Sample of Penicillin Mould Presented by Alexander Fleming to Douglas Macleod, 1935
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
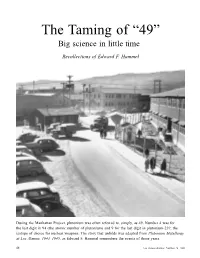
The Taming of “49” Big Science in Little Time
The Taming of “49” Big science in little time Recollections of Edward F. Hammel During the Manhattan Project, plutonium was often referred to, simply, as 49. Number 4 was for the last digit in 94 (the atomic number of plutonium) and 9 for the last digit in plutonium-239, the isotope of choice for nuclear weapons. The story that unfolds was adapted from Plutonium Metallurgy at Los Alamos, 1943–1945, as Edward F. Hammel remembers the events of those years. 48 Los Alamos Science Number 26 2000 The Taming of “49” he work in plutonium chemistry tion work was an inevitable conse- the metal could be fabricated into and metallurgy carried out at quence of the nuclear and physical satisfactory weapon components. TLos Alamos (Site Y) between research that was still to be conducted In addition, not until January 1944 1943 and 1945 had a somewhat contro- on the metal. It would clearly have did the first few milligrams of pile- versial history. The controversy was been inefficient and time consuming to produced plutonium arrive at Los about who was going to do what. ship small amounts of plutonium metal Alamos. The first 1-gram shipment At the time Los Alamos was being back to Chicago for repurification and arrived in February 1944, and quantity organized, most of the expertise in plu- refabrication into different sizes and shipments of plutonium did not begin to tonium chemistry resided at Berkeley, shapes for the next-scheduled nuclear arrive at Los Alamos until May 1945. where plutonium was discovered in physics experiment. From the outset, it was clear that the December 1940, and at the Met Lab in Minimizing the time spent to solve purification of plutonium was the most Chicago. -
Fleming Vs. Florey: It All Comes Down to the Mold Kristin Hess La Salle University
The Histories Volume 2 | Issue 1 Article 3 Fleming vs. Florey: It All Comes Down to the Mold Kristin Hess La Salle University Follow this and additional works at: https://digitalcommons.lasalle.edu/the_histories Part of the History Commons Recommended Citation Hess, Kristin () "Fleming vs. Florey: It All Comes Down to the Mold," The Histories: Vol. 2 : Iss. 1 , Article 3. Available at: https://digitalcommons.lasalle.edu/the_histories/vol2/iss1/3 This Paper is brought to you for free and open access by the Scholarship at La Salle University Digital Commons. It has been accepted for inclusion in The iH stories by an authorized editor of La Salle University Digital Commons. For more information, please contact [email protected]. The Histories, Vol 2, No. 1 Page 3 Fleming vs. Florey: It All Comes Down to the Mold Kristen Hess Without penicillin, the world as it is known today would not exist. Simple infections, earaches, menial operations, and diseases, like syphilis and pneumonia, would possibly all end fatally, shortening the life expectancy of the population, affecting everything from family-size and marriage to retirement plans and insurance policies. So how did this “wonder drug” come into existence and who is behind the development of penicillin? The majority of the population has heard the “Eureka!” story of Alexander Fleming and his famous petri dish with the unusual mold growth, Penicillium notatum. Very few realize that there are not only different variations of the Fleming discovery but that there are also other people who were vitally important to the development of penicillin as an effective drug. -

