Common Newborn Rashes N
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Multiple Asymptomatic Papules on the Back of the Right Side of the Chest Angoori Gnaneshwar Rao
QUIZ Multiple Asymptomatic Papules on the Back of the Right Side of the Chest Angoori Gnaneshwar Rao A 43-year-old male presented with multiple asymptomatic complete blood picture, blood sugar, complete urine examination, papules on the back of the right side of the chest of 1 year blood urea, serum creatinine, liver function tests and serum duration. He was asymptomatic a year back then he developed lipid profile were normal. Fundus was normal. A slit skin smear small papules on the right side of the front of the chest initially for acid fast bacilli was negative. A punch biopsy from the and later on involved the front and back of the chest. No representative lesion subjected to histopathological examination history was suggestive of leprosy and hyperlipidemias. Family revealed a cyst with an intricately folded wall, lined by two to history was negative for similar problem. Examination revealed three layers of flattened squamous epithelium and the absence multiple skin-colored to yellowish papules distributed on the of the granular layer. Lobules of sebaceous glands were found front and back of the chest and shoulder region on the right embedded in cyst lining. The lumen was filled with amorphous side [Figure 1]. Also, there were multiple hyperpigmented eosinophilic material and multiple hair shafts [Figures 2-4]. macules on the right infrascapular region. There was no nerve thickening and no sensory deficit and there were no Question hypopigmented or anesthetic patches. Systemic examination did not reveal any abnormality. Routine investigations including What is your diagnosis? (Original) Multiple skin-colored to yellowish papules on the back of chest Figure 1: Figure 2: (Original) Histopathology of skin showing a cyst with an intricately folded and shoulder region on the right side wall lined by two to three layers of flattened squamous epithelium and the absence of granular layer. -

Pediatric and Adolescent Dermatology
Pediatric and adolescent dermatology Management and referral guidelines ICD-10 guide • Acne: L70.0 acne vulgaris; L70.1 acne conglobata; • Molluscum contagiosum: B08.1 L70.4 infantile acne; L70.5 acne excoriae; L70.8 • Nevi (moles): Start with D22 and rest depends other acne; or L70.9 acne unspecified on site • Alopecia areata: L63 alopecia; L63.0 alopecia • Onychomycosis (nail fungus): B35.1 (capitis) totalis; L63.1 alopecia universalis; L63.8 other alopecia areata; or L63.9 alopecia areata • Psoriasis: L40.0 plaque; L40.1 generalized unspecified pustular psoriasis; L40.3 palmoplantar pustulosis; L40.4 guttate; L40.54 psoriatic juvenile • Atopic dermatitis (eczema): L20.82 flexural; arthropathy; L40.8 other psoriasis; or L40.9 L20.83 infantile; L20.89 other atopic dermatitis; or psoriasis unspecified L20.9 atopic dermatitis unspecified • Scabies: B86 • Hemangioma of infancy: D18 hemangioma and lymphangioma any site; D18.0 hemangioma; • Seborrheic dermatitis: L21.0 capitis; L21.1 infantile; D18.00 hemangioma unspecified site; D18.01 L21.8 other seborrheic dermatitis; or L21.9 hemangioma of skin and subcutaneous tissue; seborrheic dermatitis unspecified D18.02 hemangioma of intracranial structures; • Tinea capitis: B35.0 D18.03 hemangioma of intraabdominal structures; or D18.09 hemangioma of other sites • Tinea versicolor: B36.0 • Hyperhidrosis: R61 generalized hyperhidrosis; • Vitiligo: L80 L74.5 focal hyperhidrosis; L74.51 primary focal • Warts: B07.0 verruca plantaris; B07.8 verruca hyperhidrosis, rest depends on site; L74.52 vulgaris (common warts); B07.9 viral wart secondary focal hyperhidrosis unspecified; or A63.0 anogenital warts • Keratosis pilaris: L85.8 other specified epidermal thickening 1 Acne Treatment basics • Tretinoin 0.025% or 0.05% cream • Education: Medications often take weeks to work AND and the patient’s skin may get “worse” (dry and red) • Clindamycin-benzoyl peroxide 1%-5% gel in the before it gets better. -

