Differential Diagnosis for the Lower Extremity
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Gluteal Region-II
Gluteal Region-II Dr Garima Sehgal Associate Professor King George’s Medical University UP, Lucknow Structures in the Gluteal region • Bones & joints • Ligaments Thickest muscle • Muscles • Vessels • Nerves Thickest nerve • Bursae Learning Objectives By the end of this teaching session Gluteal region –II all the MBBS 1st year students must be able to: • Enumerate the nerves of gluteal region • Write a short note on nerves of gluteal region • Describe the location & relations of sciatic nerve in gluteal region • Enumerate the arteries of gluteal region • Write a short note on arteries of gluteal region • Enumerate the arteries taking part in trochanteric and cruciate anastomosis • Write a short note on trochanteric and cruciate anastomosis • Enumerate the structures passing through greater sciatic foramen • Enumerate the structures passing through lesser sciatic foramen • Enumerate the bursae in relation to gluteus maximus • Enumerate the structures deep to gluteus maximus • Discuss applied anatomy Nerves of Gluteal region (all nerves in gluteal region are branches of sacral plexus) Superior gluteal nerve (L4,L5, S1) Inferior gluteal nerve (L5, S1, S2) FROM DORSAL DIVISIONS Perforating cutaneous nerve (S2,S3) Nerve to quadratus femoris (L4,L5, S1) Nerve to obturator internus (L5, S1, S2) FROM VENTRAL DIVISIONS Pudendal nerve (S2,S3,S4) Sciatic nerve (L4,L5,S1,S2,S3) Posterior cutaneous nerve of thigh FROM BOTH DORSAL &VENTRAL (S1,S2) & (S2,S3) DIVISIONS 1. Superior Gluteal nerve (L4,L5,S1- dorsal division) 1 • Enters through the greater 3 sciatic foramen • Above piriformis 2 • Runs forwards between gluteus medius & gluteus minimus • SUPPLIES: 1. Gluteus medius 2. Gluteus minimus 3. Tensor fasciae latae 2. -

Anatomy of the Dog the Present Volume of Anatomy of the Dog Is Based on the 8Th Edition of the Highly Successful German Text-Atlas of Canine Anatomy
Klaus-Dieter Budras · Patrick H. McCarthy · Wolfgang Fricke · Renate Richter Anatomy of the Dog The present volume of Anatomy of the Dog is based on the 8th edition of the highly successful German text-atlas of canine anatomy. Anatomy of the Dog – Fully illustrated with color line diagrams, including unique three-dimensional cross-sectional anatomy, together with radiographs and ultrasound scans – Includes topographic and surface anatomy – Tabular appendices of relational and functional anatomy “A region with which I was very familiar from a surgical standpoint thus became more comprehensible. […] Showing the clinical rele- vance of anatomy in such a way is a powerful tool for stimulating students’ interest. […] In addition to putting anatomical structures into clinical perspective, the text provides a brief but effective guide to dissection.” vet vet The Veterinary Record “The present book-atlas offers the students clear illustrative mate- rial and at the same time an abbreviated textbook for anatomical study and for clinical coordinated study of applied anatomy. Therefore, it provides students with an excellent working know- ledge and understanding of the anatomy of the dog. Beyond this the illustrated text will help in reviewing and in the preparation for examinations. For the practising veterinarians, the book-atlas remains a current quick source of reference for anatomical infor- mation on the dog at the preclinical, diagnostic, clinical and surgical levels.” Acta Veterinaria Hungarica with Aaron Horowitz and Rolf Berg Budras (ed.) Budras ISBN 978-3-89993-018-4 9 783899 9301 84 Fifth, revised edition Klaus-Dieter Budras · Patrick H. McCarthy · Wolfgang Fricke · Renate Richter Anatomy of the Dog The present volume of Anatomy of the Dog is based on the 8th edition of the highly successful German text-atlas of canine anatomy. -