The Expert Panel on the Socio-Economic Impacts of Innovation Investments
INNOVATION IMPACTS: MEASUREMENT AND ASSESSMENT The Expert Panel on the Socio-economic Impacts of Innovation Investments Science Advice in the Public Interest INNOVATION IMPACTS: MEASUREMENT AND ASSESSMENT The Expert Panel on the Socio-economic Impacts of Innovation Investments ii Innovation Impacts: Measurement and Assessment THE COUNCIL OF CANADIAN ACADEMIES 180 Elgin Street, Suite 1401, Ottawa, ON Canada K2P 2K3 Notice: The project that is the subject of this report was undertaken with the approval of the Board of Governors of the Council of Canadian Academies. Board members are drawn from the Royal Society of Canada (RSC), the Canadian Academy of Engineering (CAE), and the Canadian Academy of Health Sciences (CAHS), as well as from the general public. The members of the expert panel responsible for the report were selected by the Council for their special competencies and with regard for appropriate balance. This report was prepared in response to a request from the Ontario Ministry of Research and Innovation. Any opinions, findings, or conclusions expressed in this publication are those of the authors, the Expert Panel on the Socio-economic Impacts of Innovation Investments, and do not necessarily represent the views of their organizations of affiliation or employment. Library and Archives Canada Cataloguing in Publication Innovation impacts: measurement and assessment [electronic resource] : socio-economic impacts of innovation investments of the government of Ontario/ Council of Canadian Academies. Includes bibliographical references and index. Electronic monograph in PDF format. Issued also in print format. ISBN 978-1-926558-58-5 1. Public investments – Ontario – Measurement. 2. Public investments – Ontario – Evaluation. 3. Technological innovations – Government policy – Ontario. -

The Bradbury Years 1943-1945
THE n late 1945 a small group of courageous and loyal scientists and technicians undertook to continue the post-war operation of the Los Alamos Scientific Laboratory. These men believed that atomic weapons development had barely begun, that other countries would develop such weapons, and that the safety and security of the United States-if not of the world-depended upon the technical lead of this country. These men had the courage to stay at Los Alamos in the face of an uncertain future. These men did not make demands nor require promises. These men stayed and built the greatest weapons laboratory this country has ever known. These men stayed and developed the greatest array of powerful and flexible atomic weapons of any country in the world-developed them faster, developed them where they were urgently needed and requested by the Armed Forces-developed them to fit the productive resources of the newly established Atomic Energy Commission. They stayed and built a laboratory that developed every successfuZ thermonuclear weapon that exists today. Others left, but these men stayed and worked, and many others came to join them. LOS ALAMOS SCIENCE WinterISpring 1983 What these men accomplished cannot be told in detail, for these its developments while it was further expanding its scientific staff. facts are classified TOP SECRET. These men do not talk. They Had the Laboratory attempted to exploit the thermonuclear field believe in deeds, not words. But these deeds earned for the Los to the exclusion of the fission field in 1946, what would have Alamos Scientific Laboratory the only Presidential Citation ever happened? Hypothetical history can only be an educated guess, but awarded to any laboratory for its extraordinary success in the the guess in this case is almost certain. -
Can Nuclear Weapons Fallout Mark the Beginning of the Anthropocene
Feature Bulletin of the Atomic Scientists 2015, Vol. 71(3) 46–57 ! The Author(s) 2015 Reprints and permissions: Can nuclear weapons fallout sagepub.co.uk/journalsPermissions.nav DOI: 10.1177/0096340215581357 mark the beginning of the http://thebulletin.sagepub.com Anthropocene Epoch? Colin N. Waters, James P. M. Syvitski, Agnieszka Gałuszka, Gary J. Hancock, Jan Zalasiewicz, Alejandro Cearreta, Jacques Grinevald, Catherine Jeandel, J. R. McNeill, Colin Summerhayes, and Anthony Barnosky Abstract Many scientists are making the case that humanity is living in a new geological epoch, the Anthropocene, but there is no agreement yet as to when this epoch began. The start might be defined by a historical event, such as the beginning of the fossil-fueled Industrial Revolution or the first nuclear explosion in 1945. Standard strati- graphic practice, however, requires a more significant, globally widespread, and abrupt signature, and the fallout from nuclear weapons testing appears most suitable. The appearance of plutonium 239 (used in post- 1945 above-ground nuclear weapons tests) makes a good marker: This isotope is rare in nature but a significant component of fallout. It has other features to recommend it as a stable marker in layers of sedimentary rock and soil, including: long half-life, low solubility, and high particle reactivity. It may be used in conjunction with other radioactive isotopes, such as americium 241 and carbon 14, to categorize distinct fallout signatures in sediments and ice caps. On a global scale, the first appearance of plutonium 239 in sedimentary sequences corresponds to the early 1950s. While plutonium is easily detectable over the entire Earth using modern meas- urement techniques, a site to define the Anthropocene (known as a Ògolden spikeÓ) would ideally be located between 30 and 60 degrees north of the equator, where fallout is maximal, within undisturbed marine or lake environments. -

