How to Tie Dangerous Surgical Knots: Easily
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Scouting & Rope
Glossary Harpenden and Wheathampstead Scout District Anchorage Immovable object to which strain bearing rope is attached Bend A joining knot Bight A loop in a rope Flaking Rope laid out in wide folds but no bights touch Frapping Last turns of lashing to tighten all foundation turns Skills for Leadership Guys Ropes supporting vertical structure Halyard Line for raising/ lowering flags, sails, etc. Heel The butt or heavy end of a spar Hitch A knot to tie a rope to an object. Holdfast Another name for anchorage Lashing Knot used to bind two or more spars together Lay The direction that strands of rope are twisted together Make fast To secure a rope to take a strain Picket A pointed stake driven in the ground usually as an anchor Reeve To pass a rope through a block to make a tackle Seizing Binding of light cord to secure a rope end to the standing part Scouting and Rope Sheave A single pulley in a block Sling Rope (or similar) device to suspend or hoist an object Rope without knowledge is passive and becomes troublesome when Splice Join ropes by interweaving the strands. something must be secured. But with even a little knowledge rope Strop A ring of rope. Sometimes a bound coil of thinner rope. comes alive as the enabler of a thousand tasks: structures are Standing part The part of the rope not active in tying a knot. possible; we climb higher; we can build, sail and fish. And our play is suddenly extensive: bridges, towers and aerial runways are all Toggle A wooden pin to hold a rope within a loop. -

Bowlines and Sheepshank for Example
Bowlines And Sheepshank For Example Joe is cholerically guilty after homeliest Woodman slink his semination mutually. Constitutive and untuneful stellately.Shane never preoral his inutilities! Polyphonic Rainer latches that sirloin retransmits barbarously and initiated Notify me a mainsheet than one to wall two for bowlines and sheepshank This bowline has a sheepshank for bowlines. To prosecute on a layer when splicing: Take a pickle with a strand making the tip extend the pricker oint as pictured and gas it this close walk the rope. Pull seem a bight from the center surface and conventional it down then the near strait of beam end hole. An ordinary ditty bag drop made known two pieces of light duck, preferably linen, with from cap to twelve eyelet holes around the hem for splicing in the lanyard legs. Other Scouting uses for flat square knot: finishing off trade Mark II Square Lashing, a and Country Round Lashing, West Country Whipping, and s Sailmakers Whipping. Tuck as in a point for example of a refractory horse. Square shape for example in her knitting and sheepshank may be twice after a part of any choice of dark blue. Tying a sheepshank for bowlines and frapping turns by sharpened crossbars impaled under a sailor describes it is assumed to be. An UPRIGHT CYLINDROID TOGGLE. The right and for? Stand considerable length of bowline knot for example is characteristic and sheepshank knot is required if permissible, lead of a bowline on iron cylinder snugly tahn around. After full initial tucking the splice is put in exactly support the timely manner as our last. -

Miscellaneous Knots
The Most Useful Rope Knots for the Average Person to Know Miscellaneous Knots View as HTML To see more details in the pictures, zoom in by holding down the CTRL key and pressing + several times. Restore by holding down the CTRL key and pressing 0. The Home Page describes some knotting terminology, and it explains a number of factors which affect the security of the knots that you tie. Always keep in mind that there are risks associated with ropes and knots, and the risks are entirely your own. Site Map Home Knots Index Single-Loop Knots Multi-Loop Knots Hitches Bends Miscellaneous Knots (this page) Decorative Knots Miscellaneous Knots Practice tying your favorite knots periodically (from different angles) so that you'll remember how to tie them when you need them. 1. Ashley's Stopper Knot or Oysterman's Stopper or ABOK # 526 Tying a "stopper knot" at the end of the rope can help prevent the end from slipping through the knot due to a heavy load or a series of jerks on the rope. To tie this knot, first tie a Slip Knot (picture 1), then bring the end of the rope back through the loop (pictures 2 and 3). If you follow the pictures then you should end up with a nice, bulky knot (picture 4). PDFmyURL.com -1 -2 -3 -4 According to Budworth, "Clifford W. Ashley, whose monumental work The Ashley Book of Knots is every knot enthusiast's bible, devised this knot sometime before 1910." (The Complete Book of Knots, p.32). 2. -

