Biological Responses to Metal Implants
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Presence of ROS in Inflammatory Environment of Peri-Implantitis Tissue
Journal of Clinical Medicine Article Presence of ROS in Inflammatory Environment of Peri-Implantitis Tissue: In Vitro and In Vivo Human Evidence 1, 2, 2, 3 4 Eitan Mijiritsky y, Letizia Ferroni y, Chiara Gardin y, Oren Peleg , Alper Gultekin , Alper Saglanmak 4, Lucia Gemma Delogu 5, Dinko Mitrecic 6, Adriano Piattelli 7, 8, 2,9, , Marco Tatullo z and Barbara Zavan * z 1 Head and Neck Maxillofacial Surgery, Department of Otoryngology, Tel-Aviv Sourasky Medical Center, Sackler Faculty of Medicine, Tel-Aviv University, Weizmann street 6, 6423906 Tel-Aviv, Israel; [email protected] 2 Maria Cecilia Hospital, GVM Care & Research, Cotignola, 48033 Ravenna, Italy; [email protected] (L.F.); [email protected] (C.G.) 3 Department of Otolaryngology Head and Neck Surgery and Maxillofacial Surgery, Tel-Aviv Sourasky Medical Center, Sackler School of Medicine, Tel Aviv University, 701990 Tel-Aviv, Israel; [email protected] 4 Istanbul University, Faculty of Dentistry, Department of Oral Implantology, 34093 Istanbul, Turkey; [email protected] (A.G.); [email protected] (A.S.) 5 University of Padova, DpT Biomedical Sciences, 35133 Padova, Italy; [email protected] 6 School of Medicine, Croatian Institute for Brain Research, University of Zagreb, Šalata 12, 10 000 Zagreb, Croatia; [email protected] 7 Department of Medical, Oral, and Biotechnological Sciences, University of Chieti-Pescara, via dei Vestini 31, 66100 Chieti, Italy; [email protected] 8 Marrelli Health-Tecnologica Research Institute, Biomedical Section, Street E. Fermi, 88900 Crotone, Italy; [email protected] 9 Department of Medical Sciences, University of Ferrara, via Fossato di Mortara 70, 44123 Ferara, Italy * Correspondence: [email protected] Co-first author. -
Overview of Biomaterials and Their Use in Medical Devices
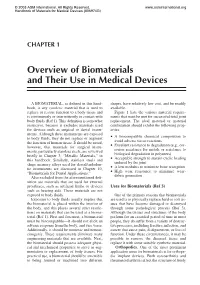
© 2003 ASM International. All Rights Reserved. www.asminternational.org Handbook of Materials for Medical Devices (#06974G) CHAPTER 1 Overview of Biomaterials and Their Use in Medical Devices A BIOMATERIAL, as defined in this hand- shapes, have relatively low cost, and be readily book, is any synthetic material that is used to available. replace or restore function to a body tissue and Figure 1 lists the various material require- is continuously or intermittently in contact with ments that must be met for successful total joint body fluids (Ref 1). This definition is somewhat replacement. The ideal material or material restrictive, because it excludes materials used combination should exhibit the following prop- for devices such as surgical or dental instru- erties: ments. Although these instruments are exposed A biocompatible chemical composition to to body fluids, they do not replace or augment • avoid adverse tissue reactions the function of human tissue. It should be noted, Excellent resistance to degradation (e.g., cor- however, that materials for surgical instru- • rosion resistance for metals or resistance to ments, particularly stainless steels, are reviewed biological degradation in polymers) briefly in Chapter 3, “Metallic Materials,” in Acceptable strength to sustain cyclic loading this handbook. Similarly, stainless steels and • endured by the joint shape memory alloys used for dental/endodon- A low modulus to minimize bone resorption tic instruments are discussed in Chapter 10, • High wear resistance to minimize wear- “Biomaterials for Dental Applications.” • debris generation Also excluded from the aforementioned defi- nition are materials that are used for external prostheses, such as artificial limbs or devices Uses for Biomaterials (Ref 3) such as hearing aids. -

