Chapter 14 *Lecture Powerpoint
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

NS201C Anatomy 1: Sensory and Motor Systems
NS201C Anatomy 1: Sensory and Motor Systems 25th January 2017 Peter Ohara Department of Anatomy [email protected] The Subdivisions and Components of the Central Nervous System Axes and Anatomical Planes of Sections of the Human and Rat Brain Development of the neural tube 1 Dorsal and ventral cell groups Dermatomes and myotomes Neural crest derivatives: 1 Neural crest derivatives: 2 Development of the neural tube 2 Timing of development of the neural tube and its derivatives Timing of development of the neural tube and its derivatives Gestational Crown-rump Structure(s) age (Weeks) length (mm) 3 3 cerebral vesicles 4 4 Optic cup, otic placode (future internal ear) 5 6 cerebral vesicles, cranial nerve nuclei 6 12 Cranial and cervical flexures, rhombic lips (future cerebellum) 7 17 Thalamus, hypothalamus, internal capsule, basal ganglia Hippocampus, fornix, olfactory bulb, longitudinal fissure that 8 30 separates the hemispheres 10 53 First callosal fibers cross the midline, early cerebellum 12 80 Major expansion of the cerebral cortex 16 134 Olfactory connections established 20 185 Gyral and sulcul patterns of the cerebral cortex established Clinical case A 68 year old woman with hypertension and diabetes develops abrupt onset numbness and tingling on the right half of the face and head and the entire right hemitrunk, right arm and right leg. She does not experience any weakness or incoordination. Physical Examination: Vitals: T 37.0° C; BP 168/87; P 86; RR 16 Cardiovascular, pulmonary, and abdominal exam are within normal limits. Neurological Examination: Mental Status: Alert and oriented x 3, 3/3 recall in 3 minutes, language fluent. -

Brainstem: Structure & Its Mode of Action
Journal of Neurology & Neurophysiology 2021, Vol.12, Issue 3, 521 Opinion Brainstem: Structure & Its Mode of action Karthikeyan Rupani Research Fellow, Tata Medical Centre, India. Corresponding Author* The brainstem is exceptionally little, making up around as it were 2.6 percent of the brain's add up to weight. It has the basic parts of directing cardiac, and Rupani K, respiratory work, making a difference to control heart rate and breathing rate. Research Fellow, Tata Medical Centre, India; It moreover gives the most engine and tactile nerve supply to the confront and E-mail: [email protected] neck by means of the cranial nerves. Ten sets of cranial nerves come from the brainstem. Other parts incorporate the direction of the central apprehensive Copyright: 2021 Rupani K. This is an open-access article distributed under the framework and the body's sleep cycle. It is additionally of prime significance terms of the Creative Commons Attribution License, which permits unrestricted within the movement of engine and tangible pathways from the rest of the use, distribution, and reproduction in any medium, provided the original author brain to the body, and from the body back to the brain. These pathways and source are credited. incorporate the corticospinal tract (engine work), the dorsal column-medial lemniscus pathway and the spinothalamic tract [3]. The primary part of the brainstem we'll consider is the midbrain. The midbrain Received 01 March 2021; Accepted 15 March 2021; Published 22 March 2021 (too known as the mesencephalon) is the foremost prevalent of the three districts of the brainstem. It acts as a conduit between the forebrain over and the pons and cerebellum underneath. -

Cranial Nerve Palsy
Cranial Nerve Palsy What is a cranial nerve? Cranial nerves are nerves that lead directly from the brain to parts of our head, face, and trunk. There are 12 pairs of cranial nerves and some are involved in special senses (sight, smell, hearing, taste, feeling) while others control muscles and glands. Which cranial nerves pertain to the eyes? The second cranial nerve is called the optic nerve. It sends visual information from the eye to the brain. The third cranial nerve is called the oculomotor nerve. It is involved with eye movement, eyelid movement, and the function of the pupil and lens inside the eye. The fourth cranial nerve is called the trochlear nerve and the sixth cranial nerve is called the abducens nerve. They each innervate an eye muscle involved in eye movement. The fifth cranial nerve is called the trigeminal nerve. It provides facial touch sensation (including sensation on the eye). What is a cranial nerve palsy? A palsy is a lack of function of a nerve. A cranial nerve palsy may cause a complete or partial weakness or paralysis of the areas served by the affected nerve. In the case of a cranial nerve that has multiple functions (such as the oculomotor nerve), it is possible for a palsy to affect all of the various functions or only some of the functions of that nerve. What are some causes of a cranial nerve palsy? A cranial nerve palsy can occur due to a variety of causes. It can be congenital (present at birth), traumatic, or due to blood vessel disease (hypertension, diabetes, strokes, aneurysms, etc). -