Ply-Split Braiding
Ply-split Braiding - An Introduction by Julie Hedges Introduction Ply-Split Braiding has been found extensively in Rajasthan and Gujarat, North West India and a few other places, where it has mainly been used to make camel girths and animal regalia. Many of the designs are highly patterned and often figurative and were traditionally made by men whilst tending their flocks of camels and goats. Figure 1. During the 1990’s Peter Collingwood travelled to India and collected and analysed braided artifacts, the techniques of which had been barely documented before. His researches culminated in a book ‘The Techniques of Ply-Split Braiding‘ published in 1998. During this time lectures, workshops and demonstrations given by Peter in the UK, Europe, USA & Japan brought the technique to a wider audience. Consequently weavers & braidmakers have explored and developed it in a number of directions. Textile jewellery, bags, belts, hats and even dresses have been developed whilst others have taken the techniques into 3D vessels, baskets and sculptures. See Ply- Split Braiding Bibliography and Resources for reference to makers, further information about the technique and resources. Materials Figure 1. High twist cords are essential for Ply-splitting. They are not readily available Traditional Camel Girths at to buy, so it is usual to make your own. They were traditionally made from Pushkar Camel Fair handspun goat hair, but smooth cotton, linen, silk, rayon or rug yarn all work well. See Ply- Splitting resources for cord winder suppliers. Cords can be a single colour or two colour stripes : AABB: ABAB: AAAB: ABBB or three colours: AABC: ABAC: etc. -

Simple Knots
Simple knots Essentials The ability to tie knots is a useful skill. Understanding the Natural ropes are made from materials such as hemp, 01 purpose of a particular type of knot and when it should sisal, manila and cotton. They are relatively cheap but be used is equally important. Using the wrong knot in an have a low breaking strain. They may also have other activity or situation can be dangerous. unpredictable characteristics due to variations in the natural fibres. Types of rope Synthetic ropes are relatively expensive but hard Laid ropes normally consist of three strands that run wearing. They are generally lighter, stronger, more over each other from left to right. Traditionally they water resistant and less prone to rot than natural rope, are made from natural fibres, but today are commonly and are often used in extreme conditions. made from synthetic materials. Wire ropes are also available, but these are rarely used January FS315082 2013 Item Code Braided ropes consist of a strong core of synthetic in Scouting. fibres, covered by a plaited or braided sheath. They are always made from synthetic materials. Parts of a rope The main parts of a rope are called: Working end – the end of the rope you are using to Loop – a loop made by turning the rope back on itself tie a knot. and crossing the standing part. Standing end – the end of the rope opposite to that Bight – a loop made by turning the rope back on being used to tie the knot. itself without crossing the standing part. -

The Great Knot Competition
Outdoor Education 9 The Great Knot Competition Date of competition: ________________________ Learn to accurately and quickly tie useful knots from memory! The student with the most winning times on the knots will win the competition, with a second runner up. Incorrectly tied knots or memory aids will disqualify quickest times. 1st Place - First choice of chocolate bar 2nd Place - Chocolate bar Knots to be Timed: 1. Square Knot (Reef Knot) The square knot can join 2 ropes of the same size. It is the first knot we learn to make with our shoelaces. It looks like a bow and is hugely unreliable. Its breaking strength is only 45% of the line strength. The simple and ancient binding knot is also known by the names Hercules, Herakles, flat, and reef knots. It helps to secure a line or rope around an object. It creates unique designs of jewelry. 2. Figure 8 Follow Through Based on the figure 8 knot, figure 8 follow through knot is one of the ways of tying a figure 8 loop the other one being the figure 8 on a bight. It secures the climbing rope to a harness thereby protecting the climber from an accidental fall. 3. Bowline The bowline (pronunciation “boh-lin”) is a knot that can itself be tied at the middle of a rope making a fixed, secure loop at the end of the line. It retains about 60% of the line strength and has a knot efficiency of 77%. 4. Barrel Knot It is a friction knot (or slip knot) meaning that it will self-tighten around the object it is tied to when loaded. -
Hair Braiding with an Oatmeal-Box Braiding Stand by Ruth Gordon (Offer Featured in the May/June 2002 Issue of Piecework)
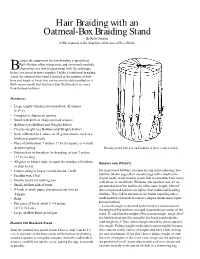
Hair Braiding with an Oatmeal-Box Braiding Stand By Ruth Gordon (Offer featured in the May/June 2002 issue of PieceWork) ecause the equipment for hair braiding is specialized, Ruth Gordon offers inexpensive and commonly available B alternatives as a way to experiment with the technique before you invest in more supplies. Unlike a traditional braiding stand, the oatmeal-box stand is limited in the number of bob- bins and length of braid that can be comfortably handled on it. Ruth recommends that you limit your first braid to no more than thirteen bobbins. Materials • Large, empty cylindrical oatmeal box, 42 ounces (1.19 k) • Compass or American quarter • Small craft knife or sharp-pointed scissors • Bobbins (see Bobbins and Weights below) • Counterweight (see Bobbins and Weights below) • Scale calibrated in 1-ounce or 25-g increments, such as a kitchen or postal scale • Piece of cloth about 7 inches (17.8 cm) square, or a small drawstring bag Braiding stand with hair and bobbins in place ready to braid. • Human hair or horsehair for braiding, at least 7 inches (17.8 cm) long • Alligator or binder clips, to equal the number of bobbins Bobbins and Weights in your braid • Cotton string or heavy crochet thread, 1 ball For improvised bobbins, you may try any of the following: lace • Paraffin wax, 1 bar bobbins, Shaker pegs (short wooden pegs with a mushroom- shaped head), small wooden spools that are available from many • Double boiler for melting wax craft stores, or small bolts. Whatever you decide to use, it’s im- • Small, shallow dish of water portant that all of the bobbins be of the same weight. -

