Wheeled Mobility and Seating Equipment Following Spinal Cord Injury
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Disability Classification System
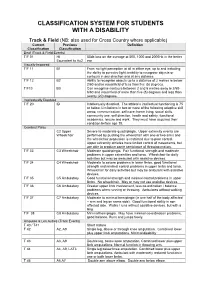
CLASSIFICATION SYSTEM FOR STUDENTS WITH A DISABILITY Track & Field (NB: also used for Cross Country where applicable) Current Previous Definition Classification Classification Deaf (Track & Field Events) T/F 01 HI 55db loss on the average at 500, 1000 and 2000Hz in the better Equivalent to Au2 ear Visually Impaired T/F 11 B1 From no light perception at all in either eye, up to and including the ability to perceive light; inability to recognise objects or contours in any direction and at any distance. T/F 12 B2 Ability to recognise objects up to a distance of 2 metres ie below 2/60 and/or visual field of less than five (5) degrees. T/F13 B3 Can recognise contours between 2 and 6 metres away ie 2/60- 6/60 and visual field of more than five (5) degrees and less than twenty (20) degrees. Intellectually Disabled T/F 20 ID Intellectually disabled. The athlete’s intellectual functioning is 75 or below. Limitations in two or more of the following adaptive skill areas; communication, self-care; home living, social skills, community use, self direction, health and safety, functional academics, leisure and work. They must have acquired their condition before age 18. Cerebral Palsy C2 Upper Severe to moderate quadriplegia. Upper extremity events are Wheelchair performed by pushing the wheelchair with one or two arms and the wheelchair propulsion is restricted due to poor control. Upper extremity athletes have limited control of movements, but are able to produce some semblance of throwing motion. T/F 33 C3 Wheelchair Moderate quadriplegia. Fair functional strength and moderate problems in upper extremities and torso. -

Reframing Sport Contexts: Labeling, Identities, and Social Justice
Reframing Sport Contexts: Labeling, Identities, and Social Justice Dr. Ted Fay and Eli Wolff Sport in Society Disability in Sport Initiative Northeastern University Critical Context • Marginalization (Current Status Quo) vs. • Legitimatization (New Inclusive Paradigm) Critical Context Naturalism vs. Trans-Humanism (Wolbring, G. (2009) How Do We Handle Our Differences related to Labeling Language and Cultural Identities? • Stereotyping? • Prejudice? • Discrimination? (Carr-Ruffino, 2003, p. 1) Ten Major Cultural Differences 1) Source of Control 2) Collectivism or Individualism 3) Homogeneous or Heterogeneous 4) Feminine or Masculine 5) Rank Status 6) Risk orientation 7) Time use 8) Space use 9) Communication Style 10) Economic System (Carr – Ruffino, 2003, p.27) Rationale for Inclusion • Divisioning by classification relative to “fair play” and equity principles • Sport model rather than “ism” segregated model (e.g., by race, gender, disability, socio-economic class, sexual orientation, look (body image), sect (religion), age) • Legitimacy • Human rights and equality Social Dynamics of Inequality Reinforce and reproduce Social Institutions Ideology Political (Patriarchy) Economic Educational Perpetuates Religious Prejudice & Are institutionalized by Discrimination Cultural Practices (ISM) Sport Music Art (Sage, 1998) Five Interlinking Conceptual Frameworks • Critical Change Factors Model (CCFM) • Organizational Continuum in Sport Governance (OCSG) • Criteria for Inclusion in Sport Organizations (CISO) • Individual Multiple Identity Sport Classifications Index (IMISCI) • Sport Opportunity Spectrum (SOS) Critical Change Factors Model (CCFM) F1) Change/occurrence of major societal event (s) affecting public opinion toward ID group. F2) Change in laws, government and court action in changing public policies toward ID group. F3) Change in level of influence of high profile ID group role models on public opinion. -

International Triathlon Union • ITU Competition Rules
