 2798 BADHOLA AGRA AGRA 33 2960 FIROZABAD, SUHAG NAGAR AGRA AGRA 34 3111 SHIKOHABAD AGRA AGRA 35 3633 AGRA, DAYALBAGH AGRA AGRA 36 3634 AHARAN AGRA AGRA 37 3635 AYELA AGRA AGRA 38 3636 BHADRAULI AGRA AGRA 39 3637 FIROZABAD, MOHALA GANJ AGRA AGRA 40 3638 MOHAMMADI AGRA AGRA 41 3639 NAGAR CHAND AGRA AGRA 42 3640 NAGLA SINGHI AGRA AGRA 43 3641 SURERA OPPOSITE GLASS FACTORYAGRA AGRA 44 3642 TEHU AGRA AGRA 45 3643 ETAH AGRA AGRA 46 3644 MATHURA, KRISHNA NGR. -

Annexure-V State/Circle Wise List of Post Offices Modernised/Upgraded
State/Circle wise list of Post Offices modernised/upgraded for Automatic Teller Machine (ATM) Annexure-V Sl No. State/UT Circle Office Regional Office Divisional Office Name of Operational Post Office ATMs Pin 1 Andhra Pradesh ANDHRA PRADESH VIJAYAWADA PRAKASAM Addanki SO 523201 2 Andhra Pradesh ANDHRA PRADESH KURNOOL KURNOOL Adoni H.O 518301 3 Andhra Pradesh ANDHRA PRADESH VISAKHAPATNAM AMALAPURAM Amalapuram H.O 533201 4 Andhra Pradesh ANDHRA PRADESH KURNOOL ANANTAPUR Anantapur H.O 515001 5 Andhra Pradesh ANDHRA PRADESH Vijayawada Machilipatnam Avanigadda H.O 521121 6 Andhra Pradesh ANDHRA PRADESH VIJAYAWADA TENALI Bapatla H.O 522101 7 Andhra Pradesh ANDHRA PRADESH Vijayawada Bhimavaram Bhimavaram H.O 534201 8 Andhra Pradesh ANDHRA PRADESH VIJAYAWADA VIJAYAWADA Buckinghampet H.O 520002 9 Andhra Pradesh ANDHRA PRADESH KURNOOL TIRUPATI Chandragiri H.O 517101 10 Andhra Pradesh ANDHRA PRADESH Vijayawada Prakasam Chirala H.O 523155 11 Andhra Pradesh ANDHRA PRADESH KURNOOL CHITTOOR Chittoor H.O 517001 12 Andhra Pradesh ANDHRA PRADESH KURNOOL CUDDAPAH Cuddapah H.O 516001 13 Andhra Pradesh ANDHRA PRADESH VISAKHAPATNAM VISAKHAPATNAM Dabagardens S.O 530020 14 Andhra Pradesh ANDHRA PRADESH KURNOOL HINDUPUR Dharmavaram H.O 515671 15 Andhra Pradesh ANDHRA PRADESH VIJAYAWADA ELURU Eluru H.O 534001 16 Andhra Pradesh ANDHRA PRADESH Vijayawada Gudivada Gudivada H.O 521301 17 Andhra Pradesh ANDHRA PRADESH Vijayawada Gudur Gudur H.O 524101 18 Andhra Pradesh ANDHRA PRADESH KURNOOL ANANTAPUR Guntakal H.O 515801 19 Andhra Pradesh ANDHRA PRADESH VIJAYAWADA -

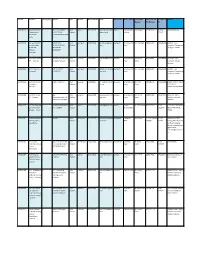
2019-May-8-Ec-Sultanpur.Pdf
! 1 I~0 .•....~ .•.... j ij .~ ~!~ i·i.. ~ ~ ~ ~h~2~1~!S6 EXECUTIVE SUMMARY SULTANPUR Besed or tne /,,[to5t oata refresh on Mar 2019, S,lltanpur stands at a ra+ d 48 out of 75 districts ":vi:t' 3 ccnocsite score 0' 0,44. Sutanpur's Ut:,t oerfOI'l'i ng .ndtcetor IS % of pregnant women received 4 or more ANC and tested for Hb against estimated PWwhen? II IS ranked 1/75 dtstnrts Wltl, a 5COIt2 ')' 100.00. The next nest perfcrrrmg indicators % of children received full immunization (BCG,Penta 1,2,3, Measles)where Sultanpur is ranked at . /75 w.th a score 0' 100.00 Jajsinghpur, PP Kamaicha, Dubeypur ,ire fie :CJ) pe"'orming blorxs wrt CC"1!)cslte score. Su!tanpur, DHQ Sultanpur, Kurebhar ere +e em pertormng blocr5 wrt (C"1!)C'5!te score. CQI',l?OS -E SCC'\, R!,N< ,'-0 :2:)" INDICATOR PERFORMANCE CHANGE Rf .