CASODEX (Bicalutamide)
HIGHLIGHTS OF PRESCRIBING INFORMATION • Gynecomastia and breast pain have been reported during treatment with These highlights do not include all the information needed to use CASODEX 150 mg when used as a single agent. (5.3) CASODEX® safely and effectively. See full prescribing information for • CASODEX is used in combination with an LHRH agonist. LHRH CASODEX. agonists have been shown to cause a reduction in glucose tolerance in CASODEX® (bicalutamide) tablet, for oral use males. Consideration should be given to monitoring blood glucose in Initial U.S. Approval: 1995 patients receiving CASODEX in combination with LHRH agonists. (5.4) -------------------------- RECENT MAJOR CHANGES -------------------------- • Monitoring Prostate Specific Antigen (PSA) is recommended. Evaluate Warnings and Precautions (5.2) 10/2017 for clinical progression if PSA increases. (5.5) --------------------------- INDICATIONS AND USAGE -------------------------- ------------------------------ ADVERSE REACTIONS ----------------------------- • CASODEX 50 mg is an androgen receptor inhibitor indicated for use in Adverse reactions that occurred in more than 10% of patients receiving combination therapy with a luteinizing hormone-releasing hormone CASODEX plus an LHRH-A were: hot flashes, pain (including general, back, (LHRH) analog for the treatment of Stage D2 metastatic carcinoma of pelvic and abdominal), asthenia, constipation, infection, nausea, peripheral the prostate. (1) edema, dyspnea, diarrhea, hematuria, nocturia, and anemia. (6.1) • CASODEX 150 mg daily is not approved for use alone or with other treatments. (1) To report SUSPECTED ADVERSE REACTIONS, contact AstraZeneca Pharmaceuticals LP at 1-800-236-9933 or FDA at 1-800-FDA-1088 or ---------------------- DOSAGE AND ADMINISTRATION ---------------------- www.fda.gov/medwatch The recommended dose for CASODEX therapy in combination with an LHRH analog is one 50 mg tablet once daily (morning or evening). -

The Journal of the International Federation of Clinical Chemistry and Laboratory Medicine in This Issue
June 2021 ISSN 1650-3414 Volume 32 Number 2 Communications and Publications Division (CPD) of the IFCC Editor-in-chief: Prof. János Kappelmayer, MD, PhD Faculty of Medicine, University of Debrecen, Hungary e-mail: [email protected] The Journal of the International Federation of Clinical Chemistry and Laboratory Medicine In this issue Introducing the eJIFCC special issue on “POCT – making the point” Guest editor: Sergio Bernardini 116 Controlling reliability, interoperability and security of mobile health solutions Damien Gruson 118 Best laboratory practices regarding POCT in different settings (hospital and outside the hospital) Adil I. Khan 124 POCT accreditation ISO 15189 and ISO 22870: making the point Paloma Oliver, Pilar Fernandez-Calle, Antonio Buno 131 Utilizing point-of-care testing to optimize patient care James H. Nichols 140 POCT: an inherently ideal tool in pediatric laboratory medicine Siobhan Wilson, Mary Kathryn Bohn, Khosrow Adeli 145 Point of care testing of serum electrolytes and lactate in sick children Aashima Dabas, Shipra Agrawal, Vernika Tyagi, Shikha Sharma, Vandana Rastogi, Urmila Jhamb, Pradeep Kumar Dabla 158 Training and competency strategies for point-of-care testing Sedef Yenice 167 Leading POCT networks: operating POCT programs across multiple sites involving vast geographical areas and rural communities Edward W. Randell, Vinita Thakur 179 Connectivity strategies in managing a POCT service Rajiv Erasmus, Sumedha Sahni, Rania El-Sharkawy 190 POCT in developing countries Prasenjit Mitra, Praveen Sharma 195 In this issue How could POCT be a useful tool for migrant and refugee health? Sergio Bernardini, Massimo Pieri, Marco Ciotti 200 Direct to consumer laboratory testing (DTCT) – opportunities and concerns Matthias Orth 209 Clinical assessment of the DiaSorin LIAISON SARS-CoV-2 Ag chemiluminescence immunoassay Gian Luca Salvagno, Gianluca Gianfilippi, Giacomo Fiorio, Laura Pighi, Simone De Nitto, Brandon M. -

