1-Cerumen-Impaction.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

UPDATE VOLUME 20 • ISSUE 3 the Newsletter of the Council for Accreditation in Occupational Hearing Conservation
Fall 2008 UPDATE VOLUME 20 • ISSUE 3 The Newsletter of the Council for Accreditation in Occupational Hearing Conservation Hearing noise-induced hearing loss and further degradation of communication. If too much hearing protection is provided, Conservation the combined effects of the hearing loss and the attenuation provided by the hearing protector may result in critical sounds for the Hearing- and communication signals becoming inaudible. I’m often asked what type of hearing protector is best for Impaired Worker workers with hearing impairment. Considering that there is no ‘best’ HPD for all workers in any hearing category, it Introduction by Ted Madison should come as no surprise that no single type of device will The prevalence of hearing loss among persons enrolled meet the needs of all those with hearing loss. What seems in occupational hearing conservation programs (HCPs) is to be consistent, however, is that each case is unique, and difficult to determine. Recently, Tak and Calvert (2008) that extra time and effort is required to help these workers estimated that 11.4% of the overall US workforce reports find the right combination of protection, having hearing difficulty of varying communication and auditory awareness. degrees and that approximately ¼ of Consultation with an audiologist or other the hearing difficulty reported can hearing health care professional is also be attributed to employment. These an important step in most cases. estimates are based on analysis of data One valuable resource is the OSHA from the US National Health Interview Safety & Health Information Bulletin Survey (NHIS) that were collected (SHIB) titled “Hearing Conservation from 1997 to 2003. -

Instruction Sheet: Otitis Externa
University of North Carolina Wilmington Abrons Student Health Center INSTRUCTION SHEET: OTITIS EXTERNA The Student Health Provider has diagnosed otitis externa, also known as external ear infection, or swimmer's ear. Otitis externa is a bacterial/fungal infection in the ear canal (the ear canal goes from the outside opening of the ear to the eardrum). Water in the ear, from swimming or bathing, makes the ear canal prone to infection. Hot and humid weather also predisposes to infection. Symptoms of otitis externa include: ear pain, fullness or itching in the ear, ear drainage, and temporary loss of hearing. These symptoms are similar to those caused by otitis media (middle ear infection). To differentiate between external ear infection and middle ear infection, the provider looks in the ear with an instrument called an otoscope. It is important to distinguish between the two infections, as they are treated differently: External otitis is treated with drops in the ear canal, while middle ear infection is sometimes treated with an antibiotic by mouth. MEASURES YOU SHOULD TAKE TO HELP TREAT EXTERNAL EAR INFECTION: 1. Use the ear drops regularly, as directed on the prescription. 2. The key to treatment is getting the drops down into the canal and keeping the medicine there. To accomplish this: Lie on your side, with the unaffected ear down. Put three to four drops in the infected ear canal, then gently pull the outer ear back and forth several times, working the medicine deeper into the ear canal. Remain still, good-ear-side-down for about 15 minutes. -

The Ear, Nose, and Throat Exam Jeffrey Texiera, MD and Joshua Jabaut, MD CPT, MC, USA LT, MC, USN
The Ear, Nose, and Throat Exam Jeffrey Texiera, MD and Joshua Jabaut, MD CPT, MC, USA LT, MC, USN Midatlantic Regional Occupational and Environmental Medicine Conference Sept. 23, 2017 Disclosures ●We have no funding or financial interest in any product featured in this presentation. The items included are for demonstration purposes only. ●We have no conflicts of interest to disclose. Overview ● Overview of clinically oriented anatomy - presented in the format of the exam ● The approach ● The examination ● Variants of normal anatomy ● ENT emergencies ● Summary/highlights ● Questions Anatomy ● The head and neck exam consists of some of the most comprehensive and complicated anatomy in the human body. ● The ear, nose, and throat comprise a portion of that exam and a focused clinical encounter for an acute ENT complaint may require only this portion of the exam. Ears www.Medscape.com www.taqplayer.info Ear – Vestibular organ www.humanantomylibrary.com Nose/Sinus Anatomy Inferior Middle Turbinate Turbinate Septum Dorsum Sidewalls Ala Floor Tip www.ENT4Students.blogspot.com Columella Vestibule www.beautyepic.com Oral cavity and oropharynx (throat) www.apsubiology.org Neck www.rdhmag.com The Ear, Nose, and Throat exam Perform in a standardized systematic way that works for you Do it the same way every time, this mitigates risk of missing a portion of the exam Practice the exam to increase comfort with performance and familiarize self with variants of normal Describe what you are doing to the patient, describe what you see in your documentation Use your PPE as appropriate A question to keep in mind… ●T/F: The otoscope is the optimal tool for examining the tympanic membrane. -