~ \/:;i..C -6 -: o~r- "e~rar'c v.cr-er "cce .ec .: or me "-: L.i\C 8( :1 :.:s:e:l ;c" - ~ f g?ir:;:t estimetec C ,\ 1175 100.00 0.44 t6- -: -0; C·~tc:ic'" oe . e""j ~26 "':t repc":ed ~ei'.e·'ii I~:: ,:,(:is'i!a;~e:o c...C) i48175 40175 0.48 ·'",6-1::',; "e', :u, ';~-:, ., ~:1C:t~~'~:~~~~I~e:el"~,?JJs:parn :'-e-:·- .,j:'" ~'::'8 r,:.'" cf ~cr'''e celtver, cgair.:;: "e~,j":e: celi ..er/{~ofTle 63175 19.25 TOP 3 PERFORMANCE BLOCKS i' ::0' e!i~ole coup t ac:to:e:llil11:"~ 'T,t:rc':, :·,1io 00 tee. -
ITI Code ITI Name ITI Category Address State District Phone Number Email Name of FLC Name of Bank Name of FLC Mobile No
ITI Code ITI Name ITI Category Address State District Phone Number Email Name of FLC Name of Bank Name of FLC Mobile No. Of Landline of Address Manager FLC Manager FLC GR09000145 Karpoori Thakur P VILL POST GANDHI Uttar Ballia 9651744234 karpoorithakur1691 Ballia Central Bank N N Kunwar 9415450332 05498- Haldi Kothi,Ballia Dhanushdhari NAGAR TELMA Pradesh @gmail.com of India 225647 Private ITC - JAMALUDDINPUR DISTT Ballia B GR09000192 Sar Sayed School P OHDARIPUR, Uttar Azamgarh 9026699883 govindazm@gmail. Azamgarh Union Bank of Shri R A Singh 9415835509 5462246390 TAMSA F.L.C.C. of Technology RAJAPURSIKRAUR, Pradesh com India Azamgarh, Collectorate, Private ITC - BEENAPARA, Azamgarh, 276001 Binapara - AZAMGARH Azamgarh GR09000314 Sant Kabir Private P Sant Kabir ITI, Salarpur, Uttar Varanasi 7376470615 [email protected] Varanasi Union Bank of Shri Nirmal 9415359661 5422370377 House No: 241G, ITC - Varanasi Rasulgarh,Varanasi Pradesh m India Kumar Ledhupur, Sarnath, Varanasi GR09000426 A.H. Private ITC - P A H ITI SIDHARI Uttar Azamgarh 9919554681 abdulhameeditc@g Azamgarh Union Bank of Shri R A Singh 9415835509 5462246390 TAMSA F.L.C.C. Azamgarh AZAMGARH Pradesh mail.com India Azamgarh, Collectorate, Azamgarh, 276001 GR09001146 Ramnath Munshi P SADAT GHAZIPUR Uttar Ghazipur 9415838111 rmiti2014@rediffm Ghazipur Union Bank of Shri B N R 9415889739 5482226630 UNION BANK OF INDIA Private Itc - Pradesh ail.com India Gupta FLC CENTER Ghazipur DADRIGHAT GHAZIPUR GR09001184 The IETE Private P 248, Uttar Varanasi 9454234449 ietevaranasi@rediff Varanasi Union Bank of Shri Nirmal 9415359661 5422370377 House No: 241G, ITI - Varanasi Maheshpur,Industrial Pradesh mail.com India Kumar Ledhupur, Sarnath, Area Post : Industrial Varanasi GR09001243 Dr. -

CIN Company Name Investor First Name Investor Middle Name