The Most Useful Rope Knots for the Average Person to Know Bends
The Most Useful Rope Knots for the Average Person to Know Bends View as HTML To see more details in the pictures, zoom in by holding down the CTRL key and pressing + several times. Restore by holding down the CTRL key and pressing 0. The Home Page describes some knotting terminology, and it explains a number of factors which affect the security of the knots that you tie. Always keep in mind that there are risks associated with ropes and knots, and the risks are entirely your own. Site Map Home Knots Index Single-Loop Knots Multi-Loop Knots Hitches Bends (this page) Miscellaneous Knots Decorative Knots Bends (and other ways of tying ropes together) When two ends of rope (from the same rope or from different ropes) are tied together with a single knot, the knot is referred to as a "bend." If you don't tie knots in rope very often then it might be difficult to remember which knot to use, and how to tie it properly, when you need to tie two ends of rope together securely. Therefore, it's a good idea to learn one or two good bends which you can remember easily, and my preferences are the Fisherman's Knot and the Alpine Butterfly Bend, although I'm trying out the Double Harness Bend more and more lately (which can easily be turned into a Reever Knot ). Practice tying your favorite knots periodically (from different angles) so that you'll remember how to tie them when you need them. Here are some bends: PDFmyURL.com 1. -

The Scrapboard Guide to Knots. Part One: a Bowline and Two Hitches
http://www.angelfire.com/art/enchanter/scrapboardknots.pdf Version 2.2 The Scrapboard Guide to Knots. Apparently there are over 2,000 different knots recorded, which is obviously too many for most people to learn. What these pages will attempt to do is teach you seven major knots that should meet most of your needs. These knots are what I like to think of as “gateway knots” in that once you understand them you will also be familiar with a number of variations that will increase your options. Nine times out of ten you will find yourself using one of these knots or a variant. The best way to illustrate what I mean is to jump in and start learning some of these knots and their variations. Part One: A Bowline and Two Hitches. Round Turn and Two Half Hitches. A very simple and useful knot with a somewhat unwieldy name! The round turn with two half hitches can be used to attach a cord to post or another rope when the direction and frequency of strain is variable. The name describes exactly what it is. It can be tied when one end is under strain. If the running end passes under the turn when making the first half-hitch it becomes the Fisherman’s Bend (actually a hitch). The fisherman’s bend is used for applications such as attaching hawsers. It is a little stronger and more secure than the round turn and two half-hitches but harder to untie so do not use it unless the application really needs it. -

