Ischial Tuberosity
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Gluteal Region-II
Gluteal Region-II Dr Garima Sehgal Associate Professor King George’s Medical University UP, Lucknow Structures in the Gluteal region • Bones & joints • Ligaments Thickest muscle • Muscles • Vessels • Nerves Thickest nerve • Bursae Learning Objectives By the end of this teaching session Gluteal region –II all the MBBS 1st year students must be able to: • Enumerate the nerves of gluteal region • Write a short note on nerves of gluteal region • Describe the location & relations of sciatic nerve in gluteal region • Enumerate the arteries of gluteal region • Write a short note on arteries of gluteal region • Enumerate the arteries taking part in trochanteric and cruciate anastomosis • Write a short note on trochanteric and cruciate anastomosis • Enumerate the structures passing through greater sciatic foramen • Enumerate the structures passing through lesser sciatic foramen • Enumerate the bursae in relation to gluteus maximus • Enumerate the structures deep to gluteus maximus • Discuss applied anatomy Nerves of Gluteal region (all nerves in gluteal region are branches of sacral plexus) Superior gluteal nerve (L4,L5, S1) Inferior gluteal nerve (L5, S1, S2) FROM DORSAL DIVISIONS Perforating cutaneous nerve (S2,S3) Nerve to quadratus femoris (L4,L5, S1) Nerve to obturator internus (L5, S1, S2) FROM VENTRAL DIVISIONS Pudendal nerve (S2,S3,S4) Sciatic nerve (L4,L5,S1,S2,S3) Posterior cutaneous nerve of thigh FROM BOTH DORSAL &VENTRAL (S1,S2) & (S2,S3) DIVISIONS 1. Superior Gluteal nerve (L4,L5,S1- dorsal division) 1 • Enters through the greater 3 sciatic foramen • Above piriformis 2 • Runs forwards between gluteus medius & gluteus minimus • SUPPLIES: 1. Gluteus medius 2. Gluteus minimus 3. Tensor fasciae latae 2. -

Correlation Analysis of Greater Sciatic Notch Dimensions and His Index in Gender Prediction Based on Hip Bone
International Journal of Multidisciplinary and Current Educational Research (IJMCER) ISSN: 2581-7027 ||Volume|| 3 ||Issue|| 3 ||Pages 175-183 ||2021|| Correlation analysis of greater sciatic notch dimensions and his index in gender prediction based on hip bone 1,Aida Sarač – Hadžihalilović, 2,Emir Beganović, 3,Zurifa Ajanović, 4,Ilvana Hasanbegović, 5,Lejla Dervišević, 6,Senad Šljuka 1,3,4,5Department of Anatomy, Faculty of Medicine, University of Sarajevo, Bosnia and Herzegovina 2 Fachklinik fur Amputationsmedizin. Osterhofen, Bayern, Germany 6 Department of Biology, Faculty of Science, University of Sarajevo, Bosnia and Herzegovina ABSTRACT BACKGROUND/AIM: The greater sciatic notch is important because the gender of the hip bone can be determined on the basis of its appearance and dimensions. Important parameters that are taken into consideration when measuring greater sciatic notch dimensions are: the width and depth of the greater sciatic notch, the width of the upper part of greater sciatic notch. It is important to monitor the ratio of the width and depth of the notch, when assessing the appearance alone. The aim of the study was to determine correlations between the upper part of the greater sciatic notch with the values of it’s width, as well as between depth and width of the upper part of the great sciatic notch. MATERIALS AND METHODS: The study was conducted prospectively on 98 hip bone, of which 56 were single and 42 were within the pelvis. The gender and age of the bones were unknown. All bones belonged to adults in the Bosnian population. The research is based on the osteometric measurements of the width and depth of the greater sciatic notch and width of the upper part of greater sciatic notch, that was used for index calculations of the upper part of the greater sciatic notch. -

Applied Anatomy of the Hip RICARDO A
Applied Anatomy of the Hip RICARDO A. FERNANDEZ, MHS, PT, OCS, CSCS • Northwestern University The hip joint is more than just a ball-and- bones fuse in adults to form the easily recog- socket joint. It supports the weight of the nized “hip” bone. The pelvis, meaning bowl head, arms, and trunk, and it is the primary in Latin, is composed of three structures: the joint that distributes the forces between the innominates, the sacrum, and the coccyx pelvis and lower extremities.1 This joint is (Figure 1). formed from the articu- The ilium has a large flare, or iliac crest, Key PointsPoints lation of the proximal superiorly, with the easily palpable anterior femur with the innomi- superior iliac spine (ASIS) anterior with the The hip joint is structurally composed of nate at the acetabulum. anterior inferior iliac spine (AIIS) just inferior strong ligamentous and capsular compo- The joint is considered to it. Posteriorly, the crest of the ilium ends nents. important because it to form the posterior superior iliac spine can affect the spine and (PSIS). With respect to surface anatomy, Postural alignment of the bones and joints pelvis proximally and the PSIS is often marked as a dimple in the of the hip plays a role in determining the femur and patella skin. Clinicians attempting to identify pelvic functional gait patterns and forces associ- distally. The biomechan- or hip subluxations, leg-length discrepancies, ated with various supporting structures. ics of this joint are often or postural faults during examinations use There is a relationship between the hip misunderstood, and the these landmarks. -

