Oral Mucosal Persistent and Short Term
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Lumps and Swellings
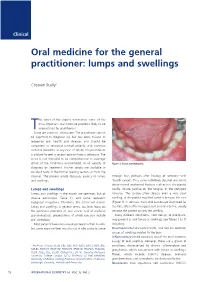
Clinical Oral medicine for the general practitioner: lumps and swellings Crispian Scully 1 his series of five papers summarises some of the most important oral medicine problems likely to be Tencountered by practitioners. Some are common, others rare. The practitioner cannot be expected to diagnose all, but has been trained to recognise oral health and disease, and should be competent to recognise normal variants, and common orofacial disorders. In any case of doubt, the practitioner is advised to seek a second opinion from a colleague. The series is not intended to be comprehensive in coverage either of the conditions encountered, or all aspects of Figure 1: Torus mandibularis. diagnosis or treatment: further details are available in standard texts, in the further reading section, or from the internet. The present article discusses aspects of lumps through fear, perhaps after hearing of someone with and swellings. ‘mouth cancer’. Thus some individuals discover and worry about normal anatomical features such as tori, the parotid Lumps and swellings papilla, foliate papillae on the tongue, or the pterygoid Lumps and swellings in the mouth are common, but of hamulus. The tongue often detects even a very small diverse aetiologies (Table 1), and some represent swelling, or the patient may first notice it because it is sore malignant neoplasms. Therefore, this article will discuss (Figure 1). In contrast, many oral cancers are diagnosed far lumps and swellings in general terms, but later focus on too late, often after being present several months, usually the particular problems of oral cancer and of orofacial because the patient ignores the swelling. -

Glossary for Narrative Writing
Periodontal Assessment and Treatment Planning Gingival description Color: o pink o erythematous o cyanotic o racial pigmentation o metallic pigmentation o uniformity Contour: o recession o clefts o enlarged papillae o cratered papillae o blunted papillae o highly rolled o bulbous o knife-edged o scalloped o stippled Consistency: o firm o edematous o hyperplastic o fibrotic Band of gingiva: o amount o quality o location o treatability Bleeding tendency: o sulcus base, lining o gingival margins Suppuration Sinus tract formation Pocket depths Pseudopockets Frena Pain Other pathology Dental Description Defective restorations: o overhangs o open contacts o poor contours Fractured cusps 1 ww.links2success.biz [email protected] 914-303-6464 Caries Deposits: o Type . plaque . calculus . stain . matera alba o Location . supragingival . subgingival o Severity . mild . moderate . severe Wear facets Percussion sensitivity Tooth vitality Attrition, erosion, abrasion Occlusal plane level Occlusion findings Furcations Mobility Fremitus Radiographic findings Film dates Crown:root ratio Amount of bone loss o horizontal; vertical o localized; generalized Root length and shape Overhangs Bulbous crowns Fenestrations Dehiscences Tooth resorption Retained root tips Impacted teeth Root proximities Tilted teeth Radiolucencies/opacities Etiologic factors Local: o plaque o calculus o overhangs 2 ww.links2success.biz [email protected] 914-303-6464 o orthodontic apparatus o open margins o open contacts o improper -

Clinical Practice Statements-Oral Contact Allergy
Clinical Practice Statements-Oral Contact Allergy Subject: Oral Contact Allergy The American Academy of Oral Medicine (AAOM) affirms that oral contact allergy (OCA) is an oral mucosal response that may be associated with materials and substances found in oral hygiene products, common food items, and topically applied agents. The AAOM also affirms that patients with suspected OCA should be referred to the appropriate dental and/or medical health care provider(s) for comprehensive evaluation and management of the condition. Replacement and/or substitution of dental materials should be considered only if (1) a reasonable temporal association has been established between the suspected triggering material and development of clinical signs and/or symptoms, (2) clinical examination supports an association between the suspected triggering material and objective clinical findings, and (3) diagnostic testing (e.g., dermatologic patch testing, skin-prick testing) confirms a hypersensitivity reaction to the suspected offending material. Originators: Dr. Eric T. Stoopler, DMD, FDS RCSEd, FDS RCSEng, Dr. Scott S. De Rossi, DMD. This Clinical Practice Statement was developed as an educational tool based on expert consensus of the American Academy of Oral Medicine (AAOM) leadership. Readers are encouraged to consider the recommendations in the context of their specific clinical situation, and consult, when appropriate, other sources of clinical, scientific, or regulatory information prior to making a treatment decision. Originator: Dr. Eric T. Stoopler, DMD, FDS RCSEd, FDS RCSEng, Dr. Scott S. De Rossi, DMD Review: AAOM Education Committee Approval: AAOM Executive Committee Adopted: October 17, 2015 Updated: February 5, 2016 Purpose The AAOM affirms that oral contact allergy (OCA) is an oral mucosal response that may be associated with materials and substances found in oral hygiene products, common food items, and topically applied agents. -

White Lesions of the Oral Cavity and Derive a Differential Diagnosis Four for Various White Lesions
2014 self-study course four course The Ohio State University College of Dentistry is a recognized provider for ADA, CERP, and AGD Fellowship, Mastership and Maintenance credit. ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry. Concerns or complaints about a CE provider may be directed to the provider or to ADA CERP at www.ada.org/goto/cerp. The Ohio State University College of Dentistry is approved by the Ohio State Dental Board as a permanent sponsor of continuing dental education ABOUT this FREQUENTLY asked COURSE… QUESTIONS… Q: Who can earn FREE CE credits? . READ the MATERIALS. Read and review the course materials. A: EVERYONE - All dental professionals in your office may earn free CE contact . COMPLETE the TEST. Answer the credits. Each person must read the eight question test. A total of 6/8 course materials and submit an questions must be answered correctly online answer form independently. for credit. us . SUBMIT the ANSWER FORM Q: What if I did not receive a ONLINE. You MUST submit your confirmation ID? answers ONLINE at: A: Once you have fully completed your p h o n e http://dent.osu.edu/sterilization/ce answer form and click “submit” you will be directed to a page with a . RECORD or PRINT THE 614-292-6737 unique confirmation ID. CONFIRMATION ID This unique ID is displayed upon successful submission Q: Where can I find my SMS number? of your answer form. -

Pediatric Oral Pathology. Soft Tissue and Periodontal Conditions
PEDIATRIC ORAL HEALTH 0031-3955100 $15.00 + .OO PEDIATRIC ORAL PATHOLOGY Soft Tissue and Periodontal Conditions Jayne E. Delaney, DDS, MSD, and Martha Ann Keels, DDS, PhD Parents often are concerned with “lumps and bumps” that appear in the mouths of children. Pediatricians should be able to distinguish the normal clinical appearance of the intraoral tissues in children from gingivitis, periodontal abnormalities, and oral lesions. Recognizing early primary tooth mobility or early primary tooth loss is critical because these dental findings may be indicative of a severe underlying medical illness. Diagnostic criteria and .treatment recommendations are reviewed for many commonly encountered oral conditions. INTRAORAL SOFT-TISSUE ABNORMALITIES Congenital Lesions Ankyloglossia Ankyloglossia, or “tongue-tied,” is a common congenital condition characterized by an abnormally short lingual frenum and the inability to extend the tongue. The frenum may lengthen with growth to produce normal function. If the extent of the ankyloglossia is severe, speech may be affected, mandating speech therapy or surgical correction. If a child is able to extend his or her tongue sufficiently far to moisten the lower lip, then a frenectomy usually is not indicated (Fig. 1). From Private Practice, Waldorf, Maryland (JED); and Department of Pediatrics, Division of Pediatric Dentistry, Duke Children’s Hospital, Duke University Medical Center, Durham, North Carolina (MAK) ~~ ~ ~ ~ ~ ~ ~ PEDIATRIC CLINICS OF NORTH AMERICA VOLUME 47 * NUMBER 5 OCTOBER 2000 1125 1126 DELANEY & KEELS Figure 1. A, Short lingual frenum in a 4-year-old child. B, Child demonstrating the ability to lick his lower lip. Developmental Lesions Geographic Tongue Benign migratory glossitis, or geographic tongue, is a common finding during routine clinical examination of children. -

