NAMS 53 2 SINGLE PAGE.Cdr
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Annual Report 2016-17
Jeee|<ekeâ efjheesš& Annual Report 201201666---20120120177 केb6ीय ितबती अaययन िव िवcालय Central University of Tibetan Studies (Deemed University) Sarnath, Varanasi - 221007 www.cuts.ac.in Conference on Buddhist Pramana A Glance of Cultural Programme Contents Chapters Page Nos. 1. A Brief Profile of the University 3 2. Faculties and Academic Departments 9 3. Research Departments 45 4. Shantarakshita Library 64 5. Administration 79 6. Activities 89 Appendices 1. List of Convocations held and Honoris Causa Degrees Conferred on Eminent Persons by CUTS 103 2. List of Members of the CUTS Society 105 3. List of Members of the Board of Governors 107 4. List of Members of the Academic Council 109 5. List of Members of the Finance Committee 112 6. List of Members of the Planning and Monitoring Board 113 7. List of Members of the Publication Committee 114 Editorial Committee Chairman: Dr. Dharma Dutt Chaturvedi Associate Professor, Dean, Faculty of Shabdavidya, Department of Sanskrit, Department of Classical and Modern Languages Members: Shri R. K. Mishra Documentation Officer Shantarakshita Library Shri Tenzin Kunsel P. R. O. V.C. Office Member Secretary: Shri M.L. Singh Sr. Clerk (Admn. Section-I) [2] A BRIEF PROFILE OF THE UNIVERSITY 1. A BRIEF PROFILE OF THE UNIVERSITY The Central University of Tibetan Studies (CUTS) at Sarnath is one of its kind in the country. The University was established in 1967. The idea of the University was mooted in course of a dialogue between Pandit Jawaharlal Nehru, the first Prime Minister of India and His Holiness the Dalai Lama with a view to educating the young Tibetan in exile and those from the Himalayan regions of India, who have religion, culture and language in common with Tibet. -

Acrs Je 2014
LIST OF ACRS OF JUNIOR ENGINERS (CIVIL) UP to 31.03.2014 S.No Name Designation D.O.B D.O.A Period 1 Pana Lal J.E 22.11.66 11.05.87 11.05.87 to31.03.2009 2 Paran Chand J.E 03.03.57 20.07.78 20.07.78 to 2008 3 Duni Chand J.E 04.01.56 24.07.78 24.07.78 & 01.08.03 to 31.03.10 4 Monaj kumar J.E 08.05.69 18.03.96 01.04.97 to 31.05.99 &01.04.04 to 31.03.112 5 Rajneesh Bansal J.E 04.10.67 23.01.95 23.01.95 to 31.03.2008 6 Paresh Chaun\han J.E 16.06.67 28.02.2004 01.03.2004 to 31.03.2012 7 Anil pathik J.E 03.05.65 28.02.04 01.04.2004 to 31.03.2012 8 Rajender Singh J.E 11.02.68 17.11.97 01.04.98 to 31.03.2009 Bagga 9 Rattan Chand J.E 22.08.60 01.04.85 01.04.85 to 31.03.98 10 Navneet Gupta J.E 03.04.72 12.08.97 12.08.97 to 31.03.2002 & 1.04.2006 yo 31.03.13 11 Mohan Rajeev J.E 23.07.63 24.01.85 01.04.85 to31.03.2004 12 Ravinder Kumar J.E 05.05.62 29.09.86 29.09.86 to 31.03.2013 13 Rajesh Kumar J.E 23.10.58 02.02.77 01.04.91 to31.03.210 14 Anil Kumar J.E 20.12.62 06.03.86 06.03.86 to31.03.2001 &01.04.2006 to31.03.2010 15 Skinder Singh J.E 03.03.68 19.07.93 19.07.93 to31.03.2010 16 Partap Singh J.E 02.01.60 08.12.86 01.04.2009 to 31.03.2012 17 18 Kishor Kumar J.E 04.07.67 10.01.97 01.04.99 to31.03.2012 19 Jagdish Chand J.E 28.01.62 16.02.96 01.04.08 to3 1.03.12 20 Anil Kumar J.E 06.06.66 14.06.91 01.04.08 to 31.03.12 21 Ashok Kumar J.E 18.04.69 13.11.2009 01.04.2010 to 31.03.2012 22 Pardeep Kumar J.E 06.03.62 01.01.97 01.01.97 to 31.03.12 Sharma 23 Pardeep kumar J.E 13.01.69 30.12.2005 01.04.2007 to 31.03.12 24 Ravinder Pal J.E 28.01.65 02.01.87 01.07.90 -