Personal Hearing Protection Devices ______
Safe Operating Procedure (Revised 10/14) PERSONAL HEARING PROTECTION DEVICES _____________________________________________________________________ When employees are exposed to sound levels in excess of occupational exposure or action limits, the first course of action is to reduce the noise with source and pathway controls (engineering controls). When sound levels cannot be reduced to less than an 8-hour Time Weighted Average (TWA) of 85 dBA through source and pathway control(s) and/or receiver controls (administrative controls), hearing protection should be used to protect workers from work-related hearing loss. Choosing the right kind of hearing protective device and correct use are essential to protection from hazardous noise exposures. This SOP describes the most common types of hearing protectors used at UNL. There may be specialty hearing protectors prescribed for certain UNL employees exposed to impulse noises which are not addressed in this SOP. Regardless, all employees participating in UNL’s Hearing Conservation Program will receive instruction in proper use of the hearing protectors prescribed for their exposure situation. Types of Hearing Protection There are two main types of hearing protection devices: ear plugs and ear muffs. Ear Plugs Ear plugs (figure 1) are commonly available in the following styles: roll-down foam; pre-molded; and semi-insert. Roll-down foam earplugs are rolled before each use and inserted into the ear canals. They conform to the shape of individual’s ear canals. One size of roll-down foam will fit most workers although workers with extremely small or large ear canals may need a different size. One disadvantage of roll-down foam ear plugs is that workers need to roll them each time they wear them, thus making it harder to use if workers have to take ear plugs out frequently during a work shift. -