Note: This sheet is applicable for uploading the particulars related to the shares transferred to Investor Education and Protection Fund. Make sure that the details are in accordance with the information already provided in e-form IEPF-4. CIN L40101DL1989GOI038121 Prefill Company Name POWER GRID CORPORATION OF INDIA LIMITED Nominal value of shares 2984380.00 Validate Clear Actual Date of Investor First Investor Middle Investor Last Father/Husband Father/Husband Father/Husband Last DP Id-Client Id- Nominal value of Address Country State District Pin Code Folio Number Number of shares transfer to IEPF (DD- Name Name Name First Name Middle Name Name Account Number shares MON-YYYY) HARESH JAGJIVAN KHORASIA JAGJIVAN DEVCHAND KHORASIA 128/25, 2ND FLOOR, HAZRA ROAD, KOLKATA,INDIA KOLKATA. WESTWEST BENGAL. BENGAL KOLKATA 700026 C12010200-12010200-00021620 10 100.00 18-DEC-2017 AMBALAL PREMJIBHAI PATEL PREMJIBHAI GOVINDBHAI PATEL DEBHARI, TA - VIRPUR, DIST- KHEDA, INDIAVIRPUR GUJARAT GUJARAT VIRPUR 388260 C12010400-12010400-00008557 10 100.00 18-DEC-2017 HARI BABU CHADERIA KUDAN LAL CHANDERIA Ward No-8, Pt Dindayal Puram BalaghatIndia MADHYA PRADESHMADHYA PRADESH BALAGHAT 481001 C12010600-12010600-00114061 200 2000.00 18-DEC-2017 SUDHIR KUMAR JAIN SHRI ASHOK KUMAR JAIN HNO.:16/1249, BEHIND RAIPUR FLOURINDIA MILL FAFADIH RAIPURCHHATTISGARH CHHATTISGARH RAIPUR 492001 C12010600-12010600-00160701 100 1000.00 18-DEC-2017 RAJ DEO RAI LATE RAM BRIKSH RAI S/O LATE RAM BRICHH RAJ F NO 302 INDIAMAA ENCLAVE KOK-2 (BAT)JHARKHAND KOKAR RANCHI RANCHIRANCHI JHARKHAND -
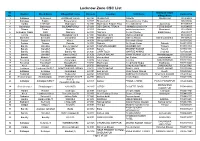
Lucknow Zone CSC List.Xlsx
Lucknow Zone CSC List Sl. Grampanchayat District Block Name Village/CSC name Pincode Location VLE Name Contact No No. Village Name 1 Sultanpur Sultanpur4 JAISINGHPUR(R) 228125 ISHAQPUR DINESH ISHAQPUR 730906408 2 Sultanpur Baldirai Bhawanighar 227815 Bhawanighar Sarvesh Kumar Yadav 896097886 3 Hardoi HARDOI1 Madhoganj 241301 Madhoganj Bilgram Road Devendra Singh Jujuvamau 912559307 4 Balrampur Balrampur BALRAMPUR(U) 271201 DEVI DAYAL TIRAHA HIMANSHU MISHRA TERHI BAZAR 912594555 5 Sitapur Sitapur Hargaon 261121 Hargaon ashok kumar singh Mumtazpur 919283496 6 Ambedkar Nagar Bhiti Naghara 224141 Naghara Gunjan Pandey Balal Paikauli 979214477 7 Gonda Nawabganj Nawabganj gird 271303 Nawabganj gird Mahmood ahmad 983850691 8 Shravasti Shravasti Jamunaha 271803 MaharooMurtiha Nafees Ahmad MaharooMurtiha 991941625 9 Badaun Budaun2 Kisrua 243601 Village KISRUA Shailendra Singh 5835005612 10 Badaun Gunnor Babrala 243751 Babrala Ajit Singh Yadav Babrala 5836237097 11 Bareilly Bareilly2 Bareilly Npp(U) 243201 TALPURA BAHERI JASVEER GIR Talpura 7037003700 12 Bareilly Bareilly3 Kyara(R) 243001 Kareilly BRIJESH KUMAR Kareilly 7037081113 13 Bareilly Bareilly5 Bareilly Nn 243003 CHIPI TOLA MAHFUZ AHMAD Chipi tola 7037260356 14 Bareilly Bareilly1 Bareilly Nn(U) 243006 DURGA NAGAR VINAY KUMAR GUPTA Nawada jogiyan 7037769541 15 Badaun Budaun1 shahavajpur 243638 shahavajpur Jay Kishan shahavajpur 7037970292 16 Faizabad Faizabad5 Askaranpur 224204 Askaranpur Kanchan ASKARANPUR 7052115061 17 Faizabad Faizabad2 Mosodha(R) 224201 Madhavpur Deepchand Gupta Madhavpur -

