5-Stridor, Stertor, and Babies That Squeak Evaluation Of
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Respiratory Examination Cardiac Examination Is an Essential Part of the Respiratory Assessment and Vice Versa
Respiratory examination Cardiac examination is an essential part of the respiratory assessment and vice versa. # Subject steps Pictures Notes Preparation: Pre-exam Checklist: A Very important. WIPE Be the one. 1 Wash your hands. Wash your hands in Introduce yourself to the patient, confirm front of the examiner or bring a sanitizer with 2 patient’s ID, explain the examination & you. take consent. Positioning of the patient and his/her (Position the patient in a 3 1 2 Privacy. 90 degree sitting position) and uncover Exposure. full exposure of the trunk. his/her upper body. 4 (if you could not, tell the examiner from the beginning). 3 4 Examination: General appearance: B (ABC2DEVs) Appearance: young, middle aged, or old, Begin by observing the and looks generally ill or well. patient's general health from the end of the bed. Observe the patient's general appearance (age, Around the bed I can't state of health, nutritional status and any other see any medications, obvious signs e.g. jaundice, cyanosis, O2 mask, or chest dyspnea). 1 tube(look at the lateral sides of chest wall), metered dose inhalers, and the presence of a sputum mug. 2 Body built: normal, thin, or obese The patient looks comfortable and he doesn't appear short of breath and he doesn't obviously use accessory muscles or any heard Connections: such as nasal cannula wheezes. To determine this, check for: (mention the medications), nasogastric Dyspnea: Assess the rate, depth, and regularity of the patient's 3 tube, oxygen mask, canals or nebulizer, breathing by counting the respiratory rate, range (16–25 breaths Holter monitor, I.V. -

Visual Examination
Visual Examination • Consider the impact of chest shape on the respiratory condition of the patient – Barrel chest – Kyphosis – Scoliosis – Pectus excavatum (funnel chest) – Pectus carinatum Visual Assessment of Thorax • Thoracic scars from previous surgery • Chest symmetry • Use of accessory muscles • Bruising • In drawing of ribs • Flail segment www.nejm.org/doi/full/10.1056/NEJMicm0904437 • Paradoxical breathing /seesaw breathing • Pursed lip breathing • Nasal flaring Palpation • For vibration of secretion • Surgical emphysema • Symmetry of chest movement • Tactile vocal fremitus • Check for a tracheal tug • Palpate Nodes http://www.ncbi.nlm.nih.gov/books/NBK368/ https://m.youtube.com/watch?v=uzgdaJCf0Mk Auscultation • Is there any air entry? • Differentiate – Normal vesicular sounds – Bronchial breathing – Wheeze – Distinguish crackles • Fine • Coarse • During inspiration or expiration • Profuse or scanty – Absent sounds – Vocal resonance http://www.easyauscultation.com/lung-sounds.aspx Percussion • Tapping of the middle phalanx of the left middle finger with the right middle finger • Sounds should be resonant but may be – Hyper resonant – Dull – Stony Dull http://stanfordmedicine25.stanford.edu/the25/pulmonary.html Pathological Expansion Mediastinal Percussion Breath Further Process Displacement Note Sounds Examination Consolidation Reduced on None Dull Bronchial affected side breathing Vocal resonance Whispering pectoriloquy Collapse Reduced on Towards Dull Reduced None affected side affected side Pleural Reduced on Towards Stony dull Reduced/ Occasional rub effusion affected side opposite side Absent Empyema Asthma Reduced None Resonant Normal/ Wheeze throughout Reduced COPD Reduced None Resonant/ Normal/ Wheeze throughout Hyper-resonant Reduced Pulmonary Normal or None Normal Normal Bibasal crepitations Fibrosis reduced throughout Pneumothorax Reduced on Towards Hyper-resonant Reduced/ None affected side opposite side Absent http://www.cram.com/flashcards/test/lung-sounds-886428 sign up and test yourself.. -