The July 1945 Szilard Petition on the Atomic Bomb
1 The July 1945 Szilard Petition on the Atomic Bomb Memoir by a signer in Oak Ridge Howard Gest Distinguished Professor Emeritus of Microbiology, Departments of Biology, and History & Philosophy of Science, Indiana University, Bloomington, IN 47405 2 Well before the first test of a nuclear explosive device at Alamogordo (New Mexico) on July 16, 1945, many scientists of the Manhattan (Atomic Bomb) Project were very concerned about how nuclear bombs might be used in World War II. Meetings were held at the University of Chicago site and at Oak Ridge (Tennessee) to discuss the future of atomic energy and its political implications. As a result, a petition originated by Leo Szilard and addressed to President Truman in July 1945 discussed the moral responsibilities involved in using nuclear weapons. It recommended that such bombs not be used against Japan “unless the terms which will be imposed upon Japan have been made public in detail and Japan knowing these terms has refused to surrender.” The Szilard petition was displayed during 1989/1990 in a special exhibition at the National Archives in Washington, D.C. This article explains how I happened to be in Oak Ridge, where I signed the petition, and examines its background and complex, unfortunate history. From bacteriology to nuclear chemistry After graduating from the University of California at Los Angeles (UCLA) in 1942, with a major in bacteriology, I began graduate work with Max Delbrück at Vanderbilt University in Nashville, Tennessee (Delbrück was awarded a Nobel Prize in 1969 for his research on bacterial viruses). Because of the increasing intensity of World War II in 1942, however, research in universities was grinding to a halt. -

Fact Sheet: the Challenge of Mass Production
Fact Sheet: The Challenge of Mass Production Discovery Sir Alexander Fleming discovered the bacteria-killing properties of penicillin while conducting research at St. Mary’s Hospital in London in 1928. Upon returning to his disorganized lab from a weekend vacation, Fleming noticed that one of the Petri dishes was uncovered and a blue-green mold was growing inside. Rather than tossing the contaminated dish into the trash, he looked carefully and observed that the mold had killed bacteria growing nearby. Quite by accident Fleming had discovered penicillin, the antibiotic released by the mold of the genus Penicillium. Alexander Fleming’s original photograph of the contaminated dish. Alexander Fleming was well acquainted with the treatment of bacterial infections after spending World War I as a captain in the British Medical Corps. He witnessed firsthand the lack of medicine to treat infections, with disease causing approximately one third of military deaths during the Great War. Despite its historical significance, Fleming’s discovery of penicillin in 1928 brought little attention. The technology and funding needed to isolate and produce the antibiotic was lacking at the time. Fleming, however, continued to grow the Penicillium notatum strain in his lab for twelve years, distributing it to scientists and saving the specimen for someone willing and able to transform the “mold juice” into a medicine suitable for human use. Purification and Trials Meanwhile, Australian scientist Howard Florey hired Ernst Chain to help with his microbiology research at Oxford University. Florey and Chain were interested in Alexander Fleming’s work and in 1938, began studying the antibacterial properties of mold. -

