Prevalance of Tuberculosis in District Dir Upper, Pakistan
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Causes of Deforestation and Climatic Changes in Dir Kohistan
CORE Metadata, citation and similar papers at core.ac.uk Provided by International Institute for Science, Technology and Education (IISTE): E-Journals Journal of Pharmacy and Alternative Medicine www.iiste.org ISSN 2222-5668 (Paper) ISSN 2222-4807 (Online) Vol. 3, No. 2, 2014 Research Article Causes of deforestation and climatic changes in Dir Kohistan Muhammad Tariq1*, Muhammad Rashid2, Wajid Rashid3 1Department of Environmental Sciences, Shaheed Benazir Bhutto University, Sheringal Dir Upper, Pakistan 2School of Pharmacy, The University of Faisalabad, Faisalabad, Pakistan 3Department of Environmental Sciences, University of Swat, Pakistan *E-mail of the corresponding author: [email protected] Accepted Date: 22 May 2014 akistan is on 2nd position among those countries, where deforestation rate is very high. The current work is design to highlight the facts, real causes and impacts of deforestation and forest degradation in P “Dir Kohistan” of K.P.K Pakistan, by incorporating the view of local people through a questionnaire. According to this survey about 83% of the local people are dependent on these forests and contribute to deforestation in one of different ways regardless of any rule regulation. The current study shows that the extensive deforestation in the mention area occurs for household needs (cooking, furniture, heating, earning etc). Another growing cause is the cutting of these forests for livestock purposes. Along this the nonscientific grazing is a key point in the deforestation. Unemployment and poverty is another attractive factor in the degradation of these forests. However the role of black marketing and role of stake holders on these forests should not be neglected in deforestation. -

S.No ID.No Inst Name Tehsil Class Beds Locality Status 1 347006 BHU
DISTRICT DIR UPPER Basic Health Units S.No ID.No Inst Name Tehsil Class Beds Locality Status 1 347006 BHU Ganori Dir 1 Ganori Functional 2 347007 BHU Hatan Dara Dir 1 Ganori Functional 3 347009 BHU Kair Dara Dir 1 Bibyaware Functional 4 347010 BHU Darora Dir 1 Darora Functional 5 347011 BHU Battal Dir 1 Palam Functional 6 347013 BHU Jabbar Dir 1 Jabbar Functional 7 347014 BHU Sawni Dir 1 Sawni Functional 8 347016 BHU Ganshal Dir 1 Sawni Functional 9 347017 BHU Qulandi Dir 1 Qulandi Functional 10 347018 BHU Doug Mina Dir 1 Doug Dara Functional 11 347019 BHU Dobando Dir 1 Qulandi Functional 12 347025 BHU Janbatti Barawal 1 Shahi kot Functional 13 347026 BHU Bilachand Barawal 1 Darikand Functional 14 347027 BHU Shahikot Barawal 1 Darikand Functional 15 347028 BHU Bin payen Barawal 1 Shahi kot Functional 16 347031 BHU Bari kot Kalkot 1 Barikot Functional 17 347032 BHU Kalkot Kalkot 1 Kalkot Functional 18 347033 BHU Thall Kalkot 1 Kalkot Functional 19 347034 BHU Gwaldi Kalkot 1 Gwaldi Functional 20 347037 BHU Dislawar Wari 1 Dislawar Functional 21 347038 BHU Bara Dara Wari 1 Kotkay Functional 22 347039 BHU Daskore Bala Wari 1 Wari Functional 23 347040 BHU Pataw Wari 1 Kotkay Functional 24 347041 BHU Karo Dara Wari 1 Akhagram Functional 25 347042 BHU Kakad Wari 1 Wari Functional 26 347043 BHU Jillare Wari 1 Chappar Functional 27 347044 BHU Nasir Abad Wari 1 Chappar Functional 28 347045 BHU Sundal Wari 1 Sundal Functional 29 347046 BHU Nehag Bandi Wari 1 Nihag Bandi Functional 30 347047 BHU Malanga Wari 1 Dislawar Functional Barawal 1 Functional -