Role of Greater Sciatic Notch in Sexing Human Hip Bones
International Journal of Recent Trends in Science And Technology, ISSN 2277-2812 E-ISSN 2249-8109, Volume 7, Issue 3, 2013 pp 119-123 Role of Greater Sciatic Notch in Sexing Human Hip Bones Rajashree Sheelawant Raut 1*, Prakash B. Hosmani 2, P. R. Kulkarni 3 1Assistant Professor, Department of Anatomy, B. J. Government Medical College, Pune, Maharashtra, INDIA. 2Associate Professor, Department of Anatomy, Dr. V. M. Government Medical College, Solapur, Maharashtra, INDIA. 3 Professor and Head, Department of Anatomy, Government Medical College, Latur, Maharashtra, INDIA. *Corresponding Address: [email protected] Research Article Abstract: Identification of the deceased person from bones is the in archaeological collections that they cannot be used for most critical problem faced by anatomist, forensic science experts sex determination. When pubic material is not preserved, & anthropologists. Skeletal remains have been used for sexing the sex determinations must be made using other less individual as bones of the body are last to perish after death. Hip bone, especially t he greater sciatic notch is valuable in deformed diagnostic features. The greater sciatic notch is especially bones because it is highly sexually dimorphic, is resistant to valuable in such situations because it is highly sexually damage, and thus can often be scored in poorly preserved dimorphic, is resistant to damage, and thus can often be skeletons. In present study one hundred and eighty three adult hip scored in poorly preserved skeletons[3]. Many attempts bones of known sex (125 male and 58 female) are studied for have been made to describe sex differences in the sciatic various parameters of greater sciatic notch. -

Approach to the Anterior Pelvis (Enneking Type III Resection) Bruno Fuchs, MD Phd & Franklin H.Sim, MD Indication 1
Approach to the Anterior Pelvis (Enneking Type III Resection) Bruno Fuchs, MD PhD & Franklin H.Sim, MD Indication 1. Tumors of the pubis 2. part of internal and external hemipelvectomy 3. pelvic fractures Technique 1. Positioning: Type III resections involve the excision of a portion of the symphysis or the whole pubis from the pubic symphysis to the lateral margin of the obturator foramen. The best position for these patients is the lithotomy or supine position. The patient is widely prepared and draped in the lithotomy position with the affected leg free to allow manipulation during the procedure. This allows the hip to be flexed, adducted, and externally rotated to facilitate exposure. 2. Landmarks: One should palpate the ASIS, the symphysis with the pubic tubercles, and the ischial tuberosity. 3. Incision: The incision may be Pfannenstiel like with vertical limbs set laterally along the horizontal incision depending on whether the pubic bones on both sides are resected or not. Alternatively, if only one side is resected, a curved incision following the root of the thigh may be used. This incision begins below the inguinal ligament along the medial border of the femoral triangle and extends across the medial thigh a centimeter distal to the inguinal crease and perineum, to curve distally below the ischium several centimeters (Fig.1). 4. Full thickness flaps are raised so that the anterior inferior pubic ramus is shown in its entire length, from the pubic tubercle to the ischial spine. Laterally, the adductor muscles are visualized, cranially the pectineus muscle and the pubic tubercle with the insertion of the inguinal ligament (Fig.2). -

Surgical Approaches to Fractures of the Acetabulum and Pelvis Joel M
Surgical Approaches to Fractures of the Acetabulum and Pelvis Joel M. Matta, M.D. Sponsored by Mizuho OSI APPROACHES TO THE The table will also stably position the ACETABULUM limb in a number of different positions. No one surgical approach is applicable for all acetabulum fractures. KOCHER-LANGENBECK After examination of the plain films as well as the CT scan the surgeon should APPROACH be knowledgeable of the precise anatomy of the fracture he or she is The Kocher-Langenbeck approach is dealing with. A surgical approach will primarily an approach to the posterior be selected with the expectation that column of the Acetabulum. There is the entire reduction and fixation can excellent exposure of the be performed through the surgical retroacetabular surface from the approach. A precise knowledge of the ischial tuberosity to the inferior portion capabilities of each surgical approach of the iliac wing. The quadrilateral is also necessary. In order to maximize surface is accessible by palpation the capabilities of each surgical through the greater or lesser sciatic approach it is advantageous to operate notch. A less effective though often the patient on the PROfx® Pelvic very useful approach to the anterior Reconstruction Orthopedic Fracture column is available by manipulation Table which can apply traction in a through the greater sciatic notch or by distal and/or lateral direction during intra-articular manipulation through the operation. the Acetabulum (Figure 1). Figure 2. Fractures operated through the Kocher-Langenbeck approach. Figure 3. Positioning of the patient on the PROfx® surgical table for operations through the Kocher-Lagenbeck approach. -