Inhalation of “Borax”
Journal of Paediatrics and Neonatal Disorders Volume 4 | Issue 1 ISSN: 2456-5482 Case Report Open Access Inhalation of “Borax” and Risk of Severe Stridor Obaid O* Department of Pediatrics, MOH, Makkah, Saudi Arabia *Corresponding author: Obaid O, Department of Pediatrics, MOH, Makkah, Saudi Arabia, Tel: 00966500606352, E-mail: [email protected] Citation: Obaid O (2019) Inhalation of “Borax” and Risk of Severe Stridor. J Paedatr Neonatal Dis 4(1): 105 Received Date: March 21, 2019 Accepted Date: June 26, 2019 Published Date: June 28, 2019 Abstract Stridor in children is not uncommon reason to visit emergency department and usually due to croup but inhalation of toxic substance may cause severe stridor which is uncommon. Keywords: Stridor; Pediatric; Sodium Burate Case Report A 9 year old Saudi girl presented to emergency department accompanied by her grandmother with history of dry cough, shortness of breath and audible wheeze for more than12 hours. She has no history of fever, foreign body ingestion and chronic cough. No history of contact with sick person and no history of lip swelling or skin rash. Her vaccination status up to date. She was a Preterm 30 weeks, admitted to Neonatal intensive care for 2 months and discharge well. In emergency room she was ill looking with biphasic stridor, kept on oxygen 10 liter/min and given one dose IM epinephrine 0.3 mg and nebulizer Racemic epinephrine, connected to Cardiorespiratory monitor and 2 IV lines was inserted started on IV Fluids and given one dose of dexamethasone. Urgent consultation to ENT was done and they recommend bronchoscopy to rule out Foreign body ingestion. -

Management of Airway Obstruction and Stridor in Pediatric Patients
November 2017 Management of Airway Volume 14, Number 11 Obstruction and Stridor in Authors Ashley Marchese, MD Department of Pediatrics, Yale-New Haven Hospital, New Haven, CT Pediatric Patients Melissa L. Langhan, MD, MHS Associate Professor of Pediatrics and Emergency Medicine; Fellowship Director, Director of Education, Pediatric Emergency Abstract Medicine, Yale University School of Medicine, New Haven, CT Peer Reviewers Stridor is a result of turbulent air-flow through the trachea from Steven S. Bin, MD upper airway obstruction, and although in children it is often Associate Clinical Professor of Emergency Medicine and Pediatrics; Medical Director, Emergency Department, UCSF School of Medicine, due to croup, it can also be caused by noninfectious and/or con- Benioff Children’s Hospital, San Francisco, CA genital conditions as well as life-threatening etiologies. The his- Alexander Toledo, DO, PharmD, FAAEM, FAAP tory and physical examination guide initial management, which Chief, Section of Pediatric Emergency Medicine; Director, Pediatric Emergency Department, Arizona Children’s Center at Maricopa includes reduction of airway inflammation, treatment of bacterial Medical Center, Phoenix, AZ infection, and, less often, imaging, emergent airway stabilization, Prior to beginning this activity, see “Physician CME Information” or surgical management. This issue discusses the most common on the back page. as well as the life-threatening etiologies of acute and chronic stridor and its management in the emergency department. Editor-in-Chief -
Pleurisy Dry and Exudative: Symptoms and Syndromes Based on Clinical-Instrumental and Laboratory Methods of Study
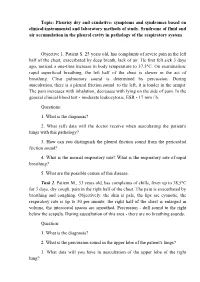
Topic: Pleurisy dry and exudative: symptoms and syndromes based on clinical-instrumental and laboratory methods of study. Syndrome of fluid and air accumulation in the pleural cavity in pathology of the respiratory system Objective 1. Patient S. 25 years old, has complaints of severe pain in the left half of the chest, exacerbated by deep breath, lack of air. He first felt sick 3 days ago, noticed a one-time increase in body temperature to 37,5°C. On examination: rapid superficial breathing, the left half of the chest is slower in the act of breathing. Clear pulmonary sound is determined by percussion. During auscultation, there is a pleural friction sound to the left, it is louder in the armpit. The pain increases with inhalation, decreases with lying on the side of pain. In the general clinical blood test - moderate leukocytosis, ESR - 17 mm / h. Questions: 1. What is the diagnosis? 2. What (all) data will the doctor receive when auscultating the patient's lungs with this pathology? 3. How can you distinguish the pleural friction sound from the pericardial friction sound? 4. What is the normal respiratory rate? What is the respiratory rate of rapid breathing? 5. What are the possible causes of this disease. Task 2. Patient M., 33 years old, has complaints of chills, fever up to 38,5°C for 3 days, dry cough, pain in the right half of the chest. The pain is exacerbated by breathing and coughing. Objectively: the skin is pale, the lips are cyanotic, the respiratory rate is up to 30 per minute, the right half of the chest is enlarged in volume, the intercostal spaces are smoothed. -