Facts About Plutonium by Alina Bradford, Live Science Contributor | December 7, 2016 09:30Pm ET
Facts About Plutonium By Alina Bradford, Live Science Contributor | December 7, 2016 09:30pm ET Plutonium is a radioactive, silver metal that can be used to create or destroy. While it was used for destruction soon after it was made, today the element is used mostly for creating energy throughout the world. Plutonium was first produced and isolated in 1940 and was used to make the "Fat Man" atomic bomb that was dropped on Nagasaki at the end of World War II, just five years after it was first produced, said Amanda Simson, an assistant professor of chemical engineering at the University of New Haven. Just the facts Here are the properties of plutonium, according to the Los Alamos National Laboratory: Atomic number: 94 Atomic symbol: Pu Atomic weight: 244 Melting point: 1,184 F (640 C) Boiling point: 5,842 F (3,228 C) Discovery & history Plutonium was discovered in 1941 by scientists Joseph W. Kennedy, Glenn T. Seaborg, Edward M. McMillan and Arthur C. Wohl at the University of California, Berkley. The discovery occurred when the team bombarded uranium-238 with deuterons that had been accelerated in a cyclotron device, which created neptunium-238 and two free neutrons. The neptunium-238 then decayed into plutonium-238 through beta decay. This experiment wasn't shared with the rest of the scientific community until 1946, after World War II. Seaborg submitted a paper on their discovery to the journal Physical Review in March 1941, but the paper was removed when it was discovered that an isotope of plutonium, Pu-239, may be used to create an atomic bomb. -

Instructions to the PRTF
FINAL NOAA Science Advisory Board Research and Development Portfolio Review Task Force Additional Information Scope The functional scope of this study should include those activities commonly referred to as “research and development,” though which NOAA improves the conduct of its mission, i.e., through which NOAA innovates. It should also consider the transfer of knowledge and technology that results from R&D to its intended application. The study is not scoped by the activities of “science” per se, and thus will not focus on scientific activities that are part of regular NOAA operations (e.g., producing a weather forecast, collecting tide measurements). The study may consider the use of operational activities and infrastructure that also support R&D as necessary to answer the questions above. Research and development (R&D) at NOAA is defined consistent with the definitions used by the National Science Foundation (NSF, 2009), and as originated by Vannevar Bush (1945) in Science: The Endless Frontier. NOAA has adopted the official NOAA/NSF definitions to conform to government-wide practices, but discourages the distinction between basic and applied research, which derives from an oversimplified, linear model of innovation from the post-war era. Instead, NOAA encourages use of Stokes’s (1997) more contemporary model of innovation, Pasteur’s Quadrant, for framing analysis (see figure below), in which research can be directed toward fundamental understanding (“pure basic”) ultimate use (“pure applied”), or both (“use- inspired”). R&D includes research, development, demonstration, and R&D plant. Research, development, and R&D plant include all direct, incidental, or related costs resulting from, or necessary to, performance of research and development, and costs of R&D plant (as defined in Appendix 2, below), regardless of whether the research and development are 1 FINAL performed by a Federal agency (intramurally) or performed by private individuals and organizations under grant or contract (extramurally). -

A Study of Federal Academic Earmarks and Research Funding In
The University of Southern Mississippi The Aquila Digital Community Dissertations Fall 12-2013 A Study of Federal Academic Earmarks and Research Funding in Relation to the Institutional Research Culture of Research University/High (RU/H) Institutions in Mississippi James Hubert Young III University of Southern Mississippi Follow this and additional works at: https://aquila.usm.edu/dissertations Part of the Higher Education Commons Recommended Citation Young, James Hubert III, "A Study of Federal Academic Earmarks and Research Funding in Relation to the Institutional Research Culture of Research University/High (RU/H) Institutions in Mississippi" (2013). Dissertations. 221. https://aquila.usm.edu/dissertations/221 This Dissertation is brought to you for free and open access by The Aquila Digital Community. It has been accepted for inclusion in Dissertations by an authorized administrator of The Aquila Digital Community. For more information, please contact [email protected]. The University of Southern Mississippi A STUDY OF FEDERAL ACADEMIC EARMARKS AND RESEARCH FUNDING IN RELATION TO THE INSTITUTIONAL RESEARCH CULTURE OF RESEARCH UNIVERSITY/HIGH (RU/H) INSTITUTIONS IN MISSISSIPPI by James Hubert Young III Abstract of a Dissertation Submitted to the Graduate School of The University of Southern Mississippi in Partial Fulfillment of the Requirements for the Degree of Doctor of Philosophy December 2013 ABSTRACT A STUDY OF FEDERAL ACADEMIC EARMARKS AND RESEARCH FUNDING IN RELATION TO THE INSTITUTIONAL RESEARCH CULTURE OF RESEARCH UNIVERSITY/HIGH (RU/H) INSTITUTIONS IN MISSISSIPPI by James Hubert Young, III December 2013 Nationally, reductions in public funding for higher education, a stagnate economy, looming sequestration, and a divisive political culture present a complex and challenging dynamic for research universities in pursuit of external funding for their research programs and infrastructure needs. -