ITU Competition Rules Approved by the ITU Executive Board, in November 2015 Green highlight – added as of November 2015 Red highlight – deleted as of November 2015 International Triathlon Union ITU Competition Rules 06-12-2015 1 The ITU Competition Rules is the master source document, found on ITU’s website at www.triathlon.org. The web based document acts as the official (authorised) reference document and is maintained based on authorised amendments in accordance with recommendations by the ITU Technical Committee and accepted by the ITU Executive Board. Contact International Triathlon Union (ITU) Maison du Sport International Av. de Rhodanie 54 Lausanne CH -1007, Switzerland Tel +41 21 614 60 30 Fax +41 21 614 60 39 Email: [email protected] For general information about ITU visit www.triathlon.org International Triathlon Union ITU Competition Rules 06-12-2015 2 TABLE OF CONTENTS 1. INTRODUCTION: _________________________________________________________________________ 4 2. CONDUCT OF ATHLETES: ___________________________________________________________________ 6 3. PENALTIES: _____________________________________________________________________________ 16 4. SWIMMING CONDUCT: ___________________________________________________________________ 20 5. CYCLING CONDUCT:______________________________________________________________________ 25 6. RUNNING CONDUCT: ____________________________________________________________________ 33 7. TRANSITION AREA CONDUCT: _____________________________________________________________ 34 8. COMPETITION -
Field Indicators of Hydric Soils
United States Department of Field Indicators of Agriculture Natural Resources Hydric Soils in the Conservation Service United States In cooperation with A Guide for Identifying and Delineating the National Technical Committee for Hydric Soils Hydric Soils, Version 8.2, 2018 Field Indicators of Hydric Soils in the United States A Guide for Identifying and Delineating Hydric Soils Version 8.2, 2018 (Including revisions to versions 8.0 and 8.1) United States Department of Agriculture, Natural Resources Conservation Service, in cooperation with the National Technical Committee for Hydric Soils Edited by L.M. Vasilas, Soil Scientist, NRCS, Washington, DC; G.W. Hurt, Soil Scientist, University of Florida, Gainesville, FL; and J.F. Berkowitz, Soil Scientist, USACE, Vicksburg, MS ii In accordance with Federal civil rights law and U.S. Department of Agriculture (USDA) civil rights regulations and policies, the USDA, its Agencies, offices, and employees, and institutions participating in or administering USDA programs are prohibited from discriminating based on race, color, national origin, religion, sex, gender identity (including gender expression), sexual orientation, disability, age, marital status, family/parental status, income derived from a public assistance program, political beliefs, or reprisal or retaliation for prior civil rights activity, in any program or activity conducted or funded by USDA (not all bases apply to all programs). Remedies and complaint filing deadlines vary by program or incident. Persons with disabilities who require alternative means of communication for program information (e.g., Braille, large print, audiotape, American Sign Language, etc.) should contact the responsible Agency or USDA’s TARGET Center at (202) 720-2600 (voice and TTY) or contact USDA through the Federal Relay Service at (800) 877-8339. -

A. Legal Permanent Resident Aliens
A. Classes Currently in Use - Legal Permanent Resident Aliens (continued) Symbol: *Arrival/ Statistical Document Adjust Section of Law Description FY AM1 AM-1 N Sec. 584(b)(1)(A) of Amerasian born in AM6 AM-6 A PL 100-202 Vietnam after (Dec. 22, 1987) Jan. 1, 1962 and before Jan. 1, 1976 who was fathered by a U.S. citizen. AM2 AM-2 N Sec. 584(b)(1)(B) of Spouse or child of an AM7 AM-7 A PL 100-202 alien classified as (Dec. 22, 1987) AM1 or AM6. AM3 AM-3 N Sec. 584(b)(1)(C) of Mother, guardian, or AM8 AM-8 A PL 100-202 next-of-kin of an (Dec. 22, 1987) alien classified as AM1 or AM6, and spouse or child of the mother, guardian, or next-of-kin. AR1 AR-1 N Sec. 201(b)(2)(A)(i) Amerasian child of a AR6 AR-6 A of the I&N Act and U.S. citizen born in 204(g) as added by Cambodia, Korea, PL 97-359 (Oct. 22, Laos, Thailand, or 1982) Vietnam (immediate relative child). AS6 AS-6 A Sec. 209(b) of the Asylee principal I&N Act as added by PL 96-212 (Mar. 17, 1980) AS7 AS-7 A Sec. 209(b) of the Spouse of an alien I&N Act as added by classified as AS6. PL 96-212 (Mar. 17, 1980) AS8 AS-8 A Sec. 209(b) of the Child of an alien I&N Act as added by classified as AS6. -

Connexion Client Cataloging Quick Reference