Approach to the Anterior Pelvis (Enneking Type III Resection) Bruno Fuchs, MD Phd & Franklin H.Sim, MD Indication 1
Approach to the Anterior Pelvis (Enneking Type III Resection) Bruno Fuchs, MD PhD & Franklin H.Sim, MD Indication 1. Tumors of the pubis 2. part of internal and external hemipelvectomy 3. pelvic fractures Technique 1. Positioning: Type III resections involve the excision of a portion of the symphysis or the whole pubis from the pubic symphysis to the lateral margin of the obturator foramen. The best position for these patients is the lithotomy or supine position. The patient is widely prepared and draped in the lithotomy position with the affected leg free to allow manipulation during the procedure. This allows the hip to be flexed, adducted, and externally rotated to facilitate exposure. 2. Landmarks: One should palpate the ASIS, the symphysis with the pubic tubercles, and the ischial tuberosity. 3. Incision: The incision may be Pfannenstiel like with vertical limbs set laterally along the horizontal incision depending on whether the pubic bones on both sides are resected or not. Alternatively, if only one side is resected, a curved incision following the root of the thigh may be used. This incision begins below the inguinal ligament along the medial border of the femoral triangle and extends across the medial thigh a centimeter distal to the inguinal crease and perineum, to curve distally below the ischium several centimeters (Fig.1). 4. Full thickness flaps are raised so that the anterior inferior pubic ramus is shown in its entire length, from the pubic tubercle to the ischial spine. Laterally, the adductor muscles are visualized, cranially the pectineus muscle and the pubic tubercle with the insertion of the inguinal ligament (Fig.2). -

Surgical Approaches to Fractures of the Acetabulum and Pelvis Joel M
Surgical Approaches to Fractures of the Acetabulum and Pelvis Joel M. Matta, M.D. Sponsored by Mizuho OSI APPROACHES TO THE The table will also stably position the ACETABULUM limb in a number of different positions. No one surgical approach is applicable for all acetabulum fractures. KOCHER-LANGENBECK After examination of the plain films as well as the CT scan the surgeon should APPROACH be knowledgeable of the precise anatomy of the fracture he or she is The Kocher-Langenbeck approach is dealing with. A surgical approach will primarily an approach to the posterior be selected with the expectation that column of the Acetabulum. There is the entire reduction and fixation can excellent exposure of the be performed through the surgical retroacetabular surface from the approach. A precise knowledge of the ischial tuberosity to the inferior portion capabilities of each surgical approach of the iliac wing. The quadrilateral is also necessary. In order to maximize surface is accessible by palpation the capabilities of each surgical through the greater or lesser sciatic approach it is advantageous to operate notch. A less effective though often the patient on the PROfx® Pelvic very useful approach to the anterior Reconstruction Orthopedic Fracture column is available by manipulation Table which can apply traction in a through the greater sciatic notch or by distal and/or lateral direction during intra-articular manipulation through the operation. the Acetabulum (Figure 1). Figure 2. Fractures operated through the Kocher-Langenbeck approach. Figure 3. Positioning of the patient on the PROfx® surgical table for operations through the Kocher-Lagenbeck approach. -
Rehabilitation Guidelines Following Proximal Hamstring Primary Repair
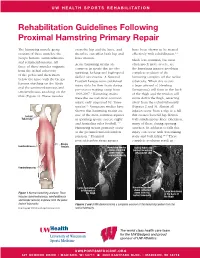
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines Following Proximal Hamstring Primary Repair The hamstring muscle group cross the hip and the knee, and have been shown to be treated consists of three muscles: the therefore can affect both hip and effectively with rehabilitation.1, 8 biceps femoris, semitendinosus knee motion. Much less common, but most and semimembranosus. All Acute hamstring strains are often much more severe, are three of these muscles originate common in sports that involve the hamstring injuries involving from the ischial tuberosity sprinting, kicking and high-speed complete avulsion of the of the pelvis and then insert skilled movements. A National hamstring complex off the ischial below the knee with the biceps Football League team published tuberosity. When this occurs femoris attaching on the fibula injury data for their team during a large amount of bleeding and the semimembranosus and pre-season training camp from (hematoma) will form in the back semitendinosus attaching on the 1998-2007.1 Hamstring strains of the thigh and the tendon will tibia (Figure 1). These muscles were the second most common move down the thigh, retracting injury, only surpassed by “knee away from the ischial tuberosity sprains”.1 Numerous studies have (Figures 2 and 3). Almost all shown that hamstring strains are injuries occur from a slip or a fall Ischial one of the most common injuries that creates forceful hip flexion Tuberosity in sprinting sports, soccer, rugby with simultaneous knee extension, and Australian rules football.1-12 -
A Case of Septic Arthritis of the Shoulder Joint That Developed After Suprascapular Nerve Block
Open Journal of Orthopedics, 2020, 10, 25-32 https://www.scirp.org/journal/ojo ISSN Online: 2164-3016 ISSN Print: 2164-3008 A Case of Septic Arthritis of the Shoulder Joint That Developed after Suprascapular Nerve Block Taihei Go1, Toshiyuki Tsutsui2*, Yasuaki Iida3, Katsunori Fukutake1, Ryoichi Fukano3, Kosei Ishigaki4, Masayuki Sekiguchi1, Hiroshi Takahashi1 1Department of Orthopedics, Toho University, Tokyo, Japan 2Department of Orthopedics, Sagamihara Chuo Hospital, Kanagawa, Japan 3Department of Orthopedics, Omori Red Cross Hospital, Tokyo, Japan 4Department of Orthopedics, Japan Community Health Care Organization Tokyo Kamata Medical Center, Tokyo, Japan How to cite this paper: Go, T., Tsutsui, T., Abstract Iida, Y., Fukutake, K., Fukano, R., Ishigaki, K., Sekiguchi, M. and Takahashi, H. (2020) Septic arthritis of the shoulder is uncommon in the immunocompetent pa- A Case of Septic Arthritis of the Shoulder tient with no previous risk factors for joint infection. We treated an immu- Joint That Developed after Suprascapular nocompetent patient who developed septic arthritis of the shoulder after su- Nerve Block. Open Journal of Orthopedics, 10, 25-32. prascapular nerve block for pain due to rotator cuff tear. An 80-year-old man https://doi.org/10.4236/ojo.2020.102005 with no underlying disease visited a nearby orthopedics clinic with complaint of left shoulder joint pain. Left suprascapular nerve block was performed, but Received: November 30, 2019 Accepted: January 19, 2020 the pain gradually aggravated. On the day after the block, he had a fever of Published: January 22, 2020 39˚C and came to our department. On examination, enlargement and ten- derness were present at the injection site. -