Self-Employment
SELF-EMPLOYMENT A Framework for Implementation National Rural Livelihood Mission Ministry of Rural Development Government of India SELF-EMPLOYMENT A Framework for Implementation National Rural Livelihood Mission Ministry of Rural Development Government of India June 22, 2016 Executive Summary MoRD has been thinking about a strategy to systematically bring panchayats out of poverty within a clear timeline. Given that 51% of the rural workforce is self-employed, there is a need to create a policy framework for holistically improving self-employment opportunities for the rural poor. In the light of the above, a framework document titled Self-Employment–A Framework for Implementation (No.J-11060/1/2016-RL) dated June 22nd, 2016 has been prepared after a consultation with state representatives in NIRD&PR in Hyderabad on January 9, 2016 and a national consultation in Delhi at Vigyan Bhawan on January 14, 2016. Before the document is taken up for formal consideration at the GoI level, it was thought necessary to seek the opinion of State governments. Accordingly, a copy of the framework document is hereby attached for your comments. The framework proposes a new scheme within the NRLM framework called the Grameen Swarozghar Yojana (GSY) that would be implemented through inter-departmental collaboration. The proposal is to ensure that self-employment, skill up-gradation, and efficient delivery of government schemes and entitlements lead to poverty-free panchayats within a definite timeline. The new scheme is proposed on 7 key principles: 1. Build on the strengths of previous efforts while avoiding it weaknesses 2. Build on the recent success of establishing high quality SHGs through the CRP strategy 3. -
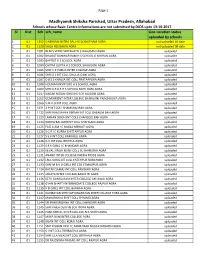
Center Information Not Updated by DIOS 13102017.Xlsx
Page 1 Madhyamik Shiksha Parishad, Uttar Pradesh, Allahabad Schools whose Basic Centre Informations are not submitted by DIOS upto 13-10-2017 Sl Dist Sch sch_name Geo-Location status uploaded by schools 1 01 1352 S NEKRAM NETRA PAL H S SCH KITHAM AGRA not uploaded till date 2 01 1620 SHILA HSS BAGIA AGRA not uploaded till date 3 01 1001 BENI S VEDIC VIDYAVATI I C BALUGANJ AGRA uploaded 4 01 1002 BHAGAT KANWAR RAM H S SCHOOL G M KHAN AGRA uploaded 5 01 1003 BAPTIST H S SCHOOL AGRA uploaded 6 01 1004 CHITRA GUPTA H S SCHOOL SHAHGANJ AGRA uploaded 7 01 1005 SHRI C P PUBLIC INTER COLLEGE