Arm Care for the Youth Pitcher
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Coaches Drill Book
1 WEBSITES AND VIDEO LINKS If you are looking for more baseball specific coaching information, here are some websites and video links that may help: Websites Baseball Canada NCCP - https://nccp.baseball.ca/ Noblesville Baseball (Indiana) – Drill page - http://www.noblesvillebaseball.org/Default.aspx?tabid=473779 Team Snap - https://www.teamsnap.com/community/skills-drills/category/baseball QC Baseball - http://www.qcbaseball.com/ Baseball Coaching 101 - http://www.baseballcoaching101.com/ Pro baseball Insider - http://probaseballinsider.com/ Video Links Baseball Canada NCCP - https://nccp.baseball.ca/ (use the tools section and select drill library) USA Baseball Academy - http://www.youtube.com/user/USBaseballAcademy Coach Mongero – Winning Baseball - http://www.youtube.com/user/coachmongero IMG Baseball Academy - https://www.youtube.com/watch?v=b-NuHbW38vc&list=PLuLT- JCcPoJnl82I_5NfLOLneA2j3TkKi Baseball Manitoba Sport Development Programs: The Rally Cap program will service the 4 – 7 My First Pitch is a program targeted at the age group, and involves three teams of six development of pitchers entering the 11U players that meet at the park at the same time. division where pitching is introduced for the first time. Grand Slam is the follow-up program to Rally The Mosquito Monster Mania is a fun one day Cap and is meant for players aged 8 and 9. event for Mosquito “A” teams and players that The season ends with a Regional Jamboree are not competing in League or regional and a Provincial Jamboree at Shaw Park in championship. July. The Spring Break Baseball Camp for ages 6- The Winter Academy is a baseball skill 12 runs for one week, offering complete skill development camp to prepare for the season development. -

Jan-29-2021-Digital
Collegiate Baseball The Voice Of Amateur Baseball Started In 1958 At The Request Of Our Nation’s Baseball Coaches Vol. 64, No. 2 Friday, Jan. 29, 2021 $4.00 Innovative Products Win Top Awards Four special inventions 2021 Winners are tremendous advances for game of baseball. Best Of Show By LOU PAVLOVICH, JR. Editor/Collegiate Baseball Awarded By Collegiate Baseball F n u io n t c a t REENSBORO, N.C. — Four i v o o n n a n innovative products at the recent l I i t y American Baseball Coaches G Association Convention virtual trade show were awarded Best of Show B u certificates by Collegiate Baseball. i l y t t nd i T v o i Now in its 22 year, the Best of Show t L a a e r s t C awards encompass a wide variety of concepts and applications that are new to baseball. They must have been introduced to baseball during the past year. The committee closely examined each nomination that was submitted. A number of superb inventions just missed being named winners as 147 exhibitors showed their merchandise at SUPERB PROTECTION — Truletic batting gloves, with input from two hand surgeons, are a breakthrough in protection for hamate bone fractures as well 2021 ABCA Virtual Convention See PROTECTIVE , Page 2 as shielding the back, lower half of the hand with a hard plastic plate. Phase 1B Rollout Impacts Frontline Essential Workers Coaches Now Can Receive COVID-19 Vaccine CDC policy allows 19 protocols to be determined on a conference-by-conference basis,” coaches to receive said Keilitz. -

Analysis of Softball Pitching (PDF)
1 Softball Pitching Technique Marion J.L. Alexander, PhD. Carolyn Taylor, MSc Sport Biomechanics Laboratory Faculty of Kinesiology and Recreation Management University of Manitoba Softball Pitching Technique Softball pitching is the most important skill in the game of softball, as the pitcher can dominate as no other player is able to do. Softball is usually a low scoring game in which only one or two runs are scored during the entire game, often due to the dominance of a highly skilled pitcher. Pitchers require several years to perfect their technique and gain control over the speed and direction of their pitches. Softball pitchers use an underhand motion that is not as stressful to the shoulder joint as the overhand pitch used in baseball. Softball pitchers can often pitch several games in one day, and often have an extended career of many years due to the lower stress levels on the shoulder joint. A softball pitcher may pitch as many as six 7-inning games during a weekend tournament; and often the best pitcher on a college team pitches most, if not all of the games each season (Werner, Guido et al. 2005). This may result in approximately 1200-1500 pitches being thrown in a 3-day period for a windmill pitcher, as compared to 100-150 for a baseball pitcher (Werner, Guido et al. 2005). The softball pitch is a relatively simple motion, consisting of a step forward from the mound onto the foot on the non pitching arm side, weight shift onto this foot, and rotation of the shoulders and trunk to a position facing the batter. -