MGT-7 Submission
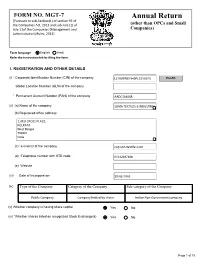
FORM NO. MGT-7 Annual Return [Pursuant to sub-Section(1) of section 92 of the Companies Act, 2013 and sub-rule (1) of (other than OPCs and Small rule 11of the Companies (Management and Companies) Administration) Rules, 2014] Form language English Hindi Refer the instruction kit for filing the form. I. REGISTRATION AND OTHER DETAILS (i) * Corporate Identification Number (CIN) of the company L51909WB1940PLC010070 Pre-fill Global Location Number (GLN) of the company * Permanent Account Number (PAN) of the company AADCS0405R (ii) (a) Name of the company SOMA TEXTILES & INDUSTRIES (b) Registered office address 2, RED CROSS PLACE, KOLKATA West Bengal 700001 India (c) *e-mail ID of the company [email protected] (d) *Telephone number with STD code 03322487406 (e) Website (iii) Date of Incorporation 29/03/1940 (iv) Type of the Company Category of the Company Sub-category of the Company Public Company Company limited by shares Indian Non-Government company (v) Whether company is having share capital Yes No (vi) *Whether shares listed on recognized Stock Exchange(s) Yes No Page 1 of 15 (a) Details of stock exchanges where shares are listed S. No. Stock Exchange Name Code 1 BSE LIMITED 1 2 National Stock Exchange of India 1,024 (b) CIN of the Registrar and Transfer Agent U67190MH1999PTC118368 Pre-fill Name of the Registrar and Transfer Agent LINK INTIME INDIA PRIVATE LIMITED Registered office address of the Registrar and Transfer Agents C-101, 1st Floor, 247 Park, Lal Bahadur Shastri Marg, Vikhroli (West) (vii) *Financial year From date 01/04/2020 (DD/MM/YYYY) To date 31/03/2021 (DD/MM/YYYY) (viii) *Whether Annual general meeting (AGM) held Yes No (a) If yes, date of AGM (b) Due date of AGM 30/09/2021 (c) Whether any extension for AGM granted Yes No II. -

53Rd AIIMS ANNUAL REPORT 2008–2009
53rd AIIMS ANNUAL REPORT 2008–2009 All India Institute of Medical Sciences New Delhi 110029 Edited jointly by: Dr Sunil Chumber, Additional Professor, Department of Surgical Disciplines and Sub-Dean (Academic) Dr Tanuj Dada, Associate Professor, Dr R.P. Centre for Ophthalmic Sciences Dr Venkata Karthikeyan C, Assistant Professor, Department of Otorhinolaryngology (ENT) Dr S.K. Maulik, Professor, Department of Pharmacology Dr Raj D. Mehra, Professor, Department of Anatomy Dr Kameshwar Prasad, Professor, Department of Neurology Dr S. Rastogi, Professor, Department of Orthopaedics Dr Sushma Sagar, Assistant Professor, JPNA Trauma Centre Dr Peush Sahni, Professor, Department of Gastrointestinal Surgery Dr Pratap Sharan, Professor, Department of Psychiatry Dr D.N. Sharma, Assistant Professor, Dr BRA, Institute Rotary Cancer Hospital Dr Subrata Sinha, Professor and Head, Department of Biochemistry Dr Sanjay Kumar Sood, Assistant Professor, Department of Physiology Dr Sachin Talwar, Assistant Professor, Department of C.T.V.S. February 2010 Printed at Saurabh Printers Pvt. Ltd., A-16, Sector-IV, NOIDA (U.P.) All India Institute of Medical Sciences The All India Institute of Medical Sciences (AIIMS) was established in 1956 as an institution of national importance by an Act of Parliament with the objects to develop patterns of teaching in undergraduate and postgraduate medical education in all its branches so as to demonstrate a high standard of medical education to all medical colleges and other allied institutions in India; to bring together in one place educational facilities of the highest order for the training of personnel in all important branches of health activity and to attain self-sufficiency in postgraduate medical education. -