AGRA uploaded 8 01 1006 SHRI D J INT COLL DHULIA GANJ AGRA uploaded 9 01 1007 D B S S KHALSA INT COLL PRATAPPURA AGRA uploaded 10 01 1008 HOLMAN INSTITUTE H S SCHOOL AGRA uploaded 11 01 1009 SHRI K R B R H S SCHOOL MOTI GANJ AGRA uploaded 12 01 1037 NAGAR NIGAM GIRLS HS SCH TAJGANJ AGRA uploaded 13 01 1052 GOVERMENT INTER COLLEGE SHAHGANJ PNACHKUIYA AGRA uploaded 14 01 1066 S M A O INT COLL AGRA uploaded 15 01 1071 A P INT COLL SHAMSHADBAD AGRA uploaded 16 01 1122 SHRI RAM SAHAY VERMA INT COLL BASAUNI BAH AGRA uploaded 17 01 1123 LAKHAN SINGH INT COLL CHANGOLI BAH AGRA uploaded 18 01 1124 RADHA BALLABH INT COLL SHAHGANJ AGRA uploaded 19 01 1125 FAIZ A AM I C NAGLA MEWATI AGRA uploaded 20 01 1126 S G R I C KURRA CHITTARPUR AGRA uploaded 21 01 1127 S S V INT COLL KARKAULI AGRA uploaded 22 01 1128 G V INT COLL BRITHLA AGRA uploaded 23 01 1129 S R K GIRLS I C KHANDARI AGRA uploaded 24 01 1130 KEVAL SINGH M INT COLL SUTHARI BAH AGRA uploaded 25 01 1131 ANAND INTER -

List of Common Service Centres Established in Uttar Pradesh
LIST OF COMMON SERVICE CENTRES ESTABLISHED IN UTTAR PRADESH S.No. VLE Name Contact Number Village Block District SCA 1 Aram singh 9458468112 Fathehabad Fathehabad Agra Vayam Tech. 2 Shiv Shankar Sharma 9528570704 Pentikhera Fathehabad Agra Vayam Tech. 3 Rajesh Singh 9058541589 Bhikanpur (Sarangpur) Fatehabad Agra Vayam Tech. 4 Ravindra Kumar Sharma 9758227711 Jarari (Rasoolpur) Fatehabad Agra Vayam Tech. 5 Satendra 9759965038 Bijoli Bah Agra Vayam Tech. 6 Mahesh Kumar 9412414296 Bara Khurd Akrabad Aligarh Vayam Tech. 7 Mohit Kumar Sharma 9410692572 Pali Mukimpur Bijoli Aligarh Vayam Tech. 8 Rakesh Kumur 9917177296 Pilkhunu Bijoli Aligarh Vayam Tech. 9 Vijay Pal Singh 9410256553 Quarsi Lodha Aligarh Vayam Tech. 10 Prasann Kumar 9759979754 Jirauli Dhoomsingh Atruli Aligarh Vayam Tech. 11 Rajkumar 9758978036 Kaliyanpur Rani Atruli Aligarh Vayam Tech. 12 Ravisankar 8006529997 Nagar Atruli Aligarh Vayam Tech. 13 Ajitendra Vijay 9917273495 Mahamudpur Jamalpur Dhanipur Aligarh Vayam Tech. 14 Divya Sharma 7830346821 Bankner Khair Aligarh Vayam Tech. 15 Ajay Pal Singh 9012148987 Kandli Iglas Aligarh Vayam Tech. 16 Puneet Agrawal 8410104219 Chota Jawan Jawan Aligarh Vayam Tech. 17 Upendra Singh 9568154697 Nagla Lochan Bijoli Aligarh Vayam Tech. 18 VIKAS 9719632620 CHAK VEERUMPUR JEWAR G.B.Nagar Vayam Tech. 19 MUSARRAT ALI 9015072930 JARCHA DADRI G.B.Nagar Vayam Tech. 20 SATYA BHAN SINGH 9818498799 KHATANA DADRI G.B.Nagar Vayam Tech. 21 SATYVIR SINGH 8979997811 NAGLA NAINSUKH DADRI G.B.Nagar Vayam Tech. 22 VIKRAM SINGH 9015758386 AKILPUR JAGER DADRI G.B.Nagar Vayam Tech. 23 Pushpendra Kumar 9412845804 Mohmadpur Jadon Dankaur G.B.Nagar Vayam Tech. 24 Sandeep Tyagi 9810206799 Chhaprola Bisrakh G.B.Nagar Vayam Tech.