Describing Baseball Pitch Movement with Right-Hand Rules
Computers in Biology and Medicine 37 (2007) 1001–1008 www.intl.elsevierhealth.com/journals/cobm Describing baseball pitch movement with right-hand rules A. Terry Bahilla,∗, David G. Baldwinb aSystems and Industrial Engineering, University of Arizona, Tucson, AZ 85721-0020, USA bP.O. Box 190 Yachats, OR 97498, USA Received 21 July 2005; received in revised form 30 May 2006; accepted 5 June 2006 Abstract The right-hand rules show the direction of the spin-induced deflection of baseball pitches: thus, they explain the movement of the fastball, curveball, slider and screwball. The direction of deflection is described by a pair of right-hand rules commonly used in science and engineering. Our new model for the magnitude of the lateral spin-induced deflection of the ball considers the orientation of the axis of rotation of the ball relative to the direction in which the ball is moving. This paper also describes how models based on somatic metaphors might provide variability in a pitcher’s repertoire. ᭧ 2006 Elsevier Ltd. All rights reserved. Keywords: Curveball; Pitch deflection; Screwball; Slider; Modeling; Forces on a baseball; Science of baseball 1. Introduction The angular rule describes angular relationships of entities rel- ative to a given axis and the coordinate rule establishes a local If a major league baseball pitcher is asked to describe the coordinate system, often based on the axis derived from the flight of one of his pitches; he usually illustrates the trajectory angular rule. using his pitching hand, much like a kid or a jet pilot demon- Well-known examples of right-hand rules used in science strating the yaw, pitch and roll of an airplane. -

Name of the Game: Do Statistics Confirm the Labels of Professional Baseball Eras?
NAME OF THE GAME: DO STATISTICS CONFIRM THE LABELS OF PROFESSIONAL BASEBALL ERAS? by Mitchell T. Woltring A Thesis Submitted in Partial Fulfillment of the Requirements for the Degree of Master of Science in Leisure and Sport Management Middle Tennessee State University May 2013 Thesis Committee: Dr. Colby Jubenville Dr. Steven Estes ACKNOWLEDGEMENTS I would not be where I am if not for support I have received from many important people. First and foremost, I would like thank my wife, Sarah Woltring, for believing in me and supporting me in an incalculable manner. I would like to thank my parents, Tom and Julie Woltring, for always supporting and encouraging me to make myself a better person. I would be remiss to not personally thank Dr. Colby Jubenville and the entire Department at Middle Tennessee State University. Without Dr. Jubenville convincing me that MTSU was the place where I needed to come in order to thrive, I would not be in the position I am now. Furthermore, thank you to Dr. Elroy Sullivan for helping me run and understand the statistical analyses. Without your help I would not have been able to undertake the study at hand. Last, but certainly not least, thank you to all my family and friends, which are far too many to name. You have all helped shape me into the person I am and have played an integral role in my life. ii ABSTRACT A game defined and measured by hitting and pitching performances, baseball exists as the most statistical of all sports (Albert, 2003, p. -
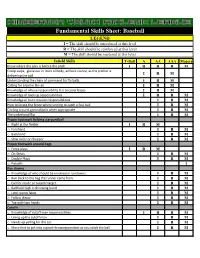
Fundamental Skills Sheet: Baseball
Fundamental Skills Sheet: Baseball LEGEND I = The skill should be introduced at this level R = The skill should be reinforced at this level M = The skill should be mastered at this level Infield Skills T-Ball A AA AAA Majors Know where the play is before the pitch I R R R M Creep steps, glove out in front of body, athletic stance, as the pitcher is I R M delivering the ball Understanding the chain of command for fly balls I R M Calling for a ball in the air I R M Knowledge of whose responsibility it is to cover bases I R M Knowledge of back up responsibilities I R R M Knowledge of bunt rotation responsibilities I R M How to locate the fence when running to catch a foul ball I R M Circling around ground balls when appropriate I R M The underhand flip I R M Proper footwork fielding a groundball o Right at the fielder I R M o Forehand I R M o Backhand I R M o Slow roller or chopper I R M Proper footwork around bags o Force plays I R M o On Steals I R M o Double Plays I R M o Pickoffs I Run downs o Knowledge of who should be involved in rundowns I R M o Run back to the bag the runner came from I R M o Call for inside or outside target I R M o Ball held high in throwing hand I R M o Limit pump fakes I R M o Follow throw I R M o Tag with two hands I R M Cutoffs o Knowledge of cutoff man responsibilities I R R M o Lining up the cutoff man I R M o Hands up yelling for the cut I R M o Move feet to get into a good throwing position as you catch the ball I R M Outfield Skills T-Ball A AA AAA Majors Know where the play is before the pitch I R R R -