Current Affairs 2013- January International
Current Affairs 2013- January International The Fourth Meeting of ASEAN and India Tourism Minister was held in Vientiane, Lao PDR on 21 January, in conjunction with the ASEAN Tourism Forum 2013. The Meeting was jointly co-chaired by Union Tourism Minister K.Chiranjeevi and Prof. Dr. Bosengkham Vongdara, Minister of Information, Culture and Tourism, Lao PDR. Both the Ministers signed the Protocol to amend the Memorandum of Understanding between ASEAN and India on Strengthening Tourism Cooperation, which would further strengthen the tourism collaboration between ASEAN and Indian national tourism organisations. The main objective of this Protocol is to amend the MoU to protect and safeguard the rights and interests of the parties with respect to national security, national and public interest or public order, protection of intellectual property rights, confidentiality and secrecy of documents, information and data. Both the Ministers welcomed the adoption of the Vision Statement of the ASEAN-India Commemorative Summit held on 20 December 2012 in New Delhi, India, particularly on enhancing the ASEAN Connectivity through supporting the implementation of the Master Plan on ASEAN Connectivity. The Ministers also supported the close collaboration of ASEAN and India to enhance air, sea and land connectivity within ASEAN and between ASEAN and India through ASEAN-India connectivity project. In further promoting tourism exchange between ASEAN and India, the Ministers agreed to launch the ASEAN-India tourism website (www.indiaasean.org) as a platform to jointly promote tourism destinations, sharing basic information about ASEAN Member States and India and a visitor guide. The Russian Navy on 20 January, has begun its biggest war games in the high seas in decades that will include manoeuvres off the shores of Syria. -

General Studies Series
IAS General Studies Series Current Affairs (Prelims), 2013 by Abhimanu’s IAS Study Group Chandigarh © 2013 Abhimanu Visions (E) Pvt Ltd. All rights reserved. No part of this document may be reproduced or transmitted in any form or by any means, electronic, mechanical, photocopying, recording, or any information storage or retrieval system or otherwise, without prior written permission of the owner/ publishers or in accordance with the provisions of the Copyright Act, 1957. Any person who does any unauthorized act in relation to this publication may be liable to criminal prosecution and civil claim for the damages. 2013 EDITION Disclaimer: Information contained in this work has been obtained by Abhimanu Visions from sources believed to be reliable. However neither Abhimanu's nor their author guarantees the accuracy and completeness of any information published herein. Though every effort has been made to avoid any error or omissions in this booklet, in spite of this error may creep in. Any mistake, error or discrepancy noted may be brought in the notice of the publisher, which shall be taken care in the next edition but neither Abhimanu's nor its authors are responsible for it. The owner/publisher reserves the rights to withdraw or amend this publication at any point of time without any notice. TABLE OF CONTENTS PERSONS IN NEWS .............................................................................................................................. 13 NATIONAL AFFAIRS .......................................................................................................................... -