Clinical Usefulness of 'Vocal Fremitus' and 'Vocal Resonance'
RESEARCH Clinical usefulness of ‘vocal fremitus’ and ‘vocal resonance’ Kyaw San Hla MMedSc, MRCP, FRACP, is Senior Lecturer and staff physician, James Cook University, Mackay Base GP perceptions and practice Hospital, Queensland. kyaw. [email protected] Assessment of vocal fremitus (VF) and vocal resonance The study was approved by the Ethics Committee at Mackay (VR) (whereby vocal vibrations are felt or heard during Base Hospital. a clinical examination) is an established part of physical examination of the respiratory system. Textbooks on Results clinical examination include these procedures as part of Sixty-seven responses were obtained (64 GPs and three the standard method.1–3 general practice registrars), providing a response rate of approximately 70%. Forty-four respondents (65.7%) Undergraduate and postgraduate candidates are required rarely performed VF/VR as part of routine chest examination to perform VF and VR when they undertake qualifying (Figure 1). 50 44 assessments, however the reliability of findings from More than half (53.7%) 40 these procedures is controversial.4 It is also unusual to disagreed with the statement 30 see experienced doctors performing VF/VR during actual that ‘routine inclusion of either chest examination. The author of the only identifiable study VF or VR on chest examination Count 20 9 on clinicians’ attitudes toward VF/VR (which had only 14 is desirable’ (with 11.9% strongly 10 6 2 3 3 respondents) remarked ‘it will be rare to see physicians disagreeing). More than a quarter 0 near about about about about rarely doing both or even one of them although the majority has (28%) remained neutral. -

Chondrodysplasia Punctata: a Case Report of Fetal Warfarin Syndrome
J Nepal Health Res Counc 2017 Jan - Apr;15(35): 81-4 Case Report Chondrodysplasia Punctata: A Case Report of Fetal Warfarin Syndrome Swachchhanda Songmen,1 Om Biju Panta,2 Sharma Paudel S,1 Ram Kumar Ghimire1 1Department of Radiology and Imaging, Tribhuvan University Teaching Hospital, Kathmandu, Nepal, 2Department of Radiology and Imaging, Koshi Zonal Hospital, Morang, Nepal. ABSTRACT Chondrodysplasia punctata is abnormal calcification in the cartilage of developing bones and has been seen in association with deranged vitamin K metabolism. Warfarin, an oral anticoagulant acting on vitamin K dependent clotting factors is known to cause chondrodysplasia punctata. Despite the knowledge of the condition the management of patients with prosthetic heart valves might require use of the drug for anticoagulation. Here, we present a case of a fetal warfarin syndrome in a second born child of a 27 year lady under warfarin for prosthetic heart valve. The pregnancy was complicated by polyhydramnios in third trimester and terminated at term by normal vaginal delivery. The baby was well, except for facial dysmorphism in the form of depressed nasal bridge, narrow nares and suspected left choanal atresia. Radiograph revealed stippled ephiphysis of vertebra, femora and humera supporting diagnosis of fetal warfarin syndrome. The baby did not develop any perinatal complication and was discharged home. Keywords: Chondrodysplasia punctata; fetal warfarin syndrome; vitamin K deficiency. INTRODUCTION Her first baby was healthy term male with normal delivery Stippled epiphysis is seen in many acquired and inherited 4 years back. There is no past history of stillbirths. On disorders as drug exposure (warfarin and phenytoin), second (current) pregnancy, she took regular iron & metabolic disorders, trisomies (18, 21) and maternal calcium tablets but not folic acid. -