Key Concepts for Injury Prevention in Baseball Players
Baseball Key Concepts for Injury Prevention What kind of injuries occur in baseball? Traumatic injuries occur suddenly. These are typically prevented with proper equipment, rules, regulations and fair play. Overuse injuries occur over time. These can be prevented by knowing early warning signs, general conditioning and following recommendations for rest. What is forced rest? Body tissues can become worn out and painful when they get too much stress with certain activities. Forced rest is taking a strategic break from motions or activities that cause damage and sometimes pain. What else can be done to reduce injury risk in baseball? • Avoid playing on multiple teams in one season • Be smart about side session work, this counts toward pitch counts too. • Play multiple sports • Take 2-3 months off from pitching each year • Cross train during season and in the off-season • Ramp up slowly in pre-season Cross training ideas for young baseball players? • Flexibility exercises • Sprinting drills • Strength training with body resistance • Core stabilization and shoulder blade stabilization Who is more likely to get an overuse injury? • Pitchers that also play in other heavy throwing positions when not pitching, i.e. catcher, shortstop • Pitchers who play year-round or on multiple teams • Players who continue throwing through fatigue and/or pain. 469-515-7100 • scottishritehospital.org Continued on reverse Baseball Training Tips Balance baseball skills training with cross training. Focus on Proper Technique Age Recommended for • HOW is as important as HOW MANY Learning Various Pitches • Too many pitches leads to fatigue and poor form Pitch Age • Limiting total pitch count allows proper technique Fastball 8 during practice and games Change-up 10 See Little League recommendations for pitch counts and rest periods Curveball 14 Flexibility Exercises Knuckleball 15 Dynamic stretching activities or static stretching of major Slider 16 muscle groups including: hamstring, calf, shoulder, trunk Forkball 16 rotation. -

Getting Back Baseball Legs Layout 1
ERFORMANCE P BASEBALL/SOFTBALL CONDITIONING A NEWSLETTER DEDICATED TO IMPROVING BASEBALL AND SOFTBALL PLAYERS www.performancecondition.com/baseballsoftball Getting Back Baseball Legs— The Transition from Off-Season Training Joe Kessler, Strength and Conditioning Coach, Cleveland Indians Joe is in his third season as the Major League Strength and running, fielding and other baseball activity, we get players who start Conditioning Coach after being named to the position on January to complain of soreness/tightness in the back area. As a result, the 8, 2010. volume and intensity of the strength and conditioning program is Kessler, 30, originally joined the Indians organization in altered through exercise selection. The program complements the March of 2009. He spent the 2009 season as an Assistant Strength reorientation process rather than adding undue stress to the athlete and Conditioning Coach in Goodyear, Arizona based on what the players show me in movement pattern deficiencies. where he worked with players based out of the This becomes the focus of what we accomplish at this time so that Goodyear complex and assisted those who good movement habits are created early and last through the entire sea- were rehabilitating from previous injuries. son. Kessler’s previous experience includes two years as the Director of Athletic Develop- Program considerations—the all-important first ten days ment for OAK Athletic Development in We treat position players different than pitchers. This is es- Bourbonnais, IL and also spent two pecially true in the first ten days. We get the jump on pitchers and seasons as a Strength and Condition- catchers because they report earlier. -

National Pastime a REVIEW of BASEBALL HISTORY
THE National Pastime A REVIEW OF BASEBALL HISTORY CONTENTS The Chicago Cubs' College of Coaches Richard J. Puerzer ................. 3 Dizzy Dean, Brownie for a Day Ronnie Joyner. .................. .. 18 The '62 Mets Keith Olbermann ................ .. 23 Professional Baseball and Football Brian McKenna. ................ •.. 26 Wallace Goldsmith, Sports Cartoonist '.' . Ed Brackett ..................... .. 33 About the Boston Pilgrims Bill Nowlin. ..................... .. 40 Danny Gardella and the Reserve Clause David Mandell, ,................. .. 41 Bringing Home the Bacon Jacob Pomrenke ................. .. 45 "Why, They'll Bet on a Foul Ball" Warren Corbett. ................. .. 54 Clemente's Entry into Organized Baseball Stew Thornley. ................. 61 The Winning Team Rob Edelman. ................... .. 72 Fascinating Aspects About Detroit Tiger Uniform Numbers Herm Krabbenhoft. .............. .. 77 Crossing Red River: Spring Training in Texas Frank Jackson ................... .. 85 The Windowbreakers: The 1947 Giants Steve Treder. .................... .. 92 Marathon Men: Rube and Cy Go the Distance Dan O'Brien .................... .. 95 I'm a Faster Man Than You Are, Heinie Zim Richard A. Smiley. ............... .. 97 Twilight at Ebbets Field Rory Costello 104 Was Roy Cullenbine a Better Batter than Joe DiMaggio? Walter Dunn Tucker 110 The 1945 All-Star Game Bill Nowlin 111 The First Unknown Soldier Bob Bailey 115 This Is Your Sport on Cocaine Steve Beitler 119 Sound BITES Darryl Brock 123 Death in the Ohio State League Craig -