Anatomy and Physiology of the Human Knee Joint
Curriculum Units by Fellows of the Yale-New Haven Teachers Institute 1985 Volume VII: Skeletal Materials- Biomineralization Anatomy and Physiology of the Human Knee Joint Curriculum Unit 85.07.06 by Mara A. Dunleavy Introduction This unit takes an indepth look at a very complex part of the human anatomy, the knee joint. There are numerous structures that are found in this joint, classified as a diarthrodial or synovial joint. Study of this area must include a review of the skeletal and muscular systems in order to see how they interact under normal use. Some knee injuries and the pathologies will be considered. The objectives of this unit are: 1. to introduce the student to the skeletal system with emphasis on the lower extremity; 2. to explain the chemical make-up of bone and the process of ossification; 3. to differentiate between the types of joints in the human body; 4. to introduce the student to the muscular system, with emphasis on those muscle groups of the leg; 5. to describe other structures that are essential for normal movement of this diarthrodial joint, including ligaments, tendons, cartilage and bursa; 6. to explain, demonstrate, and illustrate the coordination of the different systems and each of their specializations; 7. to describe some knee injuries and the pathologies. The outline of the unit is divided into the following five parts: I. Bone, as a tissue Curriculum Unit 85.07.06 1 of 15 a. Histology of bone b. Other tissues related to bones as organs II. Skeleton, bones as organs or structures a. -