Training Available: in 2012, Lorenzo Kunze, M.E
2013 Derma-Lo - offers the 2013 Thermo-Lo - offers the reduction of: sun/age spot, milia, reduction of: sun/age spot, milia, telangiectasia / epidermal spider telangiectasia / epidermal spider veins, cherry hemangiomas, veins, cherry hemangiomas and Thermolysis (AC) and Electrolysis Thermolysis (AC) hair removal. (DC) hair removal. Also: active acne, acne scarring, sebaceous hyperplasia, and skin tags. Training Available: In 2012, Lorenzo Kunze, M.E. Includes: Hydro-Lo - treatment IN DENVER ONCE A MONTH developed Chromos, Inc. - which of fine lines and wrinkles, TRAINING AVAILABLE AT in Greek, can be interpreted as enlarged pore reduction, boosts YOUR LOCATION ASK ABOUT “color” or “light” – in essence, the penetration of product into COST without light we have no color. the skin and tightens loose skin. “Dedicated to Excellence” Also: select your choice of (1 of Continuing to provide a professional & positive attitude in the medical 2) LED’s – both are non invasive and aesthetic field. hand-held light probes: BLUE for CHROMOS, Inc. the treatment of acne or Lorenzo Kunze, M.E. Chromos strives to be a guiding INFRARED to increase collagen [email protected] “light” that assists medical and and elastin, Rosacea, increased www.DermaLo.com aesthetic professionals in finding healing properties, minor muscle www.Thermo-Lo.com and pursuing proper education and moderate joint pain. 888-499-8991 / 303-994-7236 and accurate knowledge. Lorenzo Kunze, M.E. Lorenzo is a true visionary - 40 years in the medical and aesthetic field Medical Electrologist / medical educator 1st non-medical professional to provide electrolysis treatments in an OR Treated over 20,000 patients - last 16 years 1st in the U.S. -

Dermatology DDX Deck, 2Nd Edition 65
63. Herpes simplex (cold sores, fever blisters) PREMALIGNANT AND MALIGNANT NON- 64. Varicella (chicken pox) MELANOMA SKIN TUMORS Dermatology DDX Deck, 2nd Edition 65. Herpes zoster (shingles) 126. Basal cell carcinoma 66. Hand, foot, and mouth disease 127. Actinic keratosis TOPICAL THERAPY 128. Squamous cell carcinoma 1. Basic principles of treatment FUNGAL INFECTIONS 129. Bowen disease 2. Topical corticosteroids 67. Candidiasis (moniliasis) 130. Leukoplakia 68. Candidal balanitis 131. Cutaneous T-cell lymphoma ECZEMA 69. Candidiasis (diaper dermatitis) 132. Paget disease of the breast 3. Acute eczematous inflammation 70. Candidiasis of large skin folds (candidal 133. Extramammary Paget disease 4. Rhus dermatitis (poison ivy, poison oak, intertrigo) 134. Cutaneous metastasis poison sumac) 71. Tinea versicolor 5. Subacute eczematous inflammation 72. Tinea of the nails NEVI AND MALIGNANT MELANOMA 6. Chronic eczematous inflammation 73. Angular cheilitis 135. Nevi, melanocytic nevi, moles 7. Lichen simplex chronicus 74. Cutaneous fungal infections (tinea) 136. Atypical mole syndrome (dysplastic nevus 8. Hand eczema 75. Tinea of the foot syndrome) 9. Asteatotic eczema 76. Tinea of the groin 137. Malignant melanoma, lentigo maligna 10. Chapped, fissured feet 77. Tinea of the body 138. Melanoma mimics 11. Allergic contact dermatitis 78. Tinea of the hand 139. Congenital melanocytic nevi 12. Irritant contact dermatitis 79. Tinea incognito 13. Fingertip eczema 80. Tinea of the scalp VASCULAR TUMORS AND MALFORMATIONS 14. Keratolysis exfoliativa 81. Tinea of the beard 140. Hemangiomas of infancy 15. Nummular eczema 141. Vascular malformations 16. Pompholyx EXANTHEMS AND DRUG REACTIONS 142. Cherry angioma 17. Prurigo nodularis 82. Non-specific viral rash 143. Angiokeratoma 18. Stasis dermatitis 83. -