OCLC Connexion Client Cataloging Quick Reference Introduction Keystroke shortcuts The Connexion client is a Windows-based interface to OCLC • Use default keystroke shortcuts or assign your own to activate Connexion® used to access WorldCat for cataloging. commands, insert characters, run macros, and insert text strings. This quick reference provides brief instructions for editing, saving, • View key assignments in View > Assigned Keys.To print or copy exporting, and printing labels for bibliographic records; using local files; the list, click Print or Copy to Clipboard. creating and adding records to WorldCat; replacing WorldCat records; Tip: Before printing, click a column heading to sort the list by data batch processing; and cataloging with non-Latin scripts. in the column. • Assign your own keystrokes in Tools > Keymaps. Multiscript support: The client supports the following non-Latin scripts: • Print a function key template to put at the top of your keyboard: Arabic, Armenian, Bengali, Chinese, Cyrillic, Devanagari, Ethiopic, Greek, Hebrew, Japanese, Korean, Syriac, Tamil, and Thai. www.oclc.org/support/documentation/connexion/client/ gettingstarted/keyboardtemplate.pdf. This quick reference does not cover instructions for authorities work or instructions already available in: Toolbar • Getting Started with Connexion Client • The client installs with three toolbars displayed by default: • Connexion Client Setup Worksheet o Main client toolbar (with command-equivalent buttons) • Connexion: Searching WorldCat Quick Reference o WorldCat quick search tool Quick tools for text strings and user tools Connexion client documentation assumes knowledge of MARC o cataloging. • Customize the main client toolbar: In Tools > Toolbar Editor, drag and drop buttons to add or remove, or reset to the default. -
ANNUAL REPORT Financial Statements
ANNUAL REPORT Financial Statements 2005 – 2006 Torino 2006 Paralympic Games Contents Officers and Officials …………..3 Chairman’s Report …………..4 Chief Executive Report …………..4 PNZ Board .…………..5 PNZ Staff & Service Providers .…………..6 SPARC .…………..7 International Paralympic Committee .…………..7 Sponsors & Supporters .…………..8 High Performance Report ………….9 Lion Foundation Paralympic Academy .………….9 Sports Science Report .………….10 Athletes Report ………….10 International Teams and Results ………….12 PA/NZAS Carded Athletes ………….19 PNZ / NZAS Sport Liaison .………….19 Operations Report ………… 19 Key Relationships ……….….19 Events ……….….20 PNZ National Championships ……….….20 Beijing 2008 Planning / IT .………….20 Classification Report ………….21 Classifiers ….……….23 New Year Honours ..………..24 Obituary’s ..………..24 Financial Statements …………..F Statement of Financial Performance .……….…F1 Statement of Financial Position .……….…F2 Notes to the Accounts .……….…F3 Auditors Report ……….….F7 New Zealand Paralympians …………25 Strategic Plan 05-09 …………28 Sponsors and Partners …………29 2 Officers and Officials Patron Mr. Paul Holmes, NZOM Board Mr. Simon Peterson (Chair) Ms. Sandra Blewett, MBE Mr. Ross Darrah Mr. Marc Frewin (co-opted June 06) Mrs. Gillian Hall Mr. Duane Kale Mr. David Rutherford Athletes Representative Mr. Tim Prendergast & Mr. Matt Slade Honorary Solicitor Mr. John Wiltshire, LLB Auditors Hayes Knight & Co Bankers ASB Bank Ltd, Remuera, Auckland Support Office Staff Chief Executive Officer Mr. Craig Hobbs High Performance Manager Ms. Helen Murphy Operations Manager Mr. Vaughan Cruickshank (to Feb 06) Ms. Fiona Allan (from May 06) Administration Mrs. Val Hall Operations Officer Mr. Wade Chang Medical Director Dr. Paul Wharam, BM, DRCOG, FRNZGP, Dip Sports Med. Sports Science Coordinator University of Canterbury; Mr Malcolm Humm Classification Coordinator Mrs. Rebecca Foulsham (to June 06) Mrs. -

Effects of Prosthetic Foot Forefoot Flexibility on Oxygen Cost and Subjective Preference Rankings of Unilateral Transtibial Prosthesis Users