Study of Oropharyngeal Ulcers with Their Commonest Anatomical Sites of Presentation Correlated with Histopathological Diagnosis Among the North Bengal Population
Panacea Journal of Medical Sciences 2020;10(3):258–263 Content available at: https://www.ipinnovative.com/open-access-journals Panacea Journal of Medical Sciences Journal homepage: www.ipinnovative.com Original Research Article Study of oropharyngeal ulcers with their commonest anatomical sites of presentation correlated with histopathological diagnosis among the north Bengal population Tanwi Ghosal (Sen)1, Pallab Kr Saha2,*, Sauris Sen3 1Dept. of Anatomy, North Bengal Medical College, Sushrutanagar, West Bengal, India 2Dept. of Anatomy, NRS Medical College, Kolkata, West Bengal, India 3Dept. of ENT, Jalpaiguri District Hospital, Jalpaiguri, West Bengal, India ARTICLEINFO ABSTRACT Article history: Introduction: Oropharyngeal ulcers are very common in North East part of India due to bad oral habits like Received 31-07-2020 chewing of tobacco etc. A study was performed at North Bengal Medical College and Hospital among the Accepted 06-10-2020 patients attending otorhinolaryngology outdoor to explore the relationship of different types and proportion Available online 29-12-2020 of oropharyngeal ulcers with their commonest anatomical sites and to elicit the relationship with bad oral habits. Aims: • To elicit the different types and proportions of oropharyngeal ulcers. • To explore the relationship Keywords: of different histopathological types with anatomical sites. • To identify the relationship with addiction. Ulcer Material and Methods: This is a Cross-sectional Observational Hospital based study, conducted in the Oral Cavity Otorhinolaryngology outdoor of North Bengal Medical College and Hospital twice a week. 102 patients Oropharynx were selected as study population after maintaining inclusion and exclusion criteria. Anatomical sites Results: The study shows that the most common type of ulcer is aphthous (25.49%) and the least common types are erythroplakia and autoimmune ulcers (1.96%). -

Orofacial Granulomatosis
Al-Hamad, A; Porter, S; Fedele, S; (2015) Orofacial Granulomatosis. Dermatol Clin , 33 (3) pp. 433- 446. 10.1016/j.det.2015.03.008. Downloaded from UCL Discovery: http://discovery.ucl.ac.uk/1470143 ARTICLE Oro-facial Granulomatosis Arwa Al-Hamad1, 2, Stephen Porter1, Stefano Fedele1, 3 1 University College London, UCL Eastman Dental Institute, Oral Medicine Unit, 256 Gray’s Inn Road, WC1X 8LD, London UK. 2 Dental Services, King Abdulaziz Medical City-Riyadh, Ministry of National Guard, Riyadh, Saudi Arabia. 3 NIHR University College London Hospitals Biomedical Research Centre, London, UK. Acknowledgments: Part of this work was undertaken at University College London/University College London Hospital, which received a proportion of funding from the Department of Health’s National Institute for Health Research Biomedical Research Centre funding scheme. Conflicts of Interest: The authors declare that they have no affiliation with any organization with a financial interest, direct or indirect, in the subject matter or materials discussed in the manuscript that may affect the conduct or reporting of the work submitted. Authorship: all authors named above meet the following criteria of the International Committee of Medical Journal Editors: 1) Substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data; 2) Drafting the article or revising it critically for important intellectual content; 3) Final approval of the version to be published. Corresponding author: Dr. Stefano Fedele DDS, PhD -