1 Annexure - D Names of Village / Neighbourhood Councils Alongwith Seats Detail of Khyber Pakhtunkhwa
1 Annexure - D Names of Village / Neighbourhood Councils alongwith seats detail of Khyber Pakhtunkhwa No. of General Seats in No. of Seats in VC/NC (Categories) Names of S. Names of Tehsil Councils No falling in each Neighbourhood Village N/Hood Total Col Peasants/Work S. No. Village Councils (VC) S. No. Women Youth Minority . district Council Councils (NC) Councils Councils 7+8 ers 1 2 3 4 5 6 7 8 9 10 11 12 13 Abbottabad District Council 1 1 Dalola-I 1 Malik Pura Urban-I 7 7 14 4 2 2 2 2 Dalola-II 2 Malik Pura Urban-II 7 7 14 4 2 2 2 3 Dabban-I 3 Malik Pura Urban-III 5 8 13 4 2 2 2 4 Dabban-II 4 Central Urban-I 7 7 14 4 2 2 2 5 Boi-I 5 Central Urban-II 7 7 14 4 2 2 2 6 Boi-II 6 Central Urban-III 7 7 14 4 2 2 2 7 Sambli Dheri 7 Khola Kehal 7 7 14 4 2 2 2 8 Bandi Pahar 8 Upper Kehal 5 7 12 4 2 2 2 9 Upper Kukmang 9 Kehal 5 8 13 4 2 2 2 10 Central Kukmang 10 Nawa Sher Urban 5 10 15 4 2 2 2 11 Kukmang 11 Nawansher Dhodial 6 10 16 4 2 2 2 12 Pattan Khurd 5 5 2 1 1 1 13 Nambal-I 5 5 2 1 1 1 14 Nambal-II 6 6 2 1 1 1 Abbottabad 15 Majuhan-I 7 7 2 1 1 1 16 Majuhan-II 6 6 2 1 1 1 17 Pattan Kalan-I 5 5 2 1 1 1 18 Pattan Kalan-II 6 6 2 1 1 1 19 Pattan Kalan-III 6 6 2 1 1 1 20 Sialkot 6 6 2 1 1 1 21 Bandi Chamiali 6 6 2 1 1 1 22 Bakot-I 7 7 2 1 1 1 23 Bakot-II 6 6 2 1 1 1 24 Bakot-III 6 6 2 1 1 1 25 Moolia-I 6 6 2 1 1 1 26 Moolia-II 6 6 2 1 1 1 1 Abbottabad No. -

Development Budget Expenditures & Releases 2018-19
DISTRICT Project Description BE 2018-19 Final Budget Releases Expenditure DIR UPPER DP15D00008-Constt of Retaining wall care ofMuhammad Saleem UC Jaber 100,000 100,000 58,500 58,500 DIR UPPER DP15D00009-Retaining Wall at UC Jaber 250,000 250,000 146,250 146,250 DIR UPPER DP15D00010-"Pav of Street at College Colony,Naqib Korona" 200,000 200,000 - - DIR UPPER DP15D00011-"Pav of Street at Sher Afzal Korona,Mirash Patai" 100,000 100,000 - - DIR UPPER DP15D00012-Pav of Street at Kalsho care of Farid 200,000 200,000 - - DIR UPPER DP15D00061-Pav of Street at Qadar Kalay 200,000 200,000 - - DIR UPPER DP15D00065-Constt Widening of Link Road Pitaw BandaUmar Rahman Korona 200,000 200,000 - - DIR UPPER DP15D00236-Construction & Widenng of PCC Road atAlam Zaib Korona Saro Rambial 100,000 100,000 64,000 - DIR UPPER DP15D00259-PCC Road at Gul Nawaz Korona 250,000 250,000 148,952 - DIR UPPER DP15D00267-PCC Road at Mula Muhammad Daskor Bala 300,000 300,000 162,914 - DIR UPPER DP15D00272-Widening and PCC Roads at Inzar Paty 100,000 100,000 100,000 - DIR UPPER DP15D00276-Construction of PCC Road at IslamabadAlwari 100,000 100,000 100,000 - DIR UPPER DP15D00292-Pav of Street at UC Bandai 500,000 500,000 133,405 - DIR UPPER DP15D00310-Pav of street at Jekand 500,000 500,000 361,250 361,250 DIR UPPER DP15D00318-Pukhtagi of Raod at Serai Patrak 500,000 500,000 499,700 499,700 DIR UPPER DP15D00332-"Award for top Ten Students 9th, 10th,11th and 12th" 2,000,000 2,000,000 680,000 680,000 DIR UPPER DP15D00334-Bio Metric System for 07 Schools 500,000 500,000 100,000 -

World Bank Document