Volume 47, Number 6, 2010 JRRDJRRD Pages 543–552 Journal of Rehabilitation Research & Development Effects of prosthetic foot forefoot flexibility on oxygen cost and subjective preference rankings of unilateral transtibial prosthesis users Elizabeth Klodd, MS;1 Andrew Hansen, PhD;2–3* Stefania Fatone, PhD;3–4 Mark Edwards, MHPE, CP4–5 1Liberating Technologies Incorporated, Holliston, MA; 2Minneapolis Department of Veterans Affairs Medical Center, Minneapolis, MN; 3Northwestern University Prosthetics Research Laboratory & Rehabilitation Engineering Research Program; Department of Physical Medicine & Rehabilitation, Feinberg School of Medicine, Northwestern University, Chicago, IL; 4Northwestern University Prosthetics-Orthotics Center; Feinberg School of Medicine, Northwestern University, Chicago, IL; 5Otto Bock HealthCare, Minneapolis, MN Abstract—The invest igators con ducted a dou ble-blind ran - INTRODUCTION domized crossover study to determine the effects of prosthetic foot forefoot flexibility on oxygen cost and subjective prefer- Lower-limb prosthesis users exp end more ox ygen ence rankings of 13 unilateral transtibial prosthesis users. Five per unit distance (oxygen cost) during walking than non- experimental feet were fabricated for use in the study: F1, F2, disabled participants [1]. En ergy cost and expe nditure F3, F4, and F5. F1 was most flexible, F5 was least flexible, and also correlate with level of amputation [2] and residua l F3 was designed to conform to a biomimetic ankle-foot roll- limb lengt h [3] and have mo re recently been used in over shape. The experimental feet were modeled after the attempts to quantify differences between prosthetic feet Shape&Roll prosth etic foot (o riginally p roduced b y No rth- within a popula tion of prosthesis users. -
![F6-13 202 (Ibc [F] 202)](https://docslib.b-cdn.net/cover/4091/f6-13-202-ibc-f-202-1014091.webp)
F6-13 202 (Ibc [F] 202)
F6-13 202 (IBC [F] 202) Proposed Change as Submitted Proponent: Elley Klausbruckner representing Klausbruckner & Associates Inc ([email protected]) Revise as follows: SECTION 202 (IBC [F] 202) GENERAL DEFINITIONS FLAMMABLE SOLID. A solid, other than a blasting agent or explosive, that is capable of causing fire through friction, absorption of moisture, spontaneous chemical change or retained heat from manufacturing or processing, or which has an ignition temperature below 212°F (100°C) or which burns so vigorously and persistently when ignited as to create a serious hazard. A chemical shall be considered a flammable solid as determined in accordance with the test method of CPSC 16 CFR Part 1500.44, if it ignites and burns with a self-sustained flame at a rate greater than 0.1 0.0866 inch (2.5 mm 2.2 mm) per second along its major axis. Reason: The definition proposed is in line with GHS [Globally Harmonized System] which is now adopted by OSHA. When an MSDS is prepared today, a material classified as “Flammable Solids” is typically based on this definition and not the previous definition [existing language in the Fire Code]. For additional details please see http://www.osha.gov/dsg/hazcom/ghs.html. Cost Impact: The code change proposal will not increase the cost of construction. 202-FLAMMABLE SOLID-F-KLAUSBRUCKNER Committee Action Hearing Results Committee Action: Disapproved Committee Reason: The disapproval was based on the committee’s judgment that the code change could be the beginning of a trend toward acceptance of OSHA definitions which are much different than IFC definitions and are focused on worker and work- place safety only. -
Maximal Fully-Tethered Swim Performance in Para Swimmers with Physical Impairment
Hogarth, Luke and Burkett, Brendan and van de Vliet, Peter and Payton, Carl (2020) Maximal fully-tethered swim performance in Para swimmers with physical impairment. International Journal of Sports Physiology and Perfor- mance, 15 (6). ISSN 1555-0273 Downloaded from: https://e-space.mmu.ac.uk/624727/ Version: Accepted Version Publisher: Human Kinetics DOI: https://doi.org/10.1123/ijspp.2019-0515 Please cite the published version https://e-space.mmu.ac.uk Maximal fully-tethered swim performance in Para swimmers with physical impairment Luke Hogarth1, Brendan Burkett1, Peter Van de Vliet2 and Carl Payton3 1 School of Health and Sport Sciences, University of the Sunshine Coast, Australia. 2 Medical and Scientific Department, International Paralympic Committee, Germany. 