Features of Reactive White Lesions of the Oral Mucosa
Head and Neck Pathology (2019) 13:16–24 https://doi.org/10.1007/s12105-018-0986-3 SPECIAL ISSUE: COLORS AND TEXTURES, A REVIEW OF ORAL MUCOSAL ENTITIES Frictional Keratosis, Contact Keratosis and Smokeless Tobacco Keratosis: Features of Reactive White Lesions of the Oral Mucosa Susan Müller1 Received: 21 September 2018 / Accepted: 2 November 2018 / Published online: 22 January 2019 © Springer Science+Business Media, LLC, part of Springer Nature 2019 Abstract White lesions of the oral cavity are quite common and can have a variety of etiologies, both benign and malignant. Although the vast majority of publications focus on leukoplakia and other potentially malignant lesions, most oral lesions that appear white are benign. This review will focus exclusively on reactive white oral lesions. Included in the discussion are frictional keratoses, irritant contact stomatitis, and smokeless tobacco keratoses. Leukoedema and hereditary genodermatoses that may enter in the clinical differential diagnoses of frictional keratoses including white sponge nevus and hereditary benign intraepithelial dyskeratosis will be reviewed. Many products can result in contact stomatitis. Dentrifice-related stomatitis, contact reactions to amalgam and cinnamon can cause keratotic lesions. Each of these lesions have microscopic findings that can assist in patient management. Keywords Leukoplakia · Frictional keratosis · Smokeless tobacco keratosis · Stomatitis · Leukoedema · Cinnamon Introduction white lesions including infective and non-infective causes will be discussed -

Orofacial Granulomatosis Presenting As Gingival Enlargement – Report of Three Cases
Open Access Journal of Dentistry & Oral Disorders Case Report Orofacial Granulomatosis Presenting as Gingival Enlargement – Report of Three Cases Savithri V*, Janardhanan M, Suresh R and Aravind T Abstract Department of Oral Pathology & Microbiology, Amrita Orofacial Granulomatosis (OFG) is an uncommon disease characterized School of Dentistry, Amrita VishwaVidyapeetham, Amrita by non-caseating granulomatous inflammation in the oral and maxillofacial University, India region. They present clinically as labial enlargement, perioral and/or mucosal *Corresponding author: Vindhya Savithri, swelling, angular cheilitis, mucosal tags, vertical fissures of lips, lingua plicata, Department of Oral Pathology & Microbiology, Amrita oral ulcerations and gingival enlargement. The term OFG was introduced by School of Dentistry, Amrita VishwaVidyapeetham, Amrita Wiesenfeld in 1985. The diagnosis of OFG is done by the clinical presentation University, India and histological picture and this may be further complicated by the fact that OFG may be the oral manifestation of a systemic condition, such as Crohn’s Received: October 16, 2017; Accepted: November 27, disease, sarcoidosis, or, more rarely, Wegener’s granulomatosis. In addition, 2017; Published: December 04, 2017 several conditions, including tuberculosis, leprosy, systemic fungal infections, and foreign body reactions may show granulomatous inflammation on histologic examination. They have to be excluded out by appropriate investigations. They have to be excluded out by appropriate investigations. -

Herpes Simplex Virus Infection
FUNGI VIRUS BACTERIA DISEASE The oral focal infection theory • A concept generally negleted for several decades, is controversial yet has gained renewed interest with progress in clasification and identification of oral microorganisms. • Additionally, recent evidence associating dental with artherosclerosis and other chronic disease has also helped resurrect the focal infection theory Pathways of infection arising from oral bacteria The three pathway that may link oral bacteria to secondary disease distant from the oral nidus are : 1. Metastatic infection attributable to transient bacteria in the blood 2. Metastatic immunologic injury 3. Metastatic toxic injury The scientific evidence weak a it is best supports of first pathway of transient bacteriemias of oral origin Mechanical prosthetic valve (arrow) Odontogenic infection Caries dental pulpitis Necrosis of the pulp pulp polyp Periapical abscess Periodontal infection Periodontal abscess Gingivitis ANUG Salivary infection Mucositis Recurent Apthous Stomatitis Minor RAS Mayor Fungal infection • Are oral fungal infections common ? • No, most are associated with an underlying systemic condition immunosuppression imunodeficiency syndrome cancer therapy anemia diabetes uremia leukemia • Patients who have conditions that modify the normal oral environment are at increased risk of fungal infection Among these individuals are patients with _ xerostomia _ have taken broad spectrum antibiotics Diagnosis of oral fungal infection based on : • History • Clinical appearance • Culture • Potassium hydroxide -