Metallosis and Pseudotumor Around Ceramic-On-Polyethylene Total Hip Arthroplasty; Case Report and Literature Review
Available online at www.ijmrhs.com Special Issue 9S: Medical Science and Healthcare: Current Scenario and Future Development International Journal of Medical Research & ISSN No: 2319-5886 Health Sciences, 2016, 5, 9S:518-524 Metallosis and Pseudotumor around Ceramic-On-Polyethylene Total Hip Arthroplasty; Case Report and Literature Review Afshin Taheriazam 1* and Amin Saeidinia 2,3 1Hip Surgeon, Assistant Professor, Department of Orthopedics Surgery, Tehran Medical Sciences Branch, Islamic Azad University, Tehran, Iran 2General Practitioner, Assistant Researcher, Mashhad University of Medical Sciences, Mashhad, Iran 3Member of Young Researchers Club, Rasht Branch, Islamic Azad University, Rasht, Iran *Corresponding Email: [email protected] _____________________________________________________________________________________________ ABSTRACT Polyethylene failure is a rare complication of ceramic-on-polyethylene total hip arthroplasty due to characteristics of ceramic. Complications associated with ceramic-on-polyethylene articulations have been studied extensively, however, only few reports have described its catastrophic wear and concurrent pseudotumor formation. The etiology of this biological reaction and concurrency of pseudotumor formation with metallosis remain unclear. We report two cases of wear of the acetabular liner in a ceramic-on-polyethylene prosthesis due to total hip arthroplasty (THA) long time ago. They came back to the clinic with the history of worsening hip pain and abnormal radiological and clinical findings. Then they underwent surgery and metallosis and pseudotumors were detected and revisions were performed for them. It is necessary to evaluate patients underwent THA complaining of hip pain for component wear and be checked the cup appear well fixing and fairly oriented on follow-up radiographies. Close follow ups can prevent accelerated polyethylene wear in ceramic-on-polyethylene coupling THA. -

A Mini-Review of Dental Implant Biomaterials
Mini Review Modifying an Implant: A Mini-review of Dental Implant Biomaterials Oliver K. Semisch-Dieter1, Andy H. Choi1, Besim Ben-Nissan1 and Martin P. Stewart1,* Abstract 1School of Life Sciences, Faculty of Science, University Dental implants have been used as far back as 2000BC, and since then have developed into highly sophisti- of Technology Sydney, Ultimo, cated solutions for tooth replacement. It is becoming increasingly important for the materials used in dental implants to exhibit and maintain favorable long-term mechanical, biological and more recently, aesthetic NSW, Australia properties. This review aims to assess the biomaterials used in modern dental implants, introducing their properties, and concentrating on modifications to improve these biomaterials. Focus is drawn to the promi- nent biomaterials, titanium (Ti) and zirconia due to their prevalence in implant dentistry. Additionally, novel coatings and materials with potential use as viable improvements or alternatives are reviewed. An effective *Correspondence to: dental biomaterial should osseointegrate, maintain structural integrity, resist corrosion and infection, and not Martin P. Stewart cause systemic toxicity or cytotoxicity. Current materials such as bioactive glass offer protection against bio- E-mail: martin.stewart@uts. film formation, and when combined with a titanium–zirconium (TiZr) alloy, provide a reliable combination edu.au of properties to represent a competitive alternative. Further long-term clinical studies are needed to inform the development of next-generation materials. Received: September 7 2020 Revised: December 7 2020 Keywords Accepted: January 4 2021 Biocompatibility, biomaterials, dental implant, titanium, zirconia. Published Online: March 19 2021 Significance Statement Available at: Biomaterials have become essential for modern implants. -

1995) Borrelia Burgdorferi-Specific T Lymphocytes Induce Severe Destructive Lyme Arthritis
LTT (Lymphozyten-Proliferationstest, „Lymphozyten-Transformationstest“) Interferon Gamma Test, ELISpot (T-Cell Spot), dem Lymphozytentransformationstest bei Borreliose und bei anderen Infektionskrankheiten Im Lymphozyten-Proliferationstest, auch Lymphozyten-Transformationstest genannt (LTT), wird die Proliferationskapazität von Lymphozyten dargestellt. Der Test dient der Bewertung des Immunstatus oder der Diagnose einer speziellen Sensibilisierung. In the Lymphocyte proliferation assay, also known as lymphocyte transformation test (LTT), the proliferation capacity of lymphocytes is shown. The test is used to evaluate the immune status or the diagnosis of specific sensitization of an object. Im Interferon Gamma Test, dem ELISPOT (Enzyme-Linked ImmunoSpot), auch T- Cellspot genannt, wird durch die Bestimmung der Zytokin – Produktion die Quantität und die Qualität einer T – Zell - Immunantwort zeitnah dokumentiert. In the Interferone Gamma Test, ELISPOT (Enzyme-Linked ImmunoSpot), also called T-Cell spot, represented by the determination of cytokine – Production, the quantity and quality of T - cell - immune response in a timely manner is documented. Lim LC, England DM, DuChateau BK, Glowacki NJ, Schell RF (1995) Borrelia burgdorferi-specific T lymphocytes induce severe destructive Lyme arthritis. Infect. Immun. 63, 1400-1408. Dwyer JM et al. (1979) Behavior of human immunoregulatory cells in culture. L Variables requiring consideration for clinical studies. Clin Exp Immunol 38, 499-513 Johnson C, Dwyer JM (1981) Quantitation of spontaneous suppressor cell activity in human cord blood lymphocytes and their behavior in culture (abstract). Fed Proc 40, 1075 Czerkinsky C, Nilsson L, Nygren H, Ouchterlony O, Tarkowski A (1983) A solid-phase enzyme- linked immunospot (ELISPOT) assay for enumeration of specific antibody-secreting cells.J Immunol Methods 65 (1–2), 109–121. -