CHARGE Factsheet 3 Clinical Diagnosis and Features
The Information Pack CHARGE for Practitioners Factsheet 3 CHARGE syndrome: major and minor medical diagnostic criteria plus later onset features DR JEREMY KIRK, MD, FRCP, FRCPCH, Consultant Paediatric Endocrinologist, Birmingham Children’s Hospital Original diagnostic criteria The initial association of coloboma and choanal atresia with other congenital abnormalities was first described by Hall and separately Hittner et al. in 1979 (Hall, 1979; Hittner et al., 1979). In 1981 there was further description and expansion of the condition (Pagon et al., 1981). It was at this stage that the acronym CHARGE (C–coloboma, H–heart disease, A–atresia choanae, R–retarded growth and retarded development and/or CNS anomalies, G–genital hypoplasia, and E–ear anomalies and/or deafness) was made. In order to make the diagnosis of CHARGE syndrome, historically four out of six of the features of the acronym needed to be fulfilled, although one should be either choanal atresia or a coloboma (Pagon et al., 1981). From association to syndrome been several attempts to refine the diagnostic criteria, Initially CHARGE was described as an association; namely by Blake et al. (1998) and Verloes (2005). Both a nonrandom collection of birth defects, rather than of these use major features which are very specific for a syndrome, which is a more recognisable pattern of CHARGE syndrome, along with other minor features. birth defects (often with a known genetic cause). With the identification of the gene CHD7 in 2004 (Vissers The criteria suggested by Blake et al. consist of four et al., 2004) it has now been renamed a syndrome, major ‘C’s: as CHD7 is mutated in at least 60% of patients with 1. -

Domestic Violence: the Shaken Adult Syndrome
138 J Accid Emerg Med 2000;17:138–139 J Accid Emerg Med: first published as 10.1136/emj.17.2.139 on 1 March 2000. Downloaded from CASE REPORTS Domestic violence: the shaken adult syndrome T D Carrigan, E Walker, S Barnes Abstract Her initial blood pressure was 119/72 mm A case of domestic violence is reported. Hg, pulse 88 beats/min, her pupils were equal The patient presented with the triad of and reactive directly and consensually, and her injuries associated with the shaking of Glasgow coma score was 13/15 (she was infants: retinal haemorrhages, subdural confused and was opening her eyes to com- haematoma, and patterned bruising; this mand). Examination of the head showed bilat- has been described as the shaken adult eral periorbital ecchymoses, nasal bridge swell- syndrome. This case report reflects the ing and epistaxis, a right frontal abrasion, and diYculties in diagnosing domestic vio- an occipital scalp haematoma. Ecchymoses lence in the accident and emergency were also noted on her back and buttocks, setting. being linear in fashion on both upper arms, (J Accid Emerg Med 2000;17:138–139) and her underpants were torn. Initial skull and Keywords: domestic violence; women; assault facial x ray films were normal, and she was admitted under the care of A&E for neurologi- cal observations. Domestic violence is an under-reported and Over the next 24 hours, her Glasgow coma major public health problem that often first score improved to 15/15, but she had vomited presents to the accident and emergency (A&E) five times and complained that her vision department. -