The World Bank Khyber Pakhtunkhwa Hydropower and Renewable Energy Development (P163461) Public Disclosure Authorized Public Disclosure Authorized Combined Project Information Documents / Integrated Safeguards Datasheet (PID/ISDS) Appraisal Stage | Date Prepared/Updated: 05-Feb-2020 | Report No: PIDISDSA28695 Public Disclosure Authorized Public Disclosure Authorized Feb 05, 2020 Page 1 of 24 The World Bank Khyber Pakhtunkhwa Hydropower and Renewable Energy Development (P163461) BASIC INFORMATION OPS_TABLE_BASIC_DATA A. Basic Project Data Country Project ID Project Name Parent Project ID (if any) Pakistan P163461 Khyber Pakhtunkhwa Hydropower and Renewable Energy Development Region Estimated Appraisal Date Estimated Board Date Practice Area (Lead) SOUTH ASIA 14-Feb-2020 30-Apr-2020 Energy & Extractives Financing Instrument Borrower(s) Implementing Agency Investment Project Financing The Islamic Republic of Pakhtunkhwa Energy Pakistan Development Organization, Energy and Power Department, Government of Khyber Pakhtunkhwa Proposed Development Objective(s) Increase renewable energy generation and strengthen the capacity of associated institutions in Khyber Pakhtunkhwa. Components Development of Hydropower and Renewable Energy Projects Institutional Strengthening and Energy Sector Development Environment and Social Management Project Implementation Support and Technical Assistance PROJECT FINANCING DATA (US$, Millions) SUMMARY-NewFin1 Total Project Cost 782.00 Total Financing 782.00 of which IBRD/IDA 425.00 Financing Gap 0.00 Feb 05, 2020 Page -
Upper Dir Blockwise
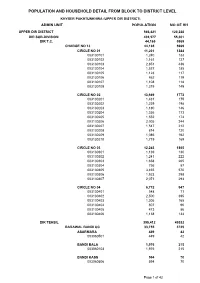
POPULATION AND HOUSEHOLD DETAIL FROM BLOCK TO DISTRICT LEVEL KHYBER PAKHTUNKHWA (UPPER DIR DISTRICT) ADMIN UNIT POPULATION NO OF HH UPPER DIR DISTRICT 946,421 120,228 DIR SUB-DIVISION 439,577 55,301 DIR T.C. 44,165 5969 CHARGE NO 13 44,165 5969 CIRCLE NO 01 11,201 1384 003130101 1,240 133 003130102 1,161 127 003130103 2,851 436 003130104 1,537 185 003130105 1,123 117 003130106 862 119 003130107 1,108 118 003130108 1,319 149 CIRCLE NO 02 13,949 1773 003130201 1,431 175 003130202 1,259 198 003130203 1,180 146 003130204 1,356 173 003130205 1,552 174 003130206 2,005 244 003130207 1,547 212 003130208 814 120 003130209 1,086 162 003130210 1,719 169 CIRCLE NO 03 12,243 1865 003130301 1,139 130 003130302 1,241 222 003130303 1,658 265 003130304 756 87 003130305 3,455 570 003130306 1,923 298 003130307 2,071 293 CIRCLE NO 04 6,772 947 003130401 548 71 003130402 2,500 395 003130403 1,306 165 003130404 807 96 003130405 473 86 003130406 1,138 134 DIR TEHSIL 395,412 49332 BARAWAL BANDI UC 33,755 3725 ASARMARA 449 42 003060501 449 42 BANDI BALA 1,976 215 003060103 1,976 215 BANDI KASS 594 70 003060506 594 70 Page 1 of 42 POPULATION AND HOUSEHOLD DETAIL FROM BLOCK TO DISTRICT LEVEL KHYBER PAKHTUNKHWA (UPPER DIR DISTRICT) ADMIN UNIT POPULATION NO OF HH BANDI PAYEEN 3,302 412 003060101 1,925 197 003060102 1,377 215 CHINDU KOT 1,766 173 003060205 1,766 173 CHIPATRARA 2,470 265 003060408 1,140 120 003060409 1,330 145 DALA KAL KASS 1,438 132 003060302 1,438 132 DIRKHAN 839 127 003060403 839 127 GULO DHERI 153 25 003060106 153 25 JAKARAI 648 74 003060404 648 -

An Ethnobotanical Survey on Fuel Wood and Timber Plant Species of Kaghan Valley, Khyber Pakhtoonkhwa Province, Pakistan