Mlb the Show 17 Pc Iso Download Free MLB the Show 21 Torrent Download PC Game
mlb the show 17 pc iso download free MLB The Show 21 Torrent Download PC Game. How do you want to own the show? In a nail-biting competitive game or maybe a chill game where you can kick back and watch the dingers roll in. No matter what you’re playstyle MLB The Show 21 has you covered. MLB The Show 21 will feature cross-platform multiplayer, so you can play against anyone, regardless of what console they’re using. It also supports “cross progression,” which lets you pick up where you left off on another platform, even if it’s a different console generation. MLB The Show 19 PC Download Free Full Version [2021 Updated] MLB The Show 19 PC Download is a real-time strategy game developed in 2019 by Sony Interactive Entertainment for Windows and PlayStation 4 . Overview. MLB The Show 19 is out of nowhere ends up in a phenomenal position. The COVID-19 coronavirus has disturbed games over the globe, and baseball is the same, like Opening Day of the 2020 Major League Baseball season was as of late deferred for in any event the following two months and even that appears to be hopeful. It’s an unbelievable unforeseen development, yet it likewise implies Sony San Diego’s most recent baseball sim is presently one of the main approaches to encounter the 2020 period of America’s preferred side interest. It’s a great job, at that point, that MLB 20 keeps up the arrangement’s reliably high caliber. Refinements to handling and hitting may just be steady this year, yet they add more profundity to what is as yet one of the most convincing sporting events available, while new options and modes off the field increment the game’s assortment as you diagram a course towards World Series greatness. -

Hitting Approach
Hitting Approach By Scott Brosius With the start of the upcoming season right around the corner, coaches start to spend a lot of time thinking, and in some cases worrying, about their team’s offensive performance. We ask questions such as. “Are we going to hit this year?” and “how can we make these guys better”. Hitting is a huge concern for coaches and we dedicate a lot of time to offense in our practices. So what makes good hitters good? What do they do? What do they think? As part one of a two-part series on hitting, this article will focus on basic hitting approaches while part two will focus on drills and practice work we can do to implement our approach. Why start with approach? Because as coaches we can’t put the cart ahead of the horse when it comes to teaching our players. So many times at the start of the season coaches break out the balls and bats, get their players in a circle, give them a little talk on proper hitting mechanics, then send them in the cages to go to work. Guys will take hundreds and hundreds of swings to master these mechanics, but when the games start they have no idea how to take a quality at- bat. As coaches we need to take a step back and spend some time with our players, before they take their first swing, and provide them with an offensive approach or thought process. And I believe there are 3 simple thoughts all good hitters have in common. -

Dynamical Chaos in a Simple Model of a Knuckleball
Dynamical Chaos in a Simple Model of a Knuckleball Nicholas J. Nelson, Eric Strauss Department of Physics California State University, Chico 400 W. 1st St. Chico, CA 95929 Abstract The knuckleball is perhaps the most enigmatic pitch in baseball. Relying on the presence of raised seams on the surface of the ball to create asymmetric flow, a knuckleball's trajectory has proven very challenging to predict compared to other baseball pitches, such as fastballs or curveballs. Previous experimental tracking of large numbers of knuckleballs has shown that they can move in essentially any direction relative to what would be expected from a drag-only trajectory. This has led to speculation that knuckleballs exhibit chaotic motion. Here we develop a relatively simple model of a knuckleball that includes quadratic drag and lift from asymmetric flow which is taken from experimental measurements of slowly rotating baseballs. Our models can indeed exhibit dynamical chaos as long In contrast, models that omit torques on the ball in flight do not show chaotic behavior. Uncertainties in the phase space position of the knuckleball are shown to grow by factors as large as 106 over the flight of the ball from the pitcher to home plate. We quantify the impact of our model parameters on the chaos realized in our models, specifically showing that maximum Lyapunov exponent is roughly proportional to the square root of the effective lever arm of the torque, and also roughly proportional to the initial velocity of the pitch. We demonstrate the existence of bifurcations that can produce changes in the location of the ball when it reaches the plate of as much as 1.2 m for specific initial conditions similar to those used by professional knuckleball pitchers.