Scientific Summary, Digital Implant Solutions
Atlantis® Simplant® Scientific Summary Digital Implant Solutions Comprehensive solutions for all phases of implant dentistry Welcome Are you looking for information about the excellent results with our individually designed Atlantis abutments and suprastructures and how to achieve simplicity, freedom, esthetics, and reliability when treating your patients? Or do you want to explore the research findings behind Simplant, a comprehensive digitial 3D system developed to accomplish more accurate and predictable implant treatment? You will find the answers here, and much more. This Scientific Summary provides a synopsis of the key research findings supporting our digital solutions including Atlantis patient-specific prosthetic solutions and computer guided implant treatment with Simplant. Each summary is based on facts retrieved from the original research article. The Scientific Summary focuses on the following topics: Atlantis® 9 Simplant® 23 References 30 Summary by Dentsply Sirona Implants of facts retrieved from the original articles. For a more comprehensive view of the documentation and research on our products, please refer to our Scientific Reviews. The Scientific Reviews are available for download at www.dentsplyimplants.com/science To improve readability for our customers, Dentsply Sirona does not use ® or ™ in body copy. However, Dentsply Sirona Implants does not waive any right to the trademark and nothing herein shall be interpreted to the contrary. Ongoing innovation For two decades, the Atlantis products and services have been -

Regulations Governing the Classification of Medical Devices (Draft)
Regulations Governing the Classification of Medical Devices (Draft) Article 1 These Regulations are enacted pursuant to Paragraph 2, Article 3 of the Medical Devices Act (hereinafter “this Act”). Article 2 Medical devices are classified into the following categories according to their function, intended use, operating instructions, and working principle, depending on the applicable medical specialty: 1. Clinical chemistry and clinical toxicology devices 2. Hematology and pathology devices 3. Immunology and microbiology devices 4. Anesthesiology devices 5. Cardiovascular devices 6. Dental devices 7. Ear, nose, and throat devices 8. Gastroenterology and urology devices 9. General and plastic surgery devices 10. General hospital and personal use devices 11. Neurological devices 12. Obstetrical and gynecological devices 13. Ophthalmic devices 14. Orthopedic devices 15. Physical medicine devices 16. Radiology devices Article 3 Medical devices are classified into the following classes according to their risk level: 1. Class I: Low risk 2. Class II: Medium risk 3. Class III: High risk 1 Article 4 Product items of the medical device classification are specified in the Annex. In addition to rules stated in the Annex, medical devices whose function, intended use, or working principle are special may have their classification determined according to the following rules: 1. If two or more categories, classes, or product items are applicable to the same medical device, the highest class of risk level is assigned. 2. The accessory to a medical device, intended specifically by the manufacturer for use with a particular medical device, is classified the same as the particular medical device, unless otherwise specified in the Annex. 3. -

Ampath Medical Surveillance Guidelines Metal Chemicals
AMPATH MEDICAL SURVEILLANCE GUIDELINES METAL CHEMICALS TABLE OF CONTENTS Introduction 3 Definitions 4 Biological monitoring 7 Biological effect monitoring 15 Health program 15 Food handler’s health program 16 Driver’s health program 16 Substance abuse in the workplace 17 Alcohol in the workplace 17 Target organs for alcohol abuse 21 Drugs in the workplace 22 Ampath drugs of abuse screening and confirmatory tests on urine 23 Conditions under which a pathologist will testify in court 23 Chain of custody 24 Hazardous chemical regulations 25 Designing and implementing a program of medical surveillance 25 Assessment of potential exposure 25 Table 3 substances 26 Available tests 27 Test interpretation 31 Ampath Quality Assurance 33 Designing exposure profiles 34 Work related hazardous chemical exposure 36 Chemical exposure: DNA adducts 37 Target organs for chemical exposure 39 Chemical exposure profiles 40 Aniline 40 Acetone 41 Benzene 42 Carbon disulphide 43 Carbon monoxide 44 Cyanide 45 Ethyl benzene 46 NