Surgical Approaches to Fractures of the Acetabulum and Pelvis Joel M
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Minimally Invasive Surgical Treatment Using 'Iliac Pillar' Screw for Isolated
European Journal of Trauma and Emergency Surgery (2019) 45:213–219 https://doi.org/10.1007/s00068-018-1046-0 ORIGINAL ARTICLE Minimally invasive surgical treatment using ‘iliac pillar’ screw for isolated iliac wing fractures in geriatric patients: a new challenge Weon‑Yoo Kim1,2 · Se‑Won Lee1,3 · Ki‑Won Kim1,3 · Soon‑Yong Kwon1,4 · Yeon‑Ho Choi5 Received: 1 May 2018 / Accepted: 29 October 2018 / Published online: 1 November 2018 © Springer-Verlag GmbH Germany, part of Springer Nature 2018 Abstract Purpose There have been no prior case series of isolated iliac wing fracture (IIWF) due to low-energy trauma in geriatric patients in the literature. The aim of this study was to describe the characteristics of IIWF in geriatric patients, and to pre- sent a case series of IIWF in geriatric patients who underwent our minimally invasive screw fixation technique named ‘iliac pillar screw fixation’. Materials and methods We retrospectively reviewed six geriatric patients over 65 years old who had isolated iliac wing fracture treated with minimally invasive screw fixation technique between January 2006 and April 2016. Results Six geriatric patients received iliac pillar screw fixation for acute IIWFs. The incidence of IIWFs was approximately 3.5% of geriatric patients with any pelvic bone fractures. The main fracture line exists in common; it extends from a point between the anterosuperior iliac spine and the anteroinferior iliac spine to a point located at the dorsal 1/3 of the iliac crest whether fracture was comminuted or not. Regarding the Koval walking ability, patients who underwent iliac pillar screw fixation technique tended to regain their pre-injury walking including one patient in a previously bedridden state. -

Pelvic Anatomyanatomy
PelvicPelvic AnatomyAnatomy RobertRobert E.E. Gutman,Gutman, MDMD ObjectivesObjectives UnderstandUnderstand pelvicpelvic anatomyanatomy Organs and structures of the female pelvis Vascular Supply Neurologic supply Pelvic and retroperitoneal contents and spaces Bony structures Connective tissue (fascia, ligaments) Pelvic floor and abdominal musculature DescribeDescribe functionalfunctional anatomyanatomy andand relevantrelevant pathophysiologypathophysiology Pelvic support Urinary continence Fecal continence AbdominalAbdominal WallWall RectusRectus FasciaFascia LayersLayers WhatWhat areare thethe layerslayers ofof thethe rectusrectus fasciafascia AboveAbove thethe arcuatearcuate line?line? BelowBelow thethe arcuatearcuate line?line? MedianMedial umbilicalumbilical fold Lateralligaments umbilical & folds folds BonyBony AnatomyAnatomy andand LigamentsLigaments BonyBony PelvisPelvis TheThe bonybony pelvispelvis isis comprisedcomprised ofof 22 innominateinnominate bones,bones, thethe sacrum,sacrum, andand thethe coccyx.coccyx. WhatWhat 33 piecespieces fusefuse toto makemake thethe InnominateInnominate bone?bone? PubisPubis IschiumIschium IliumIlium ClinicalClinical PelvimetryPelvimetry WhichWhich measurementsmeasurements thatthat cancan bebe mademade onon exam?exam? InletInlet DiagonalDiagonal ConjugateConjugate MidplaneMidplane InterspinousInterspinous diameterdiameter OutletOutlet TransverseTransverse diameterdiameter ((intertuberousintertuberous)) andand APAP diameterdiameter ((symphysissymphysis toto coccyx)coccyx) -