3 Musculoskeletal Science & Sports Medicine Research Centre, Manchester Metropolitan University, United Kingdom. Corresponding author: Luke Hogarth ([email protected]) School of Health and Sport Sciences University of the Sunshine Coast Australia Text-only word count: 4077 Abstract word count: 249 Number of figures and tables: 4 Number of references: 25 1 Maximal fully-tethered swim performance in Para swimmers with physical impairment Abstract Purpose: The assessment of swimming propulsion should be a cornerstone of Paralympic swimming classification. However, current methods do not objectively account for this component. This study evaluated the swimming propulsion of swimmers with and without physical impairment using a 30 s maximal fully-tethered freestyle swim test. Methods: Tethered forces were recorded during maximal fully-tethered swimming in eighty competitive swimmers with (n = 70) and without (n = 10) physical impairment. The relationships between absolute and normalised tether forces and maximal freestyle swim speed were established using general additive models. -

The ICD-10 Classification of Mental and Behavioural Disorders Diagnostic Criteria for Research
The ICD-10 Classification of Mental and Behavioural Disorders Diagnostic criteria for research World Health Organization Geneva The World Health Organization is a specialized agency of the United Nations with primary responsibility for international health matters and public health. Through this organization, which was created in 1948, the health professions of some 180 countries exchange their knowledge and experience with the aim of making possible the attainment by all citizens of the world by the year 2000 of a level of health that will permit them to lead a socially and economically productive life. By means of direct technical cooperation with its Member States, and by stimulating such cooperation among them, WHO promotes the development of comprehensive health services, the prevention and control of diseases, the improvement of environmental conditions, the development of human resources for health, the coordination and development of biomedical and health services research, and the planning and implementation of health programmes. These broad fields of endeavour encompass a wide variety of activities, such as developing systems of primary health care that reach the whole population of Member countries; promoting the health of mothers and children; combating malnutrition; controlling malaria and other communicable diseases including tuberculosis and leprosy; coordinating the global strategy for the prevention and control of AIDS; having achieved the eradication of smallpox, promoting mass immunization against a number of other -

Spinal Fractures Classification System an Aospine Knowledge Forum Initiative
Spinal Fractures Classification System an AOSpine Knowledge Forum initiative Subaxial Spine Fractures Thoracolumbar Spine Fractures Sacral Spine Fractures AOSpine–the leading global academic community for innovative education and research in spine care, inspiring lifelong learning and improving patients’ lives. Spinal Fractures Classification System 2 Spinal Fractures Classification System an AOSpine Knowledge Forum initiative CONTENT AOSpine Classification and Injury Severity System ................ 04 for Traumatic Fractures of the Subaxial Spine AOSpine Classification and Injury Severity System ................. 37 for Traumatic Fractures of the Thoracolumbar Spine AOSpine Classification and Injury Severity System .................55 for Traumatic Fractures of the Sacral Spine Spinal Fractures Classification System 3 AOSpine Knowledge Forum AOSpine Classification and Injury Severity System for Traumatic Fractures of the Subaxial Spine This is the present form of the classification the AOSpine Knowledge Forum (KF) SCI & Trauma is working on. It is the aim of the KF to develop a system, which can in the future be used as a tool for scientific research and a guide for treatment. This system is being subjected to a rigorous scientific assessment. Project members Aarabi B, Bellabarba C, Chapman J, Dvorak M, Fehlings M, Kandziora F, Kepler C, (in alphabetic order) Oner C, Rajasekaran S, Reinhold M, Schnake K, Vialle L and Vaccaro A. Disclaimer 1. Vaccaro, A. R., J. D. Koerner, K. E. Radcliff, F. C. Oner, M. Reinhold, K. J. Schnake, F. Kandziora, M. G. Fehlings, M. F. Dvorak, B. Aarabi, S. Rajasekaran, G. D. Schroeder, C. K. Kepler and L. R. Vialle (2015). “AOSpine subaxial cervical spine injury classification system.” Eur Spine J. 2. International validation process to be completed in 2015.