Pdf (563.04 K)
EGYPTIAN Vol. 65, 927:939, April, 2019 DENTAL JOURNAL I.S.S.N 0070-9484 Orthodontics, Pediatric and Preventive Dentistry www.eda-egypt.org • Codex : 180/1904 THE MOST COMMON 5 PEDIATRIC ORAL LESIONS IN MIDDLE NILE DELTA, EGYPT Talat M. Beltagy*, Enas A. El-Gendy**, Emad F. Essa*** and Ibrahim A. Kabbash**** ABSTRACT Background: The prevalence studies on common pediatric oral lesions (POLs) are still rare compared with those on dental caries and periodontal diseases. POLs vary among different geographic regions, age, racial and lifestyle of each population. The purpose of this study was to determine the most common 5 POLs referred to 5 different dental and medical branches in Middle Nile Delta, Egypt. Materials and methods: A qualitative study design was used depending on expert opinions on oral lesions in children (aged 0-14 years). A total of 1164 dental and medical staff members, dentists and physicians at the hospitals of Universities and Ministry of Health, and Specialized Medical Centers & hospitals in the Middle Nile Delta region were included. The target population of the study was experts in 5 branches: Pedodontics, Oral Medicine and Periodontology, Oral and Maxillofacial Surgery, Pediatrics, and Dermatology and Venereology. Data were collected using a checklist including the common diseases within the scope of the study and each expert was asked to give percentages for children seen with each disease entity in his/her branch. Data analysis: Data were statistically analyzed using Statistical Package for the Social Sciences version 19. For each disease, the number and percentage were calculated and differences between observation recorded by health care workers in University and Ministry of Health were tested by chi-square test. -

Topographical Dermatology Picture Cause Basic Lesion
page: 332 Chapter 12: alphabetical Topographical dermatology picture cause basic lesion search contents print last screen viewed back next Topographical dermatology Alopecia page: 333 12.1 Alopecia alphabetical Alopecia areata Alopecia areata of the scalp is characterized by the appearance of round or oval, smooth, shiny picture patches of alopecia which gradually increase in size. The patches are usually homogeneously glabrous and are bordered by a peripheral scatter of short broken- cause off hairs known as exclamation- mark hairs. basic lesion Basic Lesions: None specific Causes: None specific search contents print last screen viewed back next Topographical dermatology Alopecia page: 334 alphabetical Alopecia areata continued Alopecia areata of the occipital region, known as ophiasis, is more resistant to regrowth. Other hair picture regions can also be affected: eyebrows, eyelashes, beard, and the axillary and pubic regions. In some cases the alopecia can be generalized: this is known as cause alopecia totalis (scalp) and alopecia universalis (whole body). basic lesion Basic Lesions: Causes: None specific search contents print last screen viewed back next Topographical dermatology Alopecia page: 335 alphabetical Pseudopelade Pseudopelade consists of circumscribed alopecia which varies in shape and in size, with picture more or less distinct limits. The skin is atrophic and adheres to the underlying tissue layers. This unusual cicatricial clinical appearance can be symptomatic of cause various other conditions: lupus erythematosus, lichen planus, folliculitis decalvans. Some cases are idiopathic and these are known as pseudopelade. basic lesion Basic Lesions: Atrophy; Scars Causes: None specific search contents print last screen viewed back next Topographical dermatology Alopecia page: 336 alphabetical Trichotillomania Plucking of the hair on a large scale.