Sl.No Membership Id Name State
Sl.No Membership Id Name State 1 10 BHAT K L DELHI 2 13 ADINARAYANA RAO S V ANDHRA PRADESH 3 20 AGARWAL S K WEST BENGAL 4 22 AGARWAL Y M HARYANA 5 26 AGARWAL P K JHARKHAND 6 32 AHMAD ABDUL HAI BIHAR 7 33 AHUJA A M LT GENERAL DELHI 8 35 SINGHVI A M RAJASTHAN 9 39 ALMAST S C DELHI 10 46 AMARESH BHASKAR NALLAVANDU AIR MSHL KARNATAKA 11 47 AMARESWAR T KARNATAKA 12 48 AMARJIT SINGH PUNJAB 13 49 AMBIKE V S MAHARASTRA 14 55 ANAND PRAKASH UTTAR PRADESH 15 58 ANANTHAKRISHNAN L TAMIL NADU 16 59 NARAYAN PRASAD K TAMILNADU 17 60 ANANTHANARAYANA RAO N KARNATAKA 18 72 ANTIA N H MAHARASTRA 19 76 APTE B P MAHARASTRA 20 79 ARCANJO DE MENESES GOA 21 83 ARORA S MAHARASTRA 22 91 ASOPA H S UTTAR PRADESH 23 95 VIKRAM PRATAP SINGH LT. COL. DELHI 24 101 BAJAJ P S BIHAR 25 108 BAPAT V C MADHYA PRADESH 26 109 BHATTACHARYYA S MAHARASTRA 27 118 KRISHNA HANDE H TAMIL NADU 28 123 BALLAL C R KARNATAKA 29 127 BAMRAH N S BRIG CHANDIGARH 30 130 BANERJEE L K DELHI 31 131 BANERJEE S WEST BENGAL 32 134 ASHIM BANERJEE(COL) WEST BENGAL 33 138 BAPAT S D MAHARASHTRA 34 140 DEEPAK V BHATT GUJARAT 35 147 PRANAB KUMAR BASU UTTAR PRADESH 36 149 BAWA H S PUNJAB 37 153 BEHERA D K ODISHA 38 159 BHAJEKAR A B MAHARASTRA 39 161 BAKTHAVATSALAM G TAMIL NADU 40 163 BHALERAO R A MAHARASHTRA 41 170 BHANUSHALI H S MAHARASTRA 42 176 BHARUCHA P B MAHARASTRA 43 179 BHASALE S P MAHARASHTRA 44 184 BHATT M V MAHARASHTRA 45 188 BHATHENA T R MAHARASHTRA 46 189 JAGDISHWER BHATT RAJASTHAN 47 195 SINGARAJU KRISHNA PRABHAKAR TELANGANA 48 199 RAVIKANTH C BANGALORE KARNATAKA 49 200 BHAKTA V P MAHARASTRA 50 -

January 2013
January1 of 91. 2013 International affairs: US President Barack Obama on 31 January, has come out with his much-awaited comprehensive immigration reforms, that will pave the way for legalization of more than 11 million undocumented immigrants. The reforms, which also propose to eliminate the annual country caps in the employment category, are expected to benefit large number of Indian technocrats and professionals. In a major policy speech on comprehensive immigration in Las Vegas, Obama urged the Congress to act on his proposals. The other key proposals of his "comprehensive" reform plan include "stapling" a green card to the diplomas of science, technology, engineering and mathematics (STEM), PhD and Masters Degree graduates from qualified US universities who have found employment in the country. The President also proposed to create a startup visa for job-creating entrepreneurs. The proposal allows foreign entrepreneurs, who attract financing or revenue from American investors and customers, to start and grow their businesses in the US, and to remain permanently if their companies grow further, create jobs for American workers, and strengthen the economy. The proposal removes the backlog for employment-sponsored immigration by eliminating annual country caps and adding additional visas to the system. Outdated legal immigration programs are reformed to meet current and future demands by exempting certain categories from annual visa limitations, the White House said. Obama also proposed to eliminate existing backlogs in the family-sponsored immigration system by recapturing unused visas and temporarily increasing annual visa numbers. The proposal also raises existing annual country caps from seven per cent to 15 per cent for the family-sponsored immigration system. -

Activity Report 2009 – 2010
Activity Report 2009 – 2010 L V Prasad Eye Institute Kallam Anji Reddy Campus L V Prasad Marg, Banjara Hills Hyderabad 500 034, India Tel: 91 40 3061 2345 Fax: 91 40 2354 8271 e-mail: [email protected] L V Prasad Eye Institute Patia, Bhubaneswar 751 024 Orissa, India Tel: 91 0674 3989 2020 Fax: 91 0674 3987 130 e-mail: [email protected] L V Prasad Eye Institute G M R Varalakshmi Campus Door No: 11-113/1 Hanumanthawaka Junction Visakhapatnam 530 040 Andhra Pradesh, India Tel: 91 0891 3989 2020 Fax: 91 0891 398 4444 L V Prasad Eye Institute e-mail: [email protected] Excellence • Equity • Effi ciency Art with vision, for vision Artist-in-residence Sisir Sahana in his workshop on A view of the Art Gallery on Level 6 at Hyderabad LVPEI’s Kallam Anji Reddy campus, Hyderabad creating campus, where several works by Mr Surya Prakash, one of his signature glass sculptures. Inset: A piece from our senior artist-in-residence are on display. his latest collection, entitled “The long climb”. Inset: The hand that wields the paintbrush! L V Prasad Eye Institute Committed to excellence and equity in eye care Activity Report April 2009 – March 2010 Collaborating Centre for Prevention of Blindness L V Prasad Eye Institute, a not-for-profi t charitable organization, is governed by two trusts: Hyderabad Eye Institute and Hyderabad Eye Research Foundation. Donations to Hyderabad Eye Research Foundation are 175% exempt under section 35 (i) (ii) and donations made to Hyderabad Eye Institute are 50% exempt under section 80G of the Income Tax Act. -

List of Fellows (Name-Wise) Upto 2016
LIST OF FELLOWS (NAME-WISE) UPTO 2016 0. Description Year 1. Abdul Kalam, A.P.J. Biomedical Engineering July 1995 DMIT. Former President, Republic of India. Res: 10 Rajaji Marg, New Delhi-110001. Permanent Address: No. 2, Mosque Street, Rameswaram, Ramanathapuram District, Tamil Nadu-623526. Tel: Off: (011) 3015321, 3014930, Res: (04567) 6493708, Fax: 2300756, E-mail: [email protected] (b 1931) (d.2015) Gen. Amir Chand Oration (NAMS, 1997-98) Padma Bhushan (1981); Padma Vibhushan (1990); Bharat Ratna (1997); D.Sc (h.c.) from several Universities; National Design Award; Dr. Biren Roy Space Award; Om Prakash Bhasin Award; National Nehru Award by Govt. of Madhya Pradesh; GM Modi Award for Science 1996; HK Firodia Award for Excellence in S&T 1996; Veer Savarkar Award 1998; Hon Fellow-Institution of Electronics and Telecommunication Engineers. 2. Abraham, Jacob Neurosurgery 1984 MS, MS (Neuro), FACS, FACA. Res: 10, 15th Avenue, Harrington Road, Chennai- 600031. Tel: Res: (044) 28363211, 42849258, Mobile: 09940118382, E-mail: [email protected] (b.1931). Basanti Devi Amir Chand Prize (ICMR, 1984); Sachs Memorial Lecturer, USA (1989). 3. Achari, Kamala Obstetrics and Gynecology 1982 MS, FRCOG, FICS, FACS. Emeritus Professor, Patna Medical College, Patna-800001 (Bihar). Res: 'Tirumalai', 21/D Road No.10, Rajendra Nagar, Patna- 800016. (b.1924) (d. 2014). 4. Adithan, C. Pharmacology July 2003 MD, PhD, FIMSA, FIPS. Former Professor & Head, Department of Pharmacology, Jawaharlal Institute of Postgraduate Medical Education & Research, Pondicherry- 605006. Currently: Director-CIDRF and Professor of Pharmacology, Mahatma Gandhi Medical College and Research Institute, Pondicherry-607403. Res: Flat No. 1, Srinivas Towers, Vazhudavour Road, Kathirkamam, Pondicherry-605009. -

Download Arogya Setu App for Those Living in Hotspot Areas of the State
Monthly Current AffairsTitle Capsule & Quiz MayTitle 2020 The countries placed on the list by the Trump administration on intellectual property (IP) related issues are Algeria, Argentina, Chile, China, India, Indonesia, Russia, Saudi Arabia, Ukraine and Venezuela. According to the World Intellectual Property International Labour Day: 1 May Right Organization, the Intellectual Property is the creation of literary and artistic works, symbols, names, images. World Tuna Day: 02 May Labour Day or International Workers' Day is observed each year on the first day of May to celebrate achievements of the working class. The day, also called 'May Day', is also observed as a public holiday in many countries. On 1 May, 1886, labour unions in the US decided to go on a strike demanding that World Tuna Day is observed on May 2 every year. workers should not be made to work for more than 8 hours a day. The United Nations (UN) established the Just three days after the strike began, a blast World Tuna Day to raise awareness about the occurred in Chicago's Haymarket Square tuna fish and its importance to humans and leaving many dead. earth. To honor those who died in the blast, the It is also observed to promote more International Socialist Conference declared 1 sustainable fishing practices. May as a day designated for labourers. The United Nations general assembly officially voted in favour of observing World US places India on priority watch list for Tuna Day in the year 2016. intellectual property protection World Tuna Day was observed for the first time in the year 2017. -

Annals of the National Academy of Medical Sciences (India)
Annals of the National Academy of Medical Sciences (India) EN JUB D IL L E O E Volume 50, No. 1&2 G January-June, 2014 ISSN 0379 - 038X Annals of the National Academy of Medical Sciences (India) -: A quarterly Journal :- Editor Dr. Sanjay Wadhwa Associate Editor Dr. K.K. Sharma Assistant Editor Dr. Jyoti Wadhwa Editorial Board Editorial Associates Dr. Snehalata Deshmukh Dr. Gourdas Choudhuri Dr. Mira Rajani Dr. Rani Kumar Dr. J.N. Pande Dr. Vinod Paul Dr. Prema Ramachandran Dr. Ashok Kumar Sharma Dr. H.S. Sandhu Dr. M.V. Padma Srivastava Dr. Lalita S. Kothari Dr. Deep Takkar Members of the Advisory Board Dr. Mahtab S. Bamji Dr. D.K. Hazra Dr. Raj Baveja Dr. H.S. Juneja Dr. M. Berry Dr. B.N. Koley Dr. C.S. Bhaskaran Dr. Anand Kumar Air Marshal (Retd.)Dr. M.S. Boparai Dr. R. Madan Dr. Sanjeev Misra Dr. Lalit Nath Dr. Y.K. Chawla Dr. Haribhai L. Patel Dr. P.K. Dave Dr. K.K. Talwar Dr. Saroj Chooramani Gopal Dr. S.P. Thyagarajan Dr. Amod Gupta Emeritus Editor: Prof. J.S. Bajaj Annual Subscription Rates Inland Rs. 500.00 Foreign $ 30.00 £ 15.00 Single Copy Rs. 150.00 Correspondence All correspondence concerning the Jornal should be addressed to: Editor National Academy of Medical Sciences (India) NAMS House, Ansari Nagar, Mahatma Gandhi Marg, New Delhi - 110029 Tel.: 011-26589289 E-mail: [email protected] Website: www.nams-india.in Ann Natl Acad Med Sci (India), 50(1&2):1-74, 2014 ANAMS 50 (1&2) : 1-74, 2014 CONTENTS Editorial i J.S.