Penicillin…He Will Come Home!” the Challenge of Mass Production
“Thanks to Penicillin…He Will Come Home!” The Challenge of Mass Production A Lesson Plan from The Education Department The National WWII Museum 945 Magazine Street New Orleans, LA 70130 (504) 528-1944 www.nationalww2museum.org © The National WWII Museum Thanks to Penicillin… He Will Come Home! The Challenge of Mass Production World War II saw major advances in medical technology including the mass production of penicillin. On March 14, 1942, U.S. made-penicillin was used to successfully treat the first patient for septicemia, or blood poisoning. While that one treatment exhausted half of the available supply of penicillin in the entire U.S., the need for better techniques for rapidly producing penicillin on a large scale was necessary to treat soldiers fighting abroad. Scientists working around the clock manufactured 2.3 million doses of penicillin in preparation for the D-Day landings on June 6, 1944. Explore with your students the important role of antibiotics on human history and the collaborative effort to mass produce penicillin. OBJECTIVES: Students will analyze historic images and interpret the meaning of print materials. After reading text, students will think critically about the challenges of mass production and recognize the role of collaboration in scientific undertakings. Students will analyze the speed at which bacteria reproduce and explore exponential growth patterns. By identifying the function of antibiotics on the structure and function of bacterial cells, students will recognize the impact of antibiotics on human health during the 20th century. GRADE LEVEL: 7-12 with enrichment activities for advanced students STANDARDS: NGSS HS-PS1-b, Science is a Way of Knowing – Science knowledge has a history that includes the refinement of, and changes to, theories, ideas, and beliefs over time. -

The Experience of Cancer Illness. Spain and Beyond During The
TESIS DOCTORAL The Experience of Cancer Illness Spain and Beyond During the Second Half of the Nineteenth Century Autora: Fanny Hernández Brotons Directores: Javier Moscoso y Fernando Broncano Tutor: Fernando Broncano DEPARTAMENTO DE HUMANIDADES: FILOSOFÍA, LENGUAJE Y LITERATURA Getafe, septiembre de 2017 PhD THESIS The Experience of Cancer Illness Spain and Beyond During the Second Half of the Nineteenth Century Author: Fanny Hernández Brotons Supervisors: Javier Moscoso and Fernando Broncano Tutor: Fernando Broncano CARLOS III UNIVERSITY FACULTY OF HUMANITIES, COMMUNICATION, AND LIBRARY SCIENCE Department of Humanities: Philosophy, Language, and Literature Getafe (Madrid) – 2017 To my father ACKNOWLEDGEMENTS I began to develop a taste for scientific research over the course of my undergraduate studies in Political Sciences and Administration at Complutense University, Madrid. During the summers of 2009 and 2010, two consecutive scholarships granted by the JAE Intro programme of the Spanish National Research Council (CSIC) expanded the scope of my scholarly interests and reinforced my decision to pursue post-graduate studies. In the autumn of 2011, I enrolled in the MA programme in “Cultural Theory and Critique of Culture” at Carlos III University, Madrid. At the same time, I was granted a four-year PhD scholarship by the Spanish FPI-MICINN programme (with reference BES-2011- 046132), which provided me with institutional and financial means to carry out the present thesis. The research I conducted was successively based at the Institute