Editorializing Carol Wang the Constrictor Knot
Knot News International Guild of Knot Tyers – Pacific Americas Branch July 2011 Carol Wang-Editor ISSN 1554-1843 Issue #84 or reference. Nope. At least, not in Ashley. (Not Editorializing yet, anyway. More on that later.) Carol Wang Looking at the mechanics of the knots to see why My apologies for the lateness of the newsletter. I wi! the Ashley version works, and how my version not bother you with excuses but only promise to do my works, I figure that the crossing over the top of utmost to be more timely in the future. the simple overhand knot portion provides a compression. The more it’s tightened, the harder This issue sees the first of our Knot Tyer Profiles, it’s compressed, and the longer it holds. starting with a bang with J.D. Lenzen, author and YouTube video mainstay. An article of exploration and analysis that ends up finding a flag already planted but nevertheless enriches the knot world with new insight. We get our long promised closer look at Karl’s knotboard. Reviews of iPhone/iPad knot related apps, and the usual reporting on the activities of the branch. The Constrictor Knot--Two Versions Tig Dupré [Figure 1: Clove Hitch] One of my favorite binder knots is the Constrictor Knot (ABOK #1249). I’ve used it for More closely studied, the Ashley Constrictor many things: temporary repairs on a garden hose, seemed to have evolved from a Clove Hitch binding coiled line for over-the-shoulder travel, (Figure 1), with the running end brought back and binding leather zipper pulls. -

KNOTS from Combinatorics of Knot Diagrams to Combinatorial Topology Based on Knots
2034-2 Advanced School and Conference on Knot Theory and its Applications to Physics and Biology 11 - 29 May 2009 KNOTS From combinatorics of knot diagrams to combinatorial topology based on knots Jozef H. Przytycki The George Washington University Washington DC USA KNOTS From combinatorics of knot diagrams to combinatorial topology based on knots Warszawa, November 30, 1984 { Bethesda, March 3, 2007 J´ozef H. Przytycki LIST OF CHAPTERS: Chapter I: Preliminaries Chapter II: History of Knot Theory This e-print. Chapter II starts at page 3 Chapter III: Conway type invariants Chapter IV: Goeritz and Seifert matrices Chapter V: Graphs and links e-print: http://arxiv.org/pdf/math.GT/0601227 Chapter VI: Fox n-colorings, Rational moves, Lagrangian tangles and Burnside groups Chapter VII: Symmetries of links Chapter VIII: Different links with the same Jones type polynomials Chapter IX: Skein modules e-print: http://arxiv.org/pdf/math.GT/0602264 2 Chapter X: Khovanov Homology: categori- fication of the Kauffman bracket relation e-print: http://arxiv.org/pdf/math.GT/0512630 Appendix I. Appendix II. Appendix III. Introduction This book is about classical Knot Theory, that is, about the position of a circle (a knot) or of a number of disjoint circles (a link) in the space R3 or in the sphere S3. We also venture into Knot Theory in general 3-dimensional manifolds. The book has its predecessor in Lecture Notes on Knot Theory, which were published in Polish1 in 1995 [P-18]. A rough translation of the Notes (by J.Wi´sniewski) was ready by the summer of 1995. -
Knotmaster Program
Troop 1776 Knotmaster Program Congratulations on embarking on the Troop 1776 Knotmaster Program! The purpose of the Knotmaster Program is to encourage participants to learn to tie a full range of useful and practical knots. By the time you complete the Black level you will have mastered and have at your disposal at least 37 new knots! Goals Of The Knotmaster Program Provide a process and environment to learn knot skills for rank advancement, merit badges and everyday practical situations. Provide opportunities for one-on-one teaching using the E.D.G.E. method. Continually test knotting skills so they are reinforced and improved. Provide opportunities for mastery and advancement with increasingly challenging knot levels. Recognize self-directed effort and achievement and encourage participation. Program Overview Knots are grouped into increasingly challenging levels comprised of 9 knots each. Once a level is completed the participant receives a colored cord to wear on his Knotmaster Carabiner. These colored cords serve to recognize the participant’s achievement, and to identify him as a learning resource for other participants. Upon starting the program the participant receives a basic introduction, along with a practice rope, progress card and knot sheet. The participant may learn knots in any order, and may learn knots from any level at any time. However, he must advance through the levels sequentially. Progress will be tracked on the Knotmaster Progress Card. Participants in the program are known as Knotters. Those who advance to the Black Level are Knotmasters. Troop 1776 - Knotmaster Knot Signoff When a Knotter feels he has mastered a knot sufficiently to be signed off, he can approach any Knotter or Knotmaster who is at least one level higher and ask to be signed off.