African Journal of Biotechnology Vol. 10(82), pp. 19075-19083, 19 December, 2011 Available online at http://www.academicjournals.org/AJB DOI: 10.5897/AJB10.980 ISSN 1684–5315 © 2011 Academic Journals Full Length Research Paper An Ethnobotanical Survey on Fuel Wood and Timber plant Species of Kaghan Valley, Khyber pakhtoonkhwa Province, Pakistan Gul Jan 1, Mir Ajab Khan 2, Aman khan 1, Farzana Gul Jan 3, Rafiullah Khan 1, Mushtaq Ahmad 2, Atta-Ur-Rehman 1, Muhammad Danish 1, Muhammad Asif 1, Saimdad Khan 1, Muhammad Zafar 2 and Masood Jan 4 1Department of Plant Sciences, Quaid-i-Azam University Islamabad Pakistan. 2Department of Botany, Hazara University, Mansehra, Pakistan. 3Department of Botany, Post Graduate College Abbottabad, Pakistan. Accepted 17 March, 2011 A survey was conducted to explore the fuel wood species and timber producing species of Kaghan valleys, Pakistan. Consumption pattern and impact on the forest resources were also taken into consideration. A questionnaire was used as a survey instrument to obtain desired data. For this study, 10 villages were randomly selected. In each village, 10 persons that were randomly selected were interviewed. Only one person was interviewed from a household. A total of 100 respondents were interviewed. The studies revealed that, 75 plant species belonging to 41 families were utilized as fuel wood and 41 species belonging to 25 families were utilized as timber. Three tree species; Quercus incana , Cedrus deodara and Taxus wallichiana was found endangered. There is a dire need to conserve these species. Key words : Ethnobotany, fuel wood, timber species, Kaghan valleys, Khyber Pakhtoon Khwa Province, Pakistan. -

Contingency Plan Tingency Plan
CONTINGENCY PLAN MONSOON 2012 Provincial Disaster Management Authority Khyber Pakhtunkhwa Monsoon Contingency Plan 2012- Khyber Pakhtunkhwa CONTINGENCY PLAN MONSOON 2012 PROVINCIAL DISASTER MANAGEMENT AUTHORITY KHYBER PAKHTUNKHWA June 2012 2 Monsoon Contingency Plan 2012- Khyber Pakhtunkhwa 3 Monsoon Contingency Plan 2012- Khyber Pakhtunkhwa Prepared by Muhammad Bakhtiar Khan, Deputy Directotr (Relief) under the guidance of Zulfiqar Ali Shah, Director (Relief & Operations), supervised by Shahzad Khan Bangash, Director General, PDMA and Rashid Ahmad, Secretary, Relief, Rehabilitation & Settlement Department, Khyber Pakhtunkhwa. 4 Monsoon Contingency Plan 2012- Khyber Pakhtunkhwa Table of Contents Executive Summary .......................................................................................................................... 7 Chapter-1........................................................................................................................................ 10 Monsoon Contingency Plan 2012.................................................................................................... 10 1.1 An Overview..........................................................................................................................10 1.2 Contingency Plan for Monsoon 2012....................................................................................11 1.3 The Floods - 2010..................................................................................................................12 1.4 Response to Flood 2010........................................................................................................14 -
(Male) Dir Upper Statement Showing the School Wise & Uc Detail of Following Vacant Pst Posts As Stood on 13-11-2020
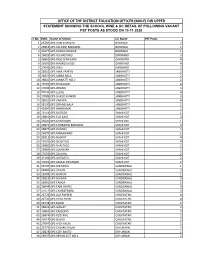
OFFICE OF THE DISTRICT EDUCATION OFFICER (MALE) DIR UPPER STATEMENT SHOWING THE SCHOOL WISE & UC DETAIL OF FOLLOWING VACANT PST POSTS AS STOOD ON 13-11-2020 S.No EMIS Name of School UC Name PST Posts 1 26784 GPS DAKI KHAWAR BARAWAL 2 2 26854 GPS KALPANI BARAWAL BARAWAL 1 3 31977 GPS DANDO KHWAR BARAWAL 1 4 26825 GPS GUJARO KALI DARIKAND 3 5 26862 GPS KASS SHINGARA DARIKAND 4 6 26895 GPS MAMOSI KASS DARIKAND 4 7 27042 GPS GIRO DARIKAND 2 8 26835 GPS JABA PAYEEN JANBHATTI 2 9 26837 GPS JABBA BALA JANBHATTI 2 10 26842 GPS JANBATTI NO.2 JANBHATTI 2 11 26969 GPS SHINAGAR JANBHATTI 4 12 27006 GPS ZIRANO JANBHATTI 3 13 27036 GPS ELGAL JANBHATTI 4 14 27089 GPS SHAGO KHWAR JANBHATTI 3 15 28661 GPS KARAPA JANBHATTI 4 16 38120 GPS ZIRANO BALA JANBHATTI 1 17 40297 GPS MAKHAMAI JANBHATTI 2 18 26754 GPS BATOOR SHAHI KOT 1 19 26810 GPS ELO KASS SHAHI KOT 3 20 26820 GPS GARAWONI SHAHI KOT 1 21 26871 GPS KHORAOW BARAWAL SHAHI KOT 3 22 26877 GPS KOONAI SHAHI KOT 3 23 26899 GPS MARAWARO SHAHI KOT 2 24 26912 GPS NASRAT SHAHI KOT 4 25 26959 GPS SHAHTAIZ SHAHI KOT 4 26 26960 GPS SHALTALO SHAHI KOT 2 27 26989 GPS SWANSAR SHAHI KOT 2 28 27005 GPS ZALIKHA SHAHI KOT 2 29 37194 GPS GATKOTO SHAHI KOT 2 30 39003 GPS KASSAI SWANSAR SHAHI KOT 2 31 26797 GPS DIR KHAN SUNDRAWAL 1 32 26886 GPS LILBAN SUNDRAWAL 3 33 26909 GPS NANGRI SUNDRAWAL 1 34 26919 GPS NOWRA SUNDRAWAL 3 35 26991 GPS TANGA SUNDRAWAL 2 36 26994 GPS TANI SRAPO SUNDRAWAL 4 37 37671 GPS CHUPATRARA SUNDRAWAL 3 38 26726 GPS ALA PAYEEN CHUKYATAN 4 39 26736 GPS AZIM ABAD CHUKYATAN 4 40 26738 GPS BADAI CHUKYATAN -
Addresses of DPW Offices, RHSC-As, Msus, Fwcs & Counters in Khyber
Addresses of Service Delivery Network Including Newly Merged Districts (DPW Offices, RHSC-As, MSUs, FWCs & Counters) (Technical Section) Directorate of Population Welfare Department Government of Khyber Pakhtunkhwa (August, 2019) Plot No 18, Sector E-8, Street No 05, Phase 7, Hayatabad. Phone: 091-9219052, Fax: 091-9219066 1 Content S.No Contents Page No 1. Updated Addresses of District Population Welfare Offices in 3 Khyber Pakhtunkhwa 2. Updated Addresses of Reproductive Health Services Outlets 4 (RHSC-As) in Khyber Pakhtunkhwa 3. Updated Addresses of Mobile Service Units in Khyber 5 Pakhtunkhwa 4. Updated Addresses of Family Welfare Centers in Khyber 7 Pakhtunkhwa 5. Updated Addresses of Counters in Khyber Pakhtunkhwa 28 6. Updated Addresses of District Population Welfare Offices in 29 Merged Districts (Erstwhile FATA) 7. Updated Addresses of Reproductive Health Services Outlets 30 (RHSC-As) in Merged Districts (Erstwhile FATA) 8. Updated Addresses of Mobile Service Units in Merged Districts 31 (Erstwhile FATA) 9. Updated Addresses of Family Welfare Centers in Merged Districts 32 (Erstwhile FATA) 2 Updated Addresses of District Population Welfare Offices in Khyber Pakhtunkhwa S.No Name of DPW Office Complete Address Abbottabad Wajid Iqbal House Azam Town Thanda Chowa PMA Road 1 KakulAbbottabad Phone and fax No.0992-401897 2 Bannu Banglow No.21, Defence Officers Colony Bannu Cantt:. (Ph: No.0928-9270330) 3 Buner Mohallah Tawheed Abad Sawari Buner 4 Battagram Opposite Sub-Jail, Near Lahore Scholars Schools System, Tehsil and District Battagram 5 Chitral Village Goldor, P.O Chitral, Teh& District Lower Chitral 6 Charsadda Opposite Excise & Taxation Office Nowshera Road Charsadda 7 D.I Khan Zakori Town, Draban Road, DIKhan 8 Dir Lower Main GT Road Malik Plaza Khungi Paeen Phone. -