Older Adult Hearing Loss and Screening Key Points • Eighty Percent of Older American Adults Have Untreated Hearing Loss. •
Older Adult Hearing Loss and Screening Key Points Eighty percent of older American adults have untreated hearing loss. Hearing loss is associated with decreased quality of life, depression, communication disorders, social withdrawal and cognitive impairment. Overview Definition Presbycusis is another term for age-related sensorineural hearing loss (ARHL). o Damage to the cochlea, Cranial Nerve VIII, or Internal Auditory canal o Bilateral, symmetric, high-frequency sensorineural hearing loss Noise-induced hearing loss (NIHL) o Direct mechanical injury to sensory hair cells in the cochlea o Continuous noise exposure Aging and hearing loss Cell reduction in auditory cortex Acoustic nerve (CN VIII) fiber degeneration Inner ear sensory cell loss and membrane calcification Risk Factors Advancing Age (ARHI) Exposure to loud noises or ototoxic agents (i.e. loud machinery) (NIHL) Other External ear or middle ear conductive hearing loss risk factors include: o Cerumen impaction o Middle ear fluid o Perforated tympanic membrane Assessment Recommendations for hearing assessments: Screening all older adults over the age of 65 years. Screening should be conducted in a primary care setting. Obtain history of chronic medical conditions (diabetes mellitus, CAD), ear infections, ear trauma, occupation Medication review assessing for use of diuretics (loop), aspirin, antineoplastic (cisplatin, 5- fluorouracil), antimalarial (chloroquine, quinine), and antibiotic (aminoglycosides, erythromycin, tetracycline, vancomycin) Assessment Instruments available include: o Hearing Handicap Inventory for the Elderly Screening (HHIE-S) https://www.audiology.org/sites/default/files/PracticeManagement/Medicare_HHI.pdf . 10 question questionnaire . Score greater than 10 points should be referred to an audiologist o Audio Scope (Welch Allyn, Inc.) . Otoscope examination . Test hearing o Whispered Voice Test, finger rub or a watch tick test o Ask the question - “Do you have a hearing problem now?” If any of the above four are positive – referral to an Audiologist is indicated. -
Digital Active Noise Reduction (DANR) Custom Earplugs PIN 05-021001
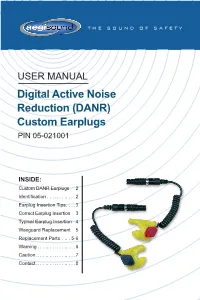
THE SOUND OF SAFETY USER MANUAL Digital Active Noise Reduction (DANR) Custom Earplugs PIN 05-021001 INSIDE: Custom DANR Earplugs 2 Identification . 2 Earplug Insertion Tips . 3 Correct Earplug Insertion 3 Typical Earplug Insertion 4 Waxguard Replacement 5 Replacement Parts . 5-6 Warning . 6 Caution . 7 Contact . 8 DANR Custom Earplugs Connectors Coiled Cables Left Earplug Right Earplug (blue) (red) Replaceable Engraved Serial Waxguard Number Identification Each earplug is molded with a serial number that is used to identify the user. There is a ‘P’ at the beginning of each serial number to indicate the text orientation. 2 | DANR THP & THPC EARPLUGS Earplug Insertion Tips • Inspect the earplugs before each use. The earplugs should be free of debris, Helix tears, and other physical damage. Tip • Inspect the coiled cable and the cable connection to the earplug. Left Earplug Right Earplug • Lubricate the earplugs with water or Aegisound Ear Gel around the canal tip, being careful not to allow water or gel into the opening at the earplug tip. • Gently insert the tip of the earplug into the ear canal with the helix rotated forward. • Rotate the earplug backwards while pushing the earplug until the tip slides into the canal and the helix fits into the pocket at the top of the ear. Correct Earplug Insertion Correct Incorrect Insertion Insertion (Earplug (Earplug not locked locked in in helix) helix) Custom Earplug Familiarization • Wearing the custom earplugs for long periods of time may require an adjustment period of a week or more. • Begin by wearing earplugs for one hour at a time for the first several days. -

Honeywell Howard Leight Arc Flash Protection Brochure
SOUNDSOURCE™ NO. 7-NA-US Arc Flash Protection What requirements must a hearing protector meet for arc flash protection? Arc flash is the term describing an extremely dangerous electrical hazard when uncontrolled current passes through the air between two conductors. When voltage is high enough (over 480V), the intense heat of the arc flash can create a serious hazard for workers in the arc flash zone; temperatures can reach 35,000° F, and the impulse sound resulting from the explosive expansion from the arc can exceed 160 dB peak. Shrapnel from an arc blast can be propelled over 700 mph. Each year, more than 2,000 persons are treated for arc flash burns (NFPA 70E-2015, Annex K). The National Fire Protection Association publishes its NFPA 70E Standard for Electrical Safety in the Workplace1, which defines arc flash boundary zones, and recommended PPE (personal protective equipment) for each zone. The FAQs on the next page summarize the requirements for hearing protection defined in NFPA 70E-2015. Are hearing protectors required for arc flash hazard zones, according to NFPA 70E ? References: Yes, the 2015 standard requires workers in an arc flash hazard zone to wear insert-type 1. National Fire Protection hearing protection (earplugs), as defined in Section 130.7(C)(5)). Association, NFPA 70E®: Standard for Electrical Safety Does NFPA certify or approve particular hearing protectors as being compliant with in the Workplace®, NFPA 70E-2015? No, the NFPA does not certify or approve any PPE. Any manufacturer 2015 edition. claims that a particular piece of PPE has been tested to NFPA standards, or has been 2. -