Anatomy First Stage
ANATOMY FIRST STAGE Myology Myology: Is the science deal with study of the description of muscles in the body including tendon, apenurosis, and accessory structures like fascia, synovial bursa, and synovial sheath of the tendon. Note 1-The muscle tissue consist of elongated cells called fibers 2-The sytoplasm of muscle cells called sarcoplasm 3-The cell membrane of muscle cells called sarcolemma 4-The sarcoplasm contains numerous myofibrils which contain two types of contractil protein filaments termed actin and myosin Function of the muscles 1-Assist the movement of articulated bones 2-Ability of excitation (contraction and relaxation)of viscera ,blood vessels and iris of eye. 3-Accept the body its architecture and shape . 4-Act as energy stories (glycogen within muscles). 5-Act as protection and fixation of viscera. 6-Responsible of heart movement . Types of muscle: There are 3 types of muscle in the body 1-Skeletal muscle:the skeletal muscle characterized by 1- Striated muscle fiber 2-Generally attached to bone 3-Usually under voluntary control 4-Consist of numbers of muscular bundles which surrounded by fibrous sheath 5- The muscle fiber have multinuclei located peripherally 6- The skeletal muscle fiber cylindrical in shape and extend along entire length of muscle. Note :- Skeletal muscles are usually arranged in pairs so that they oppose each other (they are "antagonists"), one flexing the joint (a flexor muscle) and the other extending it (extensor muscle). ANATOMY FIRST STAGE 2-Cardiac muscle The cardiac muscle like skeletal muscle but differ from it as follow 1- The cardiac muscle fiber is shorter than skeletal muscle fiber 2- They are branched muscle 3- The have certain structures termed intercalated discs ,(the cardiac muscle fiber is restricted between each two intercalated discs. -

Determination of Sex Using Os Coxae in Relation to Ischial Tuberosity – a Morphometric Study M
Research Article Determination of sex using os coxae in relation to ischial tuberosity – A morphometric study M. Shruthi, Karthik Ganesh Mohanraj* ABSTRACT Introduction: Sex determination of an unidentified individual is one of the main objectives when human skeletal remains are found, both in forensic investigation and archaeological studies. The distinctive morphology of the human hip bone and its clear sexual dimorphism build it of interest from anatomical, social science, and rhetorical points of analysis. Determination of biological sex is one of the most important determinations to be made from undocumented human remains which this study is aimed for. Materials and Methods: In the present study, a total of 30 dry human pelvic bones of unknown sex and without any gross abnormality will be collected from the Department of Anatomy, Saveetha Dental College, Chennai, for evaluation. With the help of Vernier caliper and ruler, the measurements such as minimum iliac breadth (MIB), maximum auricular length (MAL), and maximum ischiopubic length (MIPL) are measured. The results obtained were analyzed, tabulated, and represented graphically. Results: The average of MIB in male was found to be 57.61 ± 2.11 mm and in female was found to be 53.45 ± 3.14 mm. The MAL in male was 53.71 ± 1.67 mm and 49.16 ± 2.82 mm in females. The MIPL in male and female was 113.23 ± 4.89 mm and 107.2 ± 7.63 mm, respectively. Conclusion: The chances of attaining high levels of accuracy and reliability regarding sex identification are related to the skeletal components analyzed and the ability of techniques utilized to analyze shape and size differences among the sexes. -

Chapter 14: the Musculoskeletal System
The musculoskeletal system 14 Introduction – Challenges of lameness and gait abnormalities 14.1 Lameness examination and diagnostic techniques 14.2 Hoof anatomy and conformation 14.3 Trimming and shoeing 14.4 Conditions affecting the hoof 14.5 Conditions affecting the bones 14.6 Conditions affecting the joints 14.7 Conditions affecting the tendons and ligaments 14.8 Conditions affecting the muscles 14.9 Conditions affecting the synovial bursae 14.10 Case study – Malignant oedema 14.11 References 14.12 351 Introduction – Challenges of lameness and gait 14.1 abnormalities The musculoskeletal system consists of structures which move the body or maintain its form: muscles, tendons, ligaments, bones and joints. Lameness/gait abnormalities are perhaps the most common presenting sign to working equine veterinarians. Data from the welfare assessment of 4,903 working equids (Pritchard et al. 2005) suggest that over 99% of animals surveyed show gait abnormalities. Lameness can be very frustrating to treat, especially as many cases are chronic and may have many contributing factors (Broster et al. 2009). Long-term rest is often the most effective treatment but this is usually impractical for the owners of working equids. Golden Rule 1 Basic knowledge of anatomy is essential for a confident diagnosis. Golden Rule 2 Think holistically: ‘management’ rather than ‘treatment’. Golden Rule 3 The direct cause may be difficult to identify. 1. Think about which structures are under the skin in the affected area. 2. Think about what could be happening to those structures and why: Acute or chronic? Bone, joint, tendon, ligament or muscle? Infected or sterile? Single or multiple limbs? 3. -

Clinical Manifestations of Synovial Cysts
THE VESTERN Jourx.4 of Medicine Refer to: Burt TB, MacCarter DK, Gelman MI, et al: Clinical manifestations of synovial cysts. West J Med 133:99-104, Aug 1980 Clinical Manifestations of Synovial Cysts TODD B. BURT, MD; DARYL K. MacCARTER, MD; MARTIN 1. GELMAN, MD, and CECIL 0. SAMUELSON, MD, Salt Lake City Although synovial cysts are most commonly associated with rhaumatoid arthritis and osteoarthritis, they may occur in many other conditions. The clinical manifestations of these cysts are numerous and may result from pressure, dissection or acute rupture. Vascular phenomena occur when pop- liteal cysts compress vessels, and result in venous stasis with subsequent lower extremity edema or thrombophlebitis. Rarely, popliteal cysts may cause arterial compromise with intermittent claudication. Neurological sequelae in- clude pain, paresthesia, sensory loss, and muscle weakness or atrophy. When synovial cysts occur as mass lesions they may mimic popliteal aneurysms or hematomas, adenopathy, tumors or even inguinal hernias. Cutaneous joint fistulas, septic arthritis or osteomyelitis, and spinal cord and bladder compres- sion are examples of other infrequent complications. Awareness of the heter- ogeneous manifestations of synovial cysts may enable clinicians to avoid unnecessary diagnostic studies and delay in appropriate management. Ar- thrography remains the definitive diagnostic procedure of choice, although ultrasound testing may be useful. SYNOVIAL CYSTS are fluid-filled spaces lined by in 1877, resulting in the common eponym Baker synovial membrane and arise from diarthrodial cysts, for popliteal cysts.2 Subsequently, synovial joints, bursae and tendon sheaths. The first pub- cysts have been described in numerous locations lished report of a synovial cyst was made by although the knees, shoulders and wrists remain Adams, an Irish surgeon, in 1840.1 He described the most frequently involved areas. -

An Up-To-Date Overview of Evaluation and Management
Translational Research in Anatomy 11 (2018) 5–9 Contents lists available at ScienceDirect Translational Research in Anatomy journal homepage: www.elsevier.com/locate/tria Ureterosciatic hernia: An up-to-date overview of evaluation and T management ∗ Jason Gandhia,b,c, Min Yea Leea, Gunjan Joshid, Noel L. Smithe, Sardar Ali Khana,f, a Department of Physiology and Biophysics, Stony Brook University School of Medicine, Stony Brook, NY, USA b Medical Student Research Institute, St. George's University School of Medicine, West Indies, Grenada c Department of Anatomical Sciences, St. George's University School of Medicine, West Indies, Grenada d Department of Internal Medicine, Stony Brook Southampton Hospital, Southampton, NY, USA e Foley Plaza Medical, New York, NY, USA f Department of Urology, Stony Brook University School of Medicine, Stony Brook, NY, USA ARTICLE INFO ABSTRACT Keywords: Ureterosciatic hernia, defined as a suprapiriform or infrapiriform herniation of the pelvic ureter, is the sliding of Ureter the ureters into the pelvic fossa, fovea, or greater or lesser sciatic foramen. This type of hernia is the rarest form Sciatic hernia of pelvic sciatic hernias. It may cause a wide range of cryptic clinical symptoms of pain, obstructive uropathy, Ureteral obstruction sepsis, or renal failure. This condition has been described in terms of involvement in inguinal, femoral, sciatic, Sepsis obturator, and thoracic regions. A high index of clinical suspicion is essential for diagnosis because the hernia Hydronephrosis develops in the pelvic cavity and becomes overlayed by the large gluteal muscle. Since ureterosciatic hernias Renal failure have not been adequately reviewed in the literature due to the limited number of case reports, we aim to aid the clinician's knowledge by discussing the relevant anatomy, classification, clinical symptoms, optional radiology, optional diagnostic instrumentation, and management.