Interruption of the Connections of the Mammillary Bodies Protects Against Generalized Pentylenetetrazol Seizures in Guinea Pigs
The Journal of Neuroscience, March 1987, 7(3): 662-670 Interruption of the Connections of the Mammillary Bodies Protects Against Generalized Pentylenetetrazol Seizures in Guinea Pigs Marek A. Mirski and James A. Ferrendelli Division of Clinical Neuropharmacology, Department of Pharmacology and Department of Neurology and Neurological Surgery, Washington University School of Medicine, St. Louis, Missouri 63110 Electrolytic lesions in the anterior and mid-diencephalon and Morin, 1953; Gellhorn et al., 1959) fields of Fore1(Jinnai, 1966; ventral midbrain in guinea pigs were produced to examine Jinnai et al., 1969; Jinnai and Mukawa, 1970), substantianigra the effects of interruption of the fornix (FX), mammillothal- (Iadarola and Gale, 1982; Garant and Gale, 1983; Gonzalez and amic tracts (MT), and mammillary peduncles (MP), respec- Hettinger, 1984; McNamara et al., 1983, 1984), and several tively, on the expression of pentylenetetrazol (PTZ) sei- thalamic nuclei (Mullen et al., 1967; Jinnai et al., 1969; Feeney zures. As a group, all mid-diencephalic lesioned animals and Gullotta, 1972; Kusske et al., 1972; Van Straaten, 1975; had some degree of protection from the electroencephalo- Quesney et al., 1977). graphic and behavioral convulsant and lethal effects of the Recently we observed the selective metabolic activation of drug. Through a composite volume analysis of protected the mammillary bodies (MB) and their immediate connections versus unprotected animals, as well as a retrospective com- during a threshold convulsive stimulus induced by the co-in- parison between MT and non-MT lesioned animals, it was fusion of pentylenetetrazol (PTZ) and ethosuximide (ESM) demonstrated that small mid-diencephalic lesions incorpo- (Mirski and Ferrendelli, 1983). -
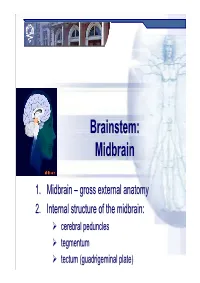
Brainstem: Midbrainmidbrain
Brainstem:Brainstem: MidbrainMidbrain 1.1. MidbrainMidbrain –– grossgross externalexternal anatomyanatomy 2.2. InternalInternal structurestructure ofof thethe midbrain:midbrain: cerebral peduncles tegmentum tectum (guadrigeminal plate) Midbrain MidbrainMidbrain –– generalgeneral featuresfeatures location – between forebrain and hindbrain the smallest region of the brainstem – 6-7g the shortest brainstem segment ~ 2 cm long least differentiated brainstem division human midbrain is archipallian – shared general architecture with the most ancient of vertebrates embryonic origin – mesencephalon main functions:functions a sort of relay station for sound and visual information serves as a nerve pathway of the cerebral hemispheres controls the eye movement involved in control of body movement Prof. Dr. Nikolai Lazarov 2 Midbrain MidbrainMidbrain –– grossgross anatomyanatomy dorsal part – tectum (quadrigeminal plate): superior colliculi inferior colliculi cerebral aqueduct ventral part – cerebral peduncles:peduncles dorsal – tegmentum (central part) ventral – cerebral crus substantia nigra Prof. Dr. Nikolai Lazarov 3 Midbrain CerebralCerebral cruscrus –– internalinternal structurestructure CerebralCerebral peduncle:peduncle: crus cerebri tegmentum mesencephali substantia nigra two thick semilunar white matter bundles composition – somatotopically arranged motor tracts: corticospinal } pyramidal tracts – medial ⅔ corticobulbar corticopontine fibers: frontopontine tracts – medially temporopontine tracts – laterally -