Ear Infections in Children
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES ∙ National Institutes of Health NIDCD Fact Sheet | Hearing and Balance Ear Infections in Children What is an ear infection? How can I tell if my child has an ear infection? An ear infection is an inflammation of the middle ear, usually caused by bacteria, that occurs when fluid builds Most ear infections happen to children before they’ve up behind the eardrum. Anyone can get an ear infection, learned how to talk. If your child isn’t old enough to say but children get them more often than adults. Five out of “My ear hurts,” here are a few things to look for: six children will have at least one ear infection by their third } Tugging or pulling at the ear(s) birthday. In fact, ear infections are the most common reason parents bring their child to a doctor. The scientific name for } Fussiness and crying an ear infection is otitis media (OM). } Trouble sleeping What are the symptoms of an } Fever (especially in infants and younger children) ear infection? } Fluid draining from the ear } Clumsiness or problems with balance There are three main types of ear infections. Each has a different combination of symptoms. } Trouble hearing or responding to quiet sounds. } Acute otitis media (AOM) is the most common ear What causes an ear infection? infection. Parts of the middle ear are infected and swollen and fluid is trapped behind the eardrum. This An ear infection usually is caused by bacteria and often causes pain in the ear—commonly called an earache. -

Differential Diagnosis and Treatment of Hearing Loss JON E
Differential Diagnosis and Treatment of Hearing Loss JON E. ISAACSON, M.D., and NEIL M. VORA, M.D., Milton S. Hershey Medical Center, Hershey, Pennsylvania Hearing loss is a common problem that can occur at any age and makes verbal communication difficult. The ear is divided anatomically into three sections (external, middle, and inner), and pathology contributing to hearing loss may strike one or more sections. Hearing loss can be cat- egorized as conductive, sensorineural, or both. Leading causes of conductive hearing loss include cerumen impaction, otitis media, and otosclerosis. Leading causes of sensorineural hear- ing loss include inherited disorders, noise exposure, and presbycusis. An understanding of the indications for medical management, surgical treatment, and amplification can help the family physician provide more effective care for these patients. (Am Fam Physician 2003;68:1125-32. Copyright© 2003 American Academy of Family Physicians) ore than 28 million Amer- tive, the sound will be heard best in the icans have some degree of affected ear. If the loss is sensorineural, the hearing impairment. The sound will be heard best in the normal ear. differential diagnosis of The sound remains midline in patients with hearing loss can be sim- normal hearing. Mplified by considering the three major cate- The Rinne test compares air conduction gories of loss. Conductive hearing loss occurs with bone conduction. The tuning fork is when sound conduction is impeded through struck softly and placed on the mastoid bone the external ear, the middle ear, or both. Sen- (bone conduction). When the patient no sorineural hearing loss occurs when there is a longer can hear the sound, the tuning fork is problem within the cochlea or the neural placed adjacent to the ear canal (air conduc- pathway to the auditory cortex. -

Endoscopy in Birds, Reptiles, Amphibians and Fish
ENDOSCOPY IN BIRDS, REPTILES, AMPHIBIANS AND FISH Michael J. MURRAY Bernd SCHILDGER Michael TAYLOR 2 Endoscopy in Birds, Reptiles, Amphibians and Fish Endoscopy in Birds, Reptiles, Amphibians and Fish 3 Important notes: Endoscopy in Birds, Reptiles, Amphibians and Fish Medical knowledge is ever changing. As new Michael J. Murray, DVM, U.S.A. research and clinical experience broaden our Bernd Schildger, DVM, Switzerland knowledge, changes in treat ment and therapy Michael Taylor, DVM, Canada may be required. The authors and editors of the material herein have consulted sources believed to be reliable in their efforts to pr ovide Correspondence address of the author: information that is complete and in accord with the standards accept ed at the time of Michael J. Murray, DVM publication. However, in view of the possibili ty Avian and Exotic Clinic of Monterey Peninsula of human error by the authors, editors, or 2 Harris Court Suite A-1 publisher, or changes in medical knowledge, Monterey, CA 93940 neither the authors, editors, publisher, nor Phone: +1 8 31-6 47-11 47 any other party who has been involved in Fax: +1 8 31-3 73-44 82 the preparation of this booklet, warrants that the information contained herein is in every Bernd Schildger, DVM respect accurate or complete, and they are Tierpark Dählhölzli, Director not responsible for any errors or omissions Tierparkweg 1 or for the results obtained from use of such CH-3005 Bern, Switzerland information. The information contained within Phone: +41 3 13 57 15 15 this booklet is intended for use by doctors Fax: +41 3 13 57 15 10 and other health care professionals. -