Development Budget Estimates 2018-19
DISTRICT Project Description BE 2018-19 DIR UPPER DP15D00008-Constt of Retaining wall care ofMuhammad Saleem UC Jaber 100,000 DIR UPPER DP15D00009-Retaining Wall at UC Jaber 250,000 DIR UPPER DP15D00010-"Pav of Street at College Colony,Naqib Korona" 200,000 DIR UPPER DP15D00011-"Pav of Street at Sher Afzal Korona,Mirash Patai" 100,000 DIR UPPER DP15D00012-Pav of Street at Kalsho care of Farid 200,000 DIR UPPER DP15D00061-Pav of Street at Qadar Kalay 200,000 DIR UPPER DP15D00065-Constt Widening of Link Road Pitaw BandaUmar Rahman Korona 200,000 DIR UPPER DP15D00236-Construction & Widenng of PCC Road atAlam Zaib Korona Saro Rambial 100,000 DIR UPPER DP15D00259-PCC Road at Gul Nawaz Korona 250,000 DIR UPPER DP15D00267-PCC Road at Mula Muhammad Daskor Bala 300,000 DIR UPPER DP15D00272-Widening and PCC Roads at Inzar Paty 100,000 DIR UPPER DP15D00276-Construction of PCC Road at IslamabadAlwari 100,000 DIR UPPER DP15D00292-Pav of Street at UC Bandai 500,000 DIR UPPER DP15D00310-Pav of street at Jekand 500,000 DIR UPPER DP15D00318-Pukhtagi of Raod at Serai Patrak 500,000 DIR UPPER DP15D00332-"Award for top Ten Students 9th, 10th,11th and 12th" 2,000,000 DIR UPPER DP15D00334-Bio Metric System for 07 Schools 500,000 DIR UPPER DP15D00393-Repair of roof at UPS Thall 400,000 DIR UPPER DP15D00400-DWSS GHS Patrak 1,000,000 DIR UPPER DP15D00418-Constt Widening PCC Road at GPS KalKana 300,000 DIR UPPER DP15D00422-Constt Repair Bridge to GHS Nihag 800,000 DIR UPPER DP15D00439-Constt work at DEO (Male) office Dir 3,000,000 DIR UPPER DP15D00451-Repair work -
Monsoon Contingency Plan 2014
2014 MONSOON CONTINGENCY PLAN This document is the plan of provincial government of Khyber Pakhtunkhwa for combating potential floods disaster of forthcoming season of monsoon 2014 Provincial Disaster Management Authority Government of Khyber Pakhtunkhwa Contents Acronyms .................................................................................................................................... 9 Executive Summary ................................................................................................................... 10 Chapter-1 .................................................................................................................................. 11 Monsoon Contingency Plan 2014 ............................................................................................... 11 1.1 An Overview 11 1.2 Khyber Pakhtunkhwa-General and Flood Profile 12 1.3 Contingency Plan for Monsoon 2014 14 Aim 14 Objectives: 14 Scope 14 Lessons Learnt from PreviousFloods: 14 1.3.1 Inadequate Flood Protection Arrangements: 14 1.3.2 Inadequate Flood Early Warning Arrangements: 15 1.3.3 Encroachments: 15 1.3.4 Lack of Preparedness: 15 1.3.5 Non observance of Early Warningby General Public: 15 1.3.6 Insufficient Water Storage and Regulation Capacity: 16 Chapter-2 .................................................................................................................................. 17 Hazard and Vulnerability Mapping of Disitricts ........................................................................ 17 2.1 Scenarios