Gluteal Region-II
Gluteal Region-II Dr Garima Sehgal Associate Professor King George’s Medical University UP, Lucknow Structures in the Gluteal region • Bones & joints • Ligaments Thickest muscle • Muscles • Vessels • Nerves Thickest nerve • Bursae Learning Objectives By the end of this teaching session Gluteal region –II all the MBBS 1st year students must be able to: • Enumerate the nerves of gluteal region • Write a short note on nerves of gluteal region • Describe the location & relations of sciatic nerve in gluteal region • Enumerate the arteries of gluteal region • Write a short note on arteries of gluteal region • Enumerate the arteries taking part in trochanteric and cruciate anastomosis • Write a short note on trochanteric and cruciate anastomosis • Enumerate the structures passing through greater sciatic foramen • Enumerate the structures passing through lesser sciatic foramen • Enumerate the bursae in relation to gluteus maximus • Enumerate the structures deep to gluteus maximus • Discuss applied anatomy Nerves of Gluteal region (all nerves in gluteal region are branches of sacral plexus) Superior gluteal nerve (L4,L5, S1) Inferior gluteal nerve (L5, S1, S2) FROM DORSAL DIVISIONS Perforating cutaneous nerve (S2,S3) Nerve to quadratus femoris (L4,L5, S1) Nerve to obturator internus (L5, S1, S2) FROM VENTRAL DIVISIONS Pudendal nerve (S2,S3,S4) Sciatic nerve (L4,L5,S1,S2,S3) Posterior cutaneous nerve of thigh FROM BOTH DORSAL &VENTRAL (S1,S2) & (S2,S3) DIVISIONS 1. Superior Gluteal nerve (L4,L5,S1- dorsal division) 1 • Enters through the greater 3 sciatic foramen • Above piriformis 2 • Runs forwards between gluteus medius & gluteus minimus • SUPPLIES: 1. Gluteus medius 2. Gluteus minimus 3. Tensor fasciae latae 2. -

Femur Pelvis HIP JOINT Femoral Head in Acetabulum Acetabular
Anatomy of the Hip Joint Overview The hip joint is one of the largest weight-bearing HIP JOINT joints in the body. This ball-and-socket joint allows the leg to move and rotate while keeping the body Femoral head in stable and balanced. Let's take a closer look at the acetabulum main parts of the hip joint's anatomy. Pelvis Bones Two bones meet at the hip joint, the femur and the pelvis. The femur, commonly called the "thighbone," is the longest and heaviest bone of the body. At the top of the femur, positioned on the femoral neck, is the femoral head. This is the "ball" of the hip joint. The other part of the joint – the Femur "socket" – is found in the pelvis. The pelvis is a bone made of three sections: the ilium, the ischium and the pubis. The socket is located where these three sections fuse. The proper name of the socket is the "acetabulum." The head of the femur fits tightly into this cup-shaped cavity. Articular Cartilage The femoral head and the acetabulum are covered Acetabular with a layer of articular cartilage. This tough, smooth tissue protects the bones. It allows them to labrum glide smoothly against each other as the ball moves in the socket. Soft Tissues Several soft tissue structures work together to hold the femoral head securely in place. The acetabulum is surrounded by a ring of cartilage called the "acetabular labrum." This deepens the socket and helps keep the ball from slipping out of alignment. It also acts as a shock absorber. -

Lab #23 Anal Triangle
THE BONY PELVIS AND ANAL TRIANGLE (Grant's Dissector [16th Ed.] pp. 141-145) TODAY’S GOALS: 1. Identify relevant bony features/landmarks on skeletal materials or pelvic models. 2. Identify the sacrotuberous and sacrospinous ligaments. 3. Describe the organization and divisions of the perineum into two triangles: anal triangle and urogenital triangle 4. Dissect the ischiorectal (ischioanal) fossa and define its boundaries. 5. Identify the inferior rectal nerve and artery, the pudendal (Alcock’s) canal and the external anal sphincter. DISSECTION NOTES: The perineum is the diamond-shaped area between the upper thighs and below the inferior pelvic aperture and pelvic diaphragm. It is divided anatomically into 2 triangles: the anal triangle and the urogenital (UG) triangle (Dissector p. 142, Fig. 5.2). The anal triangle is bounded by the tip of the coccyx, sacrotuberous ligaments, and a line connecting the right and left ischial tuberosities. It contains the anal canal, which pierced the levator ani muscle portion of the pelvic diaphragm. The urogenital triangle is bounded by the ischiopubic rami to the inferior surface of the pubic symphysis and a line connecting the right and left ischial tuberosities. This triangular space contains the urogenital (UG) diaphragm that transmits the urethra (in male) and urethra and vagina (in female). A. Anal Triangle Turn the cadaver into the prone position. Make skin incisions as on page 144, Fig. 5.4 of the Dissector. Reflect skin and superficial fascia of the gluteal region in one flap to expose the large gluteus maximus muscle. This muscle has proximal attachments to the posteromedial surface of the ilium, posterior surfaces of the sacrum and coccyx, and the sacrotuberous ligament. -

Approach to the Anterior Pelvis (Enneking Type III Resection) Bruno Fuchs, MD Phd & Franklin H.Sim, MD Indication 1
Approach to the Anterior Pelvis (Enneking Type III Resection) Bruno Fuchs, MD PhD & Franklin H.Sim, MD Indication 1. Tumors of the pubis 2. part of internal and external hemipelvectomy 3. pelvic fractures Technique 1. Positioning: Type III resections involve the excision of a portion of the symphysis or the whole pubis from the pubic symphysis to the lateral margin of the obturator foramen. The best position for these patients is the lithotomy or supine position. The patient is widely prepared and draped in the lithotomy position with the affected leg free to allow manipulation during the procedure. This allows the hip to be flexed, adducted, and externally rotated to facilitate exposure. 2. Landmarks: One should palpate the ASIS, the symphysis with the pubic tubercles, and the ischial tuberosity. 3. Incision: The incision may be Pfannenstiel like with vertical limbs set laterally along the horizontal incision depending on whether the pubic bones on both sides are resected or not. Alternatively, if only one side is resected, a curved incision following the root of the thigh may be used. This incision begins below the inguinal ligament along the medial border of the femoral triangle and extends across the medial thigh a centimeter distal to the inguinal crease and perineum, to curve distally below the ischium several centimeters (Fig.1). 4. Full thickness flaps are raised so that the anterior inferior pubic ramus is shown in its entire length, from the pubic tubercle to the ischial spine. Laterally, the adductor muscles are visualized, cranially the pectineus muscle and the pubic tubercle with the insertion of the inguinal ligament (Fig.2). -

Iliac Crest Herniation Secondary to Autogenous Bone Grafting Found on Osteopathic Examination Christine J
CASE REPORT Iliac Crest Herniation Secondary to Autogenous Bone Grafting Found on Osteopathic Examination Christine J. Ou, DO William C. Sternfeld, MD Julie M. Stausmire, MSN, ACNS-BC From Mercy St. Vincent Surgical repair of difficult or nonunion fractures is frequently performed with Medical Center in autogenous bone grafts, most commonly from the iliac crest. Complications Toledo, Ohio. Dr Ou is a fifth-year resident from this procedure may include vessel injury, nerve injury, pelvic instability, in the Osteopathic bowel herniation, and ileus. The authors report a case of iliac crest herniation General Surgery in a patient presenting with a small-bowel obstruction 2 years after anterior iliac Residency Program crest graft harvest for an open reduction and internal fixation repair of a right Financial Disclosures: None reported. humeral shaft fracture. An emergency operation revealed that the right colon had herniated through an opening in the right iliac crest. The appendix had Support: None reported. adhered to new osseous bone formed postoperatively, requiring an appendec- Address correspondence to Julie M. Stausmire MSN, tomy. The hernia defect was successfully repaired with polypropylene mesh. ACNS-BC, A high index of suspicion for graft site herniation is needed for patients with a Mercy St. Vincent history of iliac crest bone grafting who present with symptoms of abdominal Medical Center, 2213 Cherry St, pain, flank or hip pain, ileus, or small-bowel obstruction. Toledo, OH 43608-2801. J Am Osteopath Assoc. 2015;115(8):518-521 doi:10.7556/jaoa.2015.107 E-mail: [email protected] Submitted October 29, 2014; final revision utogenous bone grafting is a common procedure for orthopedic surgeons. -

The Association of Iliac and Sacral Insufficiency Fractures and Implications for Treatment: the Role of Bone Scans in Three Different Cases
Open Access Case Report DOI: 10.7759/cureus.3861 The Association of Iliac and Sacral Insufficiency Fractures and Implications for Treatment: The Role of Bone Scans in Three Different Cases Sandeep Kola 1 , Michelle Granville 2 , Robert E. Jacobson 2 1. Physical Medicine and Rehabilitation, Larkin Community Hospital, Miami, USA 2. Neurological Surgery, University of Miami Hospital, Miami, USA Corresponding author: Michelle Granville, [email protected] Abstract Iliac wing fractures are under-diagnosed fractures often associated with sacral insufficiency fractures in osteoporotic patients. They are rarely seen alone. Insufficiency fractures of the iliac bone can often be missed on computerized tomography (CT) and magnetic resonance imaging (MRI) yet identified on radioisotope bone scans. Symptomatic iliac fractures present with more lateralized pain in the hip and groin compared to patients with only sacral insufficiency fractures. Since the acetabulum is the key weight- bearing articulation between the sacrum and pelvis and the femoral head and leg, worsening of iliac stress fractures can have major effects on weight bearing and should be a consideration in patients with persistent pain in this area. The anatomy of the ilium and relationship to other pelvic insufficiency fractures is reviewed as well as treatment options. Typical cases are presented where the iliac fractures were found on bone scan either in addition to the more common sacral fracture or due to the persistence of symptoms of hip and thigh pain. Categories: Physical Medicine & Rehabilitation, Radiology, Neurosurgery Keywords: insufficency fractures, ilium, sacral fractures, sacroplasty, acetabulum rim fractures, osteoporosis Introduction The iliac bone composes part of the pelvic ring and can be affected by both traumatic and osteoporotic sacral and pelvic fractures [1-2]. -

The Pelvis Structure the Pelvic Region Is the Lower Part of the Trunk
The pelvis Structure The pelvic region is the lower part of the trunk, between the abdomen and the thighs. It includes several structures: the bony pelvis (or pelvic skeleton) is the skeleton embedded in the pelvic region of the trunk, subdivided into: the pelvic girdle (i.e., the two hip bones, which are part of the appendicular skeleton), which connects the spine to the lower limbs, and the pelvic region of the spine (i.e., sacrum, and coccyx, which are part of the axial skeleton) the pelvic cavity, is defined as the whole space enclosed by the pelvic skeleton, subdivided into: the greater (or false) pelvis, above the pelvic brim , the lesser (or true) pelvis, below the pelvic brim delimited inferiorly by the pelvic floor(or pelvic diaphragm), which is composed of muscle fibers of the levator ani, the coccygeus muscle, and associated connective tissue which span the area underneath the pelvis. Pelvic floor separate the pelvic cavity above from the perineum below. The pelvic skeleton is formed posteriorly (in the area of the back), by the sacrum and the coccyx and laterally and anteriorly (forward and to the sides), by a pair of hip bones. Each hip bone consists of 3 sections, ilium, ischium, and pubis. During childhood, these sections are separate bones, joined by the triradiate hyaline cartilage. They join each other in a Y-shaped portion of cartilage in the acetabulum. By the end of puberty the three bones will have fused together, and by the age of 25 they will have ossified. The two hip bones join each other at the pubic symphysis. -
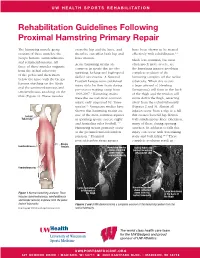
Rehabilitation Guidelines Following Proximal Hamstring Primary Repair
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines Following Proximal Hamstring Primary Repair The hamstring muscle group cross the hip and the knee, and have been shown to be treated consists of three muscles: the therefore can affect both hip and effectively with rehabilitation.1, 8 biceps femoris, semitendinosus knee motion. Much less common, but most and semimembranosus. All Acute hamstring strains are often much more severe, are three of these muscles originate common in sports that involve the hamstring injuries involving from the ischial tuberosity sprinting, kicking and high-speed complete avulsion of the of the pelvis and then insert skilled movements. A National hamstring complex off the ischial below the knee with the biceps Football League team published tuberosity. When this occurs femoris attaching on the fibula injury data for their team during a large amount of bleeding and the semimembranosus and pre-season training camp from (hematoma) will form in the back semitendinosus attaching on the 1998-2007.1 Hamstring strains of the thigh and the tendon will tibia (Figure 1). These muscles were the second most common move down the thigh, retracting injury, only surpassed by “knee away from the ischial tuberosity sprains”.1 Numerous studies have (Figures 2 and 3). Almost all shown that hamstring strains are injuries occur from a slip or a fall Ischial one of the most common injuries that creates forceful hip flexion Tuberosity in sprinting sports, soccer, rugby with simultaneous knee extension, and Australian rules football.1-12 -

Investigation of Front Seat Occupants' Acetabulum Injury in Front Impact
Investigation of front seat occupants' acetabulum injury in front impact Shinichi Hayashi Ryuuji Ootani Tsuyoshi Matsunaga Taisuke Watanabe Chinmoy Pal Shigeru Hirayama Nissan Motor Co., Ltd. Japan Paper Number 17-0207 ABSTRACT Among the proposed amendments to the US-NCAP announced on Dec. 2015, a new acetabulum injury evaluation along with the next-generation THOR dummy has been included [1]. In relation to this topic, numerous research tests and studies are already being conducted by NHTSA. However, 29% of those tests showed that acetabulum injury has occurred due to tensile load rather than a compressive load from the femur. Therefore, in this research, we investigated whether similar injury mechanism actually occurred in real world accidents using NASS-CDS (CY2000-10) data. It is observed that 95% of acetabulum injuries in real world accidents were injuries accompanied by fractures, and 82% of these injuries were related to interaction with the instrument panel. This suggests that most of the acetabulum injuries occur by a compressive load and they are far less likely to occur with tensile load. In addition, by analyzing the mechanism of injury occurrence of the research tests, there are the two influential factors for the difference between the crash test results and real world accidents. They are i) the difference between the THOR dummy and the human body around the hip joint and ii) the problem of acetabulum injury criterion. In the future, further research is necessary in order to propose a more appropriate injury risk evaluation. INTRODUCTION Related to the injuries at and around the hip joint of vehicle occupants during a frontal crash, a number of research reports were already published. -

Axial CT Cystogram
81 y/o male with abdominal pain s/p cystoscopy Edward Gillis, DO David Karimeddini, MD Axial CT Cystogram Axial CT Cystogram Axial CT Cystogram Coronal CT Cystogram ? Intra- and extraperitoneal bladder rupture Axial CT Cystogram: At the mid pelvis, contrast is seen extravasating into the left paracolic gutter, indicating an intraperitoneal component. Axial CT Cystogram: Lower down, perivesical contrast is seen. Foley catheter is present within the bladder. Axial CT Cystogram: Contrast extravasation localized around the right ureterovesical junction. Coronal CT Cystogram: Perivesical contrast around the dome of the bladder (blue arrow). Contrast is also demonstrated in the left paracolic gutter, indicating an intraperitoneal component (green arrow). Sagittal CT Cystogram: Defect in the bladder dome (yellow arrow) with perivesical contrast. Bladder Rupture Imaging Features • Intraperitoneal rupture – Contrast extravasates into the paracolic gutters and outlines loops of bowel. – Layering of contrast in dependent areas (Pouch of Douglas, Morrison’s Pouch) – Look for bladder dome defect • Extraperitoneal Rupture – Extravasation into extraperitoneal spaces, most commonly the retropubic space of Retzius – May see contrast extravasation into the anterior abdominal wall, thigh, and scrotum Bladder Rupture General Features • Extraperitoneal – 62% of all bladder ruptures – Usually secondary to pelvic fracture; fragment lacerates the base of the bladder. – Treatment is usually medical management with Abx and catheterization • Intraperitoneal – 25% of bladder ruptures – Trauma to abdomen with full bladder – May mimic acute renal failure – Treatment requires surgery to repair bladder dome • Combined – 12% of ruptures – Findings of both intraperitoneal and extraperitoneal ruptures References 1. Brant, W. E., & Helms, C. A. (2012). Fundamentals of diagnostic radiology. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins 2.