Measurements of Earplug Attenuation Under Supra-Aural and Circumaural Headphones
International Journal of Audiology 2012; 51: 730–738 Original Article Measurements of earplug attenuation under supra-aural and circumaural headphones Jennifer B. Tufts* , Jillian V. Palmer * & Lynne Marshall† *Department of Communication Sciences, University of Connecticut, Storrs, USA, and †Naval Submarine Medical Research Laboratory, Groton, Connecticut, USA Abstract Objective: Supra-aural audiometric headphones are generally not recommended for use in measuring the attenuation of earplugs, because contact between the headphone and pinna and/or earplug could alter the attenuation obtained, and because of concerns of non-comparability between modes of excitation from supra-aural headphones and the sound-fi eld procedure required by the standardized method. In this study, we compared measurements of earplug attenuation obtained under Telephonics TDH-50P supra-aural headphones with measurements obtained under circumaural headphones designed expressly for such testing. Design: The attenuation of three types of earplugs (foam, premolded quadruple-fl ange, and custom-molded) was measured in a repeated-measures design. Study sample: The study sample comprised 42 normal-hearing adults (21 females, 21 males). Results: With the foam earplugs, nearly all of the attenuation measurements under the supra-aural headphones fell within 10 dB of the measurements under the circumaural headphones. With the fl ange and custom earplugs, approximately 10% of individuals obtained spuriously high attenuation under the supra-aural headphones. Conclusions: We conclude that standard supra-aural audiometric headphones are suitable for measuring the attenuation provided by foam earplugs. However, supra-aural headphones should not be used to measure the attenuation of fl ange or custom-molded earplugs. The potential exists for substantial over-estimation of attenuation, especially of custom plugs. -

DBZ-Earplug Instructions 110518.Indd
For best results follow video instructions at www.decibullz.com/earplug-instructions 3 SHAPE WHAT IS INCLUDED 7 Place ONE mold in the hot water. Multiple molds 5 Let cool for 5 minutes before removing, repeat HEAT WILL stick together if heated at the same time. steps 1-7 with the other mold and ear. (fig. 7) Let sit for 5 minutes. (fig. 3) Insert the mold into your ear and firmly press 1 the back plug into the ear canal (fig. 5) Left and Right 2 Back Plugs S, M, L Triple Flange Attach back plug and correct size silicone tip to custom mold. (fig. 1) Custom Mold Silicone Tips* (NRR 24) DO NOT USE FOAM TIPS FOR MOLDING You can change the tips after the molding process is complete. Check that the tip is securely attached before molding. If the tip CUSTOM MOLDED becomes dislodged in the ear canal seek medical attention. ✔ OR fig. 3 Back plug Silicone tip ✘ fig. 7 Medium Max INCORRECT CORRECT fig. 5 Isolation Foam Drawstring fig. 1 EARPLUG TIP Tips* (NRR 31) Carrying Pouch 4 : Use a mirror to see what you are doing, or have a friend help. To If, for any reason, you are not satisfied with your INSTRUCTIONS ensure a smooth looking mold, avoid using your finger-nails. Remove mold with metal spoon and let cool for Decibullz product, please contact us at 30 seconds. (fig. 4) CAUTION: ITEMS MAY BE VERY HOT. [email protected] before returning. WARNING! 2 Be sure to use a metal spoon, the mold WILL stick to plastic.