Clones in the Chick Diencephalon Contain Multiple Cell Types and Siblings Are Widely Dispersed
Development 122, 65-78 (1996) 65 Printed in Great Britain © The Company of Biologists Limited 1996 DEV8292 Clones in the chick diencephalon contain multiple cell types and siblings are widely dispersed Jeffrey A. Golden1,2 and Constance L. Cepko1,3 1Department of Genetics, Harvard Medical School, 2Department of Pathology, Brigham and Women’s Hospital, and 3Howard Hughes Medical Institute, 200 Longwood Avenue, Boston, MA 02115, USA SUMMARY The thalamus, hypothalamus and epithalamus of the ver- clones dispersed in all directions, resulting in sibling cells tebrate central nervous system are derived from the populating multiple nuclei within the diencephalon. In embryonic diencephalon. These regions of the nervous addition, several distinctive patterns of dispersion were system function as major relays between the telencephalon observed. These included clones with siblings distributed and more caudal regions of the brain. Early in develop- bilaterally across the third ventricle, clones that originated ment, the diencephalon morphologically comprises distinct in the lateral ventricle, clones that crossed neuromeric units known as neuromeres or prosomeres. As development boundaries, and clones that crossed major boundaries of proceeds, multiple nuclei, the functional and anatomical the developing nervous system, such as the diencephalon units of the diencephalon, derive from the neuromeres. It and mesencephalon. These findings demonstrate that prog- was of interest to determine whether progenitors in the enitor cells in the diencephalon are multipotent and that diencephalon give rise to daughters that cross nuclear or their daughters can become widely dispersed. neuromeric boundaries. To this end, a highly complex retroviral library was used to infect diencephalic progeni- tors. Retrovirally marked clones were found to contain Key words: cell lineage, central nervous system, diencephalon, neurons, glia and occasionally radial glia. -

The Brain Stem Medulla Oblongata
Chapter 14 The Brain Stem Medulla Oblongata Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. Central sulcus Parietal lobe • embryonic myelencephalon becomes Cingulate gyrus leaves medulla oblongata Corpus callosum Parieto–occipital sulcus Frontal lobe Occipital lobe • begins at foramen magnum of the skull Thalamus Habenula Anterior Epithalamus commissure Pineal gland • extends for about 3 cm rostrally and ends Hypothalamus Posterior commissure at a groove between the medulla and Optic chiasm Mammillary body pons Cerebral aqueduct Pituitary gland Fourth ventricle Temporal lobe • slightly wider than spinal cord Cerebellum Midbrain • pyramids – pair of external ridges on Pons Medulla anterior surface oblongata – resembles side-by-side baseball bats (a) • olive – a prominent bulge lateral to each pyramid • posteriorly, gracile and cuneate fasciculi of the spinal cord continue as two pair of ridges on the medulla • all nerve fibers connecting the brain to the spinal cord pass through the medulla • four pairs of cranial nerves begin or end in medulla - IX, X, XI, XII Medulla Oblongata Associated Functions • cardiac center – adjusts rate and force of heart • vasomotor center – adjusts blood vessel diameter • respiratory centers – control rate and depth of breathing • reflex centers – for coughing, sneezing, gagging, swallowing, vomiting, salivation, sweating, movements of tongue and head Medulla Oblongata Nucleus of hypoglossal nerve Fourth ventricle Gracile nucleus Nucleus of Cuneate nucleus vagus -