Isotretinoin Induced Periungal Pyogenic Granuloma Resolution with Combination Therapy Jonathan G
Isotretinoin Induced Periungal Pyogenic Granuloma Resolution with Combination Therapy Jonathan G. Bellew, DO, PGY3; Chad Taylor, DO; Jaldeep Daulat, DO; Vernon T. Mackey, DO Advanced Desert Dermatology & Mohave Centers for Dermatology and Plastic Surgery, Peoria, AZ & Las Vegas, NV Abstract Management & Clinical Course Discussion Conclusion Pyogenic granulomas are vascular hyperplasias presenting At the time of the periungal eruption on the distal fingernails, Excess granulation tissue and pyogenic granulomas have It has been reported that the resolution of excess as red papules, polyps, or nodules on the gingiva, fingers, the patient was undergoing isotretinoin therapy for severe been described in both previous acne scars and periungal granulation tissue secondary to systemic retinoid therapy lips, face and tongue of children and young adults. Most nodulocystic acne with significant scarring. He was in his locations.4 Literature review illustrates rare reports of this occurs on withdrawal of isotretinoin.7 Unfortunately for our commonly they are associated with trauma, but systemic fifth month of isotretinoin therapy with a cumulative dose of adverse event. In addition, the mechanism by which patient, discontinuation of isotretinoin and prevention of retinoids have rarely been implicated as a causative factor 140 mg/kg. He began isotretinoin therapy at a dose of 40 retinoids cause excess granulation tissue of the skin is not secondary infection in areas of excess granulation tissue in their appearance. mg daily (0.52 mg/kg/day) for the first month and his dose well known. According to the available literature, a course was insufficient in resolving these lesions. To date, there is We present a case of eruptive pyogenic granulomas of the later increased to 80 mg daily (1.04 mg/kg/day). -

Rosacea: an Update
REVIEW JONELLE K. MCDONNELL, MD KENNETH J. TOMECKI, MD Department of Dermatology, Cleveland Clinic Department of Dermatology, Cleveland Clinic Rosacea: An update • ABSTRACT | >1 OSACEA is a chronic and recurrent LAM inflammatory skin disease characterized Rosacea is a common inflammatory skin disease affecting by erythema, papules, pustules, telangiectasia, the central face of adults. Its etiology is unknown. Early and occasionally sebaceous hyperplasia, which diagnosis and appropriate treatment, usually with topical or primarily affects the central face. The disease systemic antibiotics or both, minimizes symptoms and helps evolves in stages and affects middle-aged to prevent complications. adults. Early diagnosis and thoughtful manage- ment help to control the disease and to mini- • KEY POINTS mize the patient's discomfort and emotional distress. Historically, rosacea has been a mis- Rosacea has a spectrum of cutaneous clinical findings: understood disorder, often attributed to alco- facial erythema, papules, pustules, telangiectasia, and holism and acne.1 rhinophyma. • INCIDENCE Common triggers are sunlight, stress, exposure to extreme Rosacea is a common and chronic disease that heat or cold, alcohol, hot beverages, and spicy foods. affects approximately 13 million Americans, or about 1 in 20 people. Because rosacea fre- Rosacea can resemble other diseases, including acne, quently affects people of northern European seborrheic dermatitis, systemic lupus erythematosus, and heritage, it is often called the "curse of the sarcoidosis. Celts."2 In contrast, it is rarely seen in dark- skinned individuals.3 In most patients, the Ocular involvement occurs in more than 50% of patients onset occurs between the ages of 30 and 50. with rosacea. The early stages affect women more often than men at a ratio of 3 to 1, but men more often Oral tetracycline and topical metronidazole are the develop disfiguring rhinophyma. -

Acne in Childhood: an Update Wendy Kim, DO; and Anthony J
FEATURE Acne in Childhood: An Update Wendy Kim, DO; and Anthony J. Mancini, MD cne is the most common chron- ic skin disease affecting chil- A dren and adolescents, with an 85% prevalence rate among those aged 12 to 24 years.1 However, recent data suggest a younger age of onset is com- mon and that teenagers only comprise 36.5% of patients with acne.2,3 This ar- ticle provides an overview of acne, its pathophysiology, and contemporary classification; reviews treatment op- tions; and reviews recently published algorithms for treating acne of differing levels of severity. Acne can be classified based on le- sion type (morphology) and the age All images courtesy of Anthony J. Mancini, MD. group affected.4 The contemporary Figure 1. Comedonal acne. This patient has numerous closed comedones (ie, “whiteheads”). classification of acne based on sev- eral recent reviews is addressed below. Acne lesions (see Table 1, page 419) can be divided into noninflammatory lesions (open and closed comedones, see Figure 1) and inflammatory lesions (papules, pustules, and nodules, see Figure 2). The comedone begins with Wendy Kim, DO, is Assistant Professor of In- ternal Medicine and Pediatrics, Division of Der- matology, Loyola University Medical Center, Chicago. Anthony J. Mancini, MD, is Professor of Pediatrics and Dermatology, Northwestern University Feinberg School of Medicine, Ann and Robert H. Lurie Children’s Hospital of Chi- cago. Address correspondence to: Anthony J. Man- Figure 2. Moderate mixed acne. In this patient, a combination of closed comedones, inflammatory pap- ules, and pustules can be seen. cini, MD, Division of Dermatology Box #107, Ann and Robert H. -
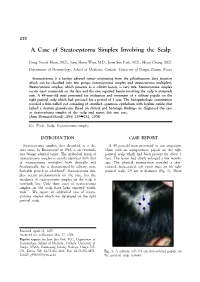
A Case of Steatocystoma Simplex Involving the Scalp
230 A Case of Steatocystoma Simplex Involving the Scalp Dong Nyeok Hyun, M.D., Jong Hoon Won, M.D., Joon Soo Park, M.D., Hyun Chung, M.D. Department of Dermatology, School of Medicine, Catholic University of Daegu, Daegu, Korea Steatocystoma is a benign adnexal tumor originating from the pilosebaceous duct junction which can be classified into two groups (steatocystoma simplex and steatocystoma multiplex). Steatocystoma simplex, which presents as a solitary lesion, is very rare. Steatocystoma simplex occurs most commonly on the face and the case reported herein involving the scalp is extremely rare. A 49-year-old man presented for evaluation and treatment of a solitary papule on the right parietal scalp which had persisted for a period of 1 year. The histopathologic examination revealed a thin-walled cyst consisting of stratified squamous epithelium with hyaline cuticle that lacked a stratum granulosum. Based on clinical and histologic findings, we diagnosed this case as steatocystoma simplex of the scalp and report this rare case. (Ann Dermatol (Seoul) 20(4) 230∼232, 2008) Key Words: Scalp, Steatocystoma simplex INTRODUCTION CASE REPORT Steatocystoma simplex, first described as a dis- A 49-year-old man presented to our outpatient tinct entity by Brownstein1 in 1982, is an extremely clinic with an asymptomatic papule on the right rare benign adnexal tumor. The individual lesion of parietal scalp which had been present for about 1 steatocystoma simplex is usually identical with that year. The lesion had slowly enlarged a few months of steatocystoma multiplex, both clinically and ago. The physical examination revealed a skin- histologically, but is characterized by solitary, non- colored, deep-seated, soft cystic mass on his right heritable growth in adulthood1. -

Fundamentals of Dermatology Describing Rashes and Lesions
Dermatology for the Non-Dermatologist May 30 – June 3, 2018 - 1 - Fundamentals of Dermatology Describing Rashes and Lesions History remains ESSENTIAL to establish diagnosis – duration, treatments, prior history of skin conditions, drug use, systemic illness, etc., etc. Historical characteristics of lesions and rashes are also key elements of the description. Painful vs. painless? Pruritic? Burning sensation? Key descriptive elements – 1- definition and morphology of the lesion, 2- location and the extent of the disease. DEFINITIONS: Atrophy: Thinning of the epidermis and/or dermis causing a shiny appearance or fine wrinkling and/or depression of the skin (common causes: steroids, sudden weight gain, “stretch marks”) Bulla: Circumscribed superficial collection of fluid below or within the epidermis > 5mm (if <5mm vesicle), may be formed by the coalescence of vesicles (blister) Burrow: A linear, “threadlike” elevation of the skin, typically a few millimeters long. (scabies) Comedo: A plugged sebaceous follicle, such as closed (whitehead) & open comedones (blackhead) in acne Crust: Dried residue of serum, blood or pus (scab) Cyst: A circumscribed, usually slightly compressible, round, walled lesion, below the epidermis, may be filled with fluid or semi-solid material (sebaceous cyst, cystic acne) Dermatitis: nonspecific term for inflammation of the skin (many possible causes); may be a specific condition, e.g. atopic dermatitis Eczema: a generic term for acute or chronic inflammatory conditions of the skin. Typically appears erythematous, -

Research Article Mucocutaneous Manifestations of HIV and the Correlation with WHO Clinical Staging in a Tertiary Hospital in Nigeria
Hindawi Publishing Corporation AIDS Research and Treatment Volume 2014, Article ID 360970, 6 pages http://dx.doi.org/10.1155/2014/360970 Research Article Mucocutaneous Manifestations of HIV and the Correlation with WHO Clinical Staging in a Tertiary Hospital in Nigeria Olumayowa Abimbola Oninla Department of Dermatology and Venereology, Faculty of Clinical Sciences, College of Health Sciences, Obafemi Awolowo University, P.O. Box 2545, Ile-Ife 250005, Osun State, Nigeria Correspondence should be addressed to Olumayowa Abimbola Oninla; [email protected] Received 31 July 2014; Revised 15 November 2014; Accepted 25 November 2014; Published 21 December 2014 Academic Editor: P. K. Nicholas Copyright © 2014 Olumayowa Abimbola Oninla. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Skin diseases are indicators of HIV/AIDS which correlates with WHO clinical stages. In resource limited environment where CD4 count is not readily available, they can be used in assessing HIV patients. The study aims to determine the mucocutaneous manifestations in HIV positive patients and their correlation with WHO clinical stages. A prospective cross-sectional study of mucocutaneous conditions was done among 215 newly diagnosed HIV patients from June 2008 to May 2012 at adult ART clinic, Wesley Guild Hospital Unit, OAU Teaching Hospitals Complex, Ilesha, Osun State, Nigeria. There were 156 dermatoses with oral/oesophageal/vaginal candidiasis (41.1%), PPE (24.4%), dermatophytic infections (8.9%), and herpes zoster (3.8%) as the most common dermatoses. The proportions of dermatoses were 4.5%, 21.8%, 53.2%, and 20.5% in stages 1–4, respectively. -