Curvature of the Greater Sciatic Notch in Sexing the Human Pelvis HIDEO TAKAHASHI1*
ANTHROPOLOGICAL SCIENCE Vol. 000, 000–000, 2006 Curvature of the greater sciatic notch in sexing the human pelvis HIDEO TAKAHASHI1* 1Department of Anatomy, Dokkyo University School of Medicine, 880 Kitakobayashi, Mibu-machi, Shimotuga-gun, Tochigi, 321-0293 Japan Received 11 November 2005; accepted 26 January 2006 Abstract The maximum curvature of the greater sciatic notch and two standardized indices were cal- culated for use in the sexing of human hip bones. This was done by means of quadratic regression of the contour points of the greater sciatic notch. The new variables are not directly affected by the osteo- metric landmarks (e.g. ischial spine, tubercle of the piriformis, and posterior inferior iliac spine) which determine the greatest width of the notch. These landmarks are, however, known to be ill-defined on occasion, but nevertheless have been used to derive the conventional depth-to-width index and angles of the sciatic notch. The curvature parameter and its new indices were applied to the sciatic notch of 164 Japanese hip bones of known sex (104 males and 61 females). The accuracy of the new variables in the determination of sex was assessed and compared with that of the conventional indices and angles of the sciatic notch. The best discriminating variable was found to be the posterior angle with an accu- racy of 91%. The new parameters of the present study that represent localized shape of the sharply curved edge of the notch diagnosed sex with an accuracy of 88%. In paleoanthropological or forensic cases, using the maximum curvature of the sciatic notch and its indices may be applicable to sexing the hip bones of specimens with postmortem damage. -

The Pelvis Structure the Pelvic Region Is the Lower Part of the Trunk
The pelvis Structure The pelvic region is the lower part of the trunk, between the abdomen and the thighs. It includes several structures: the bony pelvis (or pelvic skeleton) is the skeleton embedded in the pelvic region of the trunk, subdivided into: the pelvic girdle (i.e., the two hip bones, which are part of the appendicular skeleton), which connects the spine to the lower limbs, and the pelvic region of the spine (i.e., sacrum, and coccyx, which are part of the axial skeleton) the pelvic cavity, is defined as the whole space enclosed by the pelvic skeleton, subdivided into: the greater (or false) pelvis, above the pelvic brim , the lesser (or true) pelvis, below the pelvic brim delimited inferiorly by the pelvic floor(or pelvic diaphragm), which is composed of muscle fibers of the levator ani, the coccygeus muscle, and associated connective tissue which span the area underneath the pelvis. Pelvic floor separate the pelvic cavity above from the perineum below. The pelvic skeleton is formed posteriorly (in the area of the back), by the sacrum and the coccyx and laterally and anteriorly (forward and to the sides), by a pair of hip bones. Each hip bone consists of 3 sections, ilium, ischium, and pubis. During childhood, these sections are separate bones, joined by the triradiate hyaline cartilage. They join each other in a Y-shaped portion of cartilage in the acetabulum. By the end of puberty the three bones will have fused together, and by the age of 25 they will have ossified. The two hip bones join each other at the pubic symphysis. -
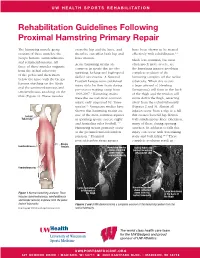
Rehabilitation Guidelines Following Proximal Hamstring Primary Repair
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines Following Proximal Hamstring Primary Repair The hamstring muscle group cross the hip and the knee, and have been shown to be treated consists of three muscles: the therefore can affect both hip and effectively with rehabilitation.1, 8 biceps femoris, semitendinosus knee motion. Much less common, but most and semimembranosus. All Acute hamstring strains are often much more severe, are three of these muscles originate common in sports that involve the hamstring injuries involving from the ischial tuberosity sprinting, kicking and high-speed complete avulsion of the of the pelvis and then insert skilled movements. A National hamstring complex off the ischial below the knee with the biceps Football League team published tuberosity. When this occurs femoris attaching on the fibula injury data for their team during a large amount of bleeding and the semimembranosus and pre-season training camp from (hematoma) will form in the back semitendinosus attaching on the 1998-2007.1 Hamstring strains of the thigh and the tendon will tibia (Figure 1). These muscles were the second most common move down the thigh, retracting injury, only surpassed by “knee away from the ischial tuberosity sprains”.1 Numerous studies have (Figures 2 and 3). Almost all shown that hamstring strains are injuries occur from a slip or a fall Ischial one of the most common injuries that creates forceful hip flexion Tuberosity in sprinting sports, soccer, rugby with simultaneous knee extension, and Australian rules football.1-12 -