Isolated Relative Afferent Pupillary Defect Secondary to Contralateral Midbrain Compression
OBSERVATION Isolated Relative Afferent Pupillary Defect Secondary to Contralateral Midbrain Compression Cheun Ju Chen, MD; Mia Scheufele, MD; Maushmi Sheth, MD; Amir Torabi, MD; Nick Hogan, MD, PhD; Elliot M. Frohman, MD, PhD Background: Relative afferent pupillary defects are typi- accounts for the relative afferent pupillary defect con- cally related to ipsilateral lesions within the anterior vi- tralateral to the described lesion. sual pathways. Result: Magnetic resonance imaging of the brain revealed a pineal tumor compressing the right rostral midbrain. Objective: To describe a patient who had a workup for headache and was found to have an isolated left relative Conclusion: While rare, a relative afferent pupillary de- afferent pupillary defect without any other neurological fect can occasionally occur secondary to lesions in the findings. postchiasmal pathways. In these circumstances, the pu- pillary defect will be observed to be contralateral to the Design: We review the neuroanatomy of the pupil- side of the lesion. lary light reflex pathway and emphasize the nasotem- poral bias of decussating fiber projections, which Arch Neurol. 2004;61:1451-1453 RELATIVE AFFERENT PUPIL- though retinal fibers concerned with this lary defect (RAPD) is char- reflex transmit information to both the ip- acterized by pupillary dila- silateral and contralateral midbrain, there tion upon illuminating the is a slight crossing bias, with about 53% of eye during the swinging the fibers crossing in the optic chiasm Aflashlight test. The presence of this sign sig- (chiefly derived from the nasal retina) and nifies an abnormality in the transmission 47% remaining ipsilateral. This anatomi- of light information within the pupillary cal organization of the pupillary constric- light constrictor pathway from the retina tor pathway results in the possibility of pro- to the rostral midbrain circuitry involved ducing an RAPD during illumination of the in this reflex. -

Measurement of the Normal Optic Chiasm on Coronal MR Images
Measurement of the Normal Optic Chiasm on Coronal MR Images Andrew L. Wagner, F. Reed Murtagh, Ken S. Hazlett, and John A. Arrington PURPOSE: To develop an objective method for measuring the optic chiasm and to document its normal range in size. METHODS: Measurements of the height and area of the optic chiasm, made on coronal T1-weighted MR images with the use of commercially available region-of-interest software, were obtained in 114 healthy subjects who had a total of 123 MR studies. A normal range and standard deviation were calculated, and the information was broken down by age and sex. RESULTS: The mean area of the optic chiasm was 43.7 mm2, with a standard deviation of 5.21. The mean width was 14.0 mm, with a standard deviation of 1.68. CONCLUSION: The area and width of the optic chiasm can be measured with the use of commercially available software, which allows an objective estimate of the chiasm’s size. Knowledge of the normal size range of the optic chiasm can be helpful in the early detection of some disorders. Index terms: Optic chiasm; Brain, anatomy; Brain, measurement AJNR Am J Neuroradiol 18:723–726, April 1997 The optic chiasm is an important land- months and that had been interpreted as normal. No pa- mark when interpreting magnetic resonance (MR) tient had suspected visual or endocrine abnormalities. All examinations of the brain. A small chiasm can be the examinations had been performed with a 1.5-T Gen- an indication of several disorders, the most com- eral Electric (Milwaukee, Wis) Signa or 1.5-T Siemens mon of which is septooptic dysplasia (1), and a (Cary, NC) Somatom MR system using routine imaging large chiasm can be the result of glioma, menin- protocols, with additional 3-mm T1-weighted contiguous coronal sections used for measurements. -

Differentiation of the Cerebellum 2463
Development 128, 2461-2469 (2001) 2461 Printed in Great Britain © The Company of Biologists Limited 2001 DEV1660 Inductive signal and tissue responsiveness defining the tectum and the cerebellum Tatsuya Sato, Isato Araki‡ and Harukazu Nakamura* Department of Molecular Neurobiology, Institute of Development, Aging and Cancer, Seiryo-machi 4-1, Aoba-ku, Sendai 980- 8575, Japan ‡Present address: Department of Neurobiology, University of Heidelberg, Im Neuenheimer Feld 364, D-69120 Heidelberg, Germany *Author for correspondence (e-mail: [email protected]) Accepted 11 April 2001 SUMMARY The mes/metencephalic boundary (isthmus) has an Fgf8b repressed Otx2 expression, but upregulated Gbx2 and organizing activity for mesencephalon and metencephalon. Irx2 expression in the mesencephalon. As a result, Fgf8b The candidate signaling molecule is Fgf8 whose mRNA is completely changed the fate of the mesencephalic alar plate localized in the region where the cerebellum differentiates. to cerebellum. Quantitative analysis showed that Fgf8b Responding to this signal, the cerebellum differentiates in signal is 100 times stronger than Fgf8a signal. Co- the metencephalon and the tectum differentiates in the transfection of Fgf8b with Otx2 indicates that Otx2 is a key mesencephalon. Based on the assumption that strong Fgf8 molecule in mesencephalic generation. We have shown by signal induces the cerebellum and that the Fgf8b signal is RT-PCR that both Fgf8a and Fgf8b are expressed, Fgf8b stronger than that of Fgf8a, we carried out experiments to expression prevailing in the isthmic region. The results all misexpress Fgf8b and Fgf8a in chick embryos. Fgf8a did not support our working hypothesis that the strong Fgf8 signal affect the expression pattern of Otx2, Gbx2 or Irx2. -