Supraglottoplasty Home Care Instructions Hospital Stay Most Children Stay Overnight in the Hospital for at Least One Night
10914 Hefner Pointe Drive, Suite 200 Oklahoma City, OK 73120 Phone: 405.608.8833 Fax: 405.608.8818 Supraglottoplasty Home Care Instructions Hospital Stay Most children stay overnight in the hospital for at least one night. Bleeding There is typically very little to no bleeding associated with this procedure. Though very unlikely to happen, if your child were to spit or cough up blood you should contact your physician immediately. Diet After surgery your child will be able to eat the foods or formula that they usually do. It is important after surgery to encourage your child to drink fluids and remain hydrated. Daily fluid needs are listed below: • Age 0-2 years: 16 ounces per day • Age 2-4 years: 24 ounces per day • Age 4 and older: 32 ounces per day It is our experience that most children experience a significant improvement in eating after this procedure. However, we have found about that approximately 4% of otherwise healthy infants may experience a transient onset of coughing or choking with feeding after surgery. In our experience these symptoms resolve over 1-2 months after surgery. We have also found that infants who have other illnesses (such as syndromes, prematurity, heart trouble, or other congenital abnormalities) have a greater risk of experiencing swallowing difficulties after a supraglottoplasty (this number can be as high as 20%). In time the child usually will return to normal swallowing but there is a small risk of feeding difficulties. You will be given a prescription before you leave the hospital for an acid reducing (anti-reflux) medication that must be filled before you are discharged. -

Stridor in the Newborn
Stridor in the Newborn Andrew E. Bluher, MD, David H. Darrow, MD, DDS* KEYWORDS Stridor Newborn Neonate Neonatal Laryngomalacia Larynx Trachea KEY POINTS Stridor originates from laryngeal subsites (supraglottis, glottis, subglottis) or the trachea; a snoring sound originating from the pharynx is more appropriately considered stertor. Stridor is characterized by its volume, pitch, presence on inspiration or expiration, and severity with change in state (awake vs asleep) and position (prone vs supine). Laryngomalacia is the most common cause of neonatal stridor, and most cases can be managed conservatively provided the diagnosis is made with certainty. Premature babies, especially those with a history of intubation, are at risk for subglottic pathologic condition, Changes in voice associated with stridor suggest glottic pathologic condition and a need for otolaryngology referral. INTRODUCTION Families and practitioners alike may understandably be alarmed by stridor occurring in a newborn. An understanding of the presentation and differential diagnosis of neonatal stridor is vital in determining whether to manage the child with further observation in the primary care setting, specialist referral, or urgent inpatient care. In most cases, the management of neonatal stridor is outside the purview of the pediatric primary care provider. The goal of this review is not, therefore, to present an exhaustive review of causes of neonatal stridor, but rather to provide an approach to the stridulous newborn that can be used effectively in the assessment and triage of such patients. Definitions The neonatal period is defined by the World Health Organization as the first 28 days of age. For the purposes of this discussion, the newborn period includes the first 3 months of age. -

Snoring and Stertor Are Associated with More Sleep Disturbance Than Apneas and Hypopneas in Pediatric SDB
Sleep and Breathing (2019) 23:1245–1254 https://doi.org/10.1007/s11325-019-01809-3 SLEEP BREATHING PHYSIOLOGY AND DISORDERS • ORIGINAL ARTICLE Snoring and stertor are associated with more sleep disturbance than apneas and hypopneas in pediatric SDB Mark B. Norman1 & Henley C. Harrison2 & Karen A. Waters1,3 & Colin E. Sullivan1,3 Received: 2 November 2018 /Revised: 26 January 2019 /Accepted: 19 February 2019 /Published online: 1 March 2019 # The Author(s) 2019 Abstract Purpose Polysomnography is not recommended for children at home and does not adequately capture partial upper airway obstruction (snoring and stertor), the dominant pathology in pediatric sleep-disordered breathing. New methods are required for assessment. Aims were to assess sleep disruption linked to partial upper airway obstruction and to evaluate unattended Sonomat use in a large group of children at home. Methods Children with suspected obstructive sleep apnea (OSA) had a single home-based Sonomat recording (n = 231). Quantification of breath sound recordings allowed identification of snoring, stertor, and apneas/hypopneas. Movement signals were used to measure quiescent (sleep) time and sleep disruption. Results Successful recordings occurred in 213 (92%) and 113 (53%) had no OSA whereas only 11 (5%) had no partial obstruc- tion. Snore/stertor occurred more frequently (15.3 [5.4, 30.1] events/h) and for a longer total duration (69.9 min [15.7, 140.9]) than obstructive/mixed apneas and hypopneas (0.8 [0.0, 4.7] events/h, 1.2 min [0.0, 8.5]); both p < 0.0001. Many non-OSA children had more partial obstruction than those with OSA.