Dega Osteotomy (Pelvic Osteotomy)
Dega Osteotomy (Pelvic Osteotomy) Why does my child need this surgery? The hip joint is a ball-and-socket joint that joins the thighbone (femur) to the pelvis. The femoral head, a bony ball at the top of the femur, rotates (turns) inside the pelvic socket (acetabulum). In a child with very tight muscle tone (spasticity), the muscles around the femur can begin pulling the ball out of the socket. For children who walk, the weight of the pelvis may help hold the joint together. A child whose pelvic socket is deep and in good condition may need a femoral derotational osteotomy. This surgery repositions the ball of the femur in the pelvic socket. Sometimes a child’s pelvic socket becomes too shallow to hold the femoral ball. They may need a Dega osteotomy and a femoral derotational osteotomy. Together, the two What happens after surgery? procedures repair the socket, reposition the ball of the femur Your child will probably not be in a cast. A bandage will and make the hip joint stable again. Both procedures will cover the incision. The doctor may use a soft wedge pillow to most likely happen during the same surgery session. They keep the legs spread so the hips can heal in the right position. will probably be combined with a procedure to relax tight Most children are out of the hospital in four to five days. muscles around the hips. The Dega osteotomy is named This includes children who have more than one procedure at for the physician who first wrote about it. -

Sex Determination Using the Distance Between Posterior Inferior Iliac Spine and Ischial Spine in Dry Human Innominate Bone K
Research Article Sex determination using the distance between posterior inferior iliac spine and ischial spine in dry human innominate bone K. Akshaya, Karthik Ganesh Mohanraj* ABSTRACT Aim: This study aims to determine the sex using the distance between the posterior inferior iliac spine and ischial spine. Introduction: Hip bone is taken into account because it is the most sexual dimorphic skeletal component in humans. The greater sciatic notch is very valuable as a result of its proof against damage and is extremely sexually dimorphic. Sexual dimorphism points to the contrasting features between male and female in relation to the size and appearance. Materials and Methods: In the present study, a total of 60 dry human pelvic bones of unknown sex and without any gross abnormality were collected from the Department of Anatomy, Saveetha Dental College, Chennai, for evaluation. With the help of Vernier caliper and ruler, the measurements such as maximum jugular length, maximum jugular breadth, and diameter were measured. The results obtained were analyzed, tabulated, and represented graphically. Results: The distance between the posterior inferior iliac spine and ischial spine is greater in females than in males amped that the depth of the sciatic notch is lesser in females. All these parameters help us distinguish female and males pelvis. Thus, the pelvic bone helps in the determination of sex and is highly sexually dimorphic. Conclusion: The distance between the posterior inferior iliac spine and ischial spine is greater in females than in males amped that the depth of the sciatic notch is lesser in females. All these parameters help us distinguish female and males pelvis. -

Determination of Sex Using Os Coxae in Relation to Ischial Tuberosity – a Morphometric Study M
Research Article Determination of sex using os coxae in relation to ischial tuberosity – A morphometric study M. Shruthi, Karthik Ganesh Mohanraj* ABSTRACT Introduction: Sex determination of an unidentified individual is one of the main objectives when human skeletal remains are found, both in forensic investigation and archaeological studies. The distinctive morphology of the human hip bone and its clear sexual dimorphism build it of interest from anatomical, social science, and rhetorical points of analysis. Determination of biological sex is one of the most important determinations to be made from undocumented human remains which this study is aimed for. Materials and Methods: In the present study, a total of 30 dry human pelvic bones of unknown sex and without any gross abnormality will be collected from the Department of Anatomy, Saveetha Dental College, Chennai, for evaluation. With the help of Vernier caliper and ruler, the measurements such as minimum iliac breadth (MIB), maximum auricular length (MAL), and maximum ischiopubic length (MIPL) are measured. The results obtained were analyzed, tabulated, and represented graphically. Results: The average of MIB in male was found to be 57.61 ± 2.11 mm and in female was found to be 53.45 ± 3.14 mm. The MAL in male was 53.71 ± 1.67 mm and 49.16 ± 2.82 mm in females. The MIPL in male and female was 113.23 ± 4.89 mm and 107.2 ± 7.63 mm, respectively. Conclusion: The chances of attaining high levels of accuracy and reliability regarding sex identification are related to the skeletal components analyzed and the ability of techniques utilized to analyze shape and size differences among the sexes.