2016 Essentials of Dermatopathology Slide Library Handout Book
2016 Essentials of Dermatopathology Slide Library Handout Book April 8-10, 2016 JW Marriott Houston Downtown Houston, TX USA CASE #01 -- SLIDE #01 Diagnosis: Nodular fasciitis Case Summary: 12 year old male with a rapidly growing temple mass. Present for 4 weeks. Nodular fasciitis is a self-limited pseudosarcomatous proliferation that may cause clinical alarm due to its rapid growth. It is most common in young adults but occurs across a wide age range. This lesion is typically 3-5 cm and composed of bland fibroblasts and myofibroblasts without significant cytologic atypia arranged in a loose storiform pattern with areas of extravasated red blood cells. Mitoses may be numerous, but atypical mitotic figures are absent. Nodular fasciitis is a benign process, and recurrence is very rare (1%). Recent work has shown that the MYH9-USP6 gene fusion is present in approximately 90% of cases, and molecular techniques to show USP6 gene rearrangement may be a helpful ancillary tool in difficult cases or on small biopsy samples. Weiss SW, Goldblum JR. Enzinger and Weiss’s Soft Tissue Tumors, 5th edition. Mosby Elsevier. 2008. Erickson-Johnson MR, Chou MM, Evers BR, Roth CW, Seys AR, Jin L, Ye Y, Lau AW, Wang X, Oliveira AM. Nodular fasciitis: a novel model of transient neoplasia induced by MYH9-USP6 gene fusion. Lab Invest. 2011 Oct;91(10):1427-33. Amary MF, Ye H, Berisha F, Tirabosco R, Presneau N, Flanagan AM. Detection of USP6 gene rearrangement in nodular fasciitis: an important diagnostic tool. Virchows Arch. 2013 Jul;463(1):97-8. CONTRIBUTED BY KAREN FRITCHIE, MD 1 CASE #02 -- SLIDE #02 Diagnosis: Cellular fibrous histiocytoma Case Summary: 12 year old female with wrist mass. -

WHAT YOU NEED to KNOW ABOUT SEYSARA® a Novel Treatment Developed Specifi Cally for Acne
Not an actual patient, results may vary. WHAT YOU NEED TO KNOW ABOUT SEYSARA® A novel treatment developed specifi cally for acne. PLEASE SEE THE ACCOMPANYING PATIENT INFORMATION AND FULL PRESCRIBING INFORMATION. almirall.us INTRODUCING SEYSARA: A NOVEL ORAL ANTIBIOTIC TREATMENT DESIGNED SPECIFICALLY FOR ACNE WHAT IS SEYSARA? WHAT CAUSES ACNE? SEYSARA is a prescription medicine used to treat moderate to Acne appears when a small hole in our skin (pore) clogs with dead severe acne vulgaris in people 9 years and older. SEYSARA should not skin cells. Normally, dead skin cells rise to the surface of the pore, be used for the treatment or prevention of infections. It is not known where they are shed. Excess production of sebum—the oil that keeps if SEYSARA is safe and effective for use for longer than 12 weeks. our skin from drying out—can cause the dead skin cells to stick SEYSARA should not be used in children under 9 years of age, or if you together and get trapped inside the pore. 1 are pregnant or breastfeeding. Sometimes the bacteria that live naturally on our skin, C. acnes, also get inside the pore, where they can multiply quickly. With WHAT IS MODERATE TO SEVERE ACNE? bacteria inside, the pore becomes infl amed (red and swollen). If the acne goes deep into the skin, an acne cyst or nodule appears.4 Acne is a common skin condition involving blockage and/or infl ammation of hair follicles and their associated gland. Depending on the severity, acne is generally categorized as mild, moderate, or severe.