Congenital Oculomotor Palsy: Associated Neurological and Ophthalmological Findings
CONGENITAL OCULOMOTOR PALSY: ASSOCIATED NEUROLOGICAL AND OPHTHALMOLOGICAL FINDINGS M. D. TSALOUMAS1 and H. E. WILLSHA W2 Birmingham SUMMARY In our group of patients we found a high incidence Congenital fourth and sixth nerve palsies are rarely of neurological abnormalities, in some cases asso associated with other evidence of neurological ahnor ciated with abnormal findings on CT scanning. mality, but there have been conflicting reports in the Aberrant regeneration, preferential fixation with literature on the associations of congenital third nerve the paretic eye, amblyopia of the non-involved eye palsy. In order to clarify the situation we report a series and asymmetric nystagmus have all been reported as 1 3 7 of 14 consecutive cases presenting to a paediatric associated ophthalmic findings. - , -9 However, we tertiary referral service over the last 12 years. In this describe for the first time a phenomenon of digital lid series of children, 5 had associated neurological elevation to allow fixation with the affected eye. Two abnormalities, lending support to the view that con children demonstrated this phenomenon and in each genital third nerve palsy is commonly a manifestation of case the accompanying neurological defect was widespread neurological damage. We also describe for profound. the first time a phenomenon of digital lid elevation to allow fixation with the affected eye. Two children demonstrated this phenomenon and in each case the PATIENTS AND METHODS accompanying neurological defect was profound. The Fourteen children (8 boys, 6 girls) with a diagnosis of frequency and severity of associated deficits is analysed, congenital oculomotor palsy presented to our paed and the mechanism of fixation with the affected eye is iatric tertiary referral centre over the 12 years from discussed. -
NERVOUS SYSTEM هذا الملف لالستزادة واثراء المعلومات Neuropsychiatry Block
NERVOUS SYSTEM هذا الملف لﻻستزادة واثراء المعلومات Neuropsychiatry block. قال تعالى: ) َو َل َق د َخ َل قنَا ا ِْلن َسا َن ِمن ُس ََل َل ة ِ من ِطي ن }12{ ثُ م َجعَ لنَاه ُ نُ ط َفة فِي َق َرا ر م ِكي ن }13{ ثُ م َخ َل قنَا ال ُّن ط َفة َ َع َل َقة َف َخ َل قنَا ا لعَ َل َقة َ ُم ضغَة َف َخ َل قنَا ا ل ُم ضغَة َ ِع َظا ما َف َك َس ونَا ا ل ِع َظا َم َل ح ما ثُ م أَن َشأنَاه ُ َخ ل قا آ َخ َر َفتَبَا َر َك ّللا ُ أَ ح َس ُن ا ل َخا ِل ِقي َن }14{( Resources BRS Embryology Book. Pathoma Book ( IN DEVELOPMENTAL ANOMALIES PART ). [email protected] 1 OVERVIEW A- Central nervous system (CNS) is formed in week 3 of development, during which time the neural plate develops. The neural plate, consisting of neuroectoderm, becomes the neural tube, which gives rise to the brain and spinal cord. B- Peripheral nervous system (PNS) is derived from three sources: 1. Neural crest cells 2. Neural tube, which gives rise to all preganglionic autonomic nerves (sympathetic and parasympathetic) and all nerves (-motoneurons and -motoneurons) that innervate skeletal muscles 3. Mesoderm, which gives rise to the dura mater and to connective tissue investments of peripheral nerve fibers (endoneurium, perineurium, and epineurium) DEVELOPMENT OF THE NEURAL TUBE Neurulation refers to the formation and closure of the neural tube. BMP-4 (bone morphogenetic protein), noggin (an inductor protein), chordin (an inductor protein), FGF-8 (fibroblast growth factor), and N-CAM (neural cell adhesion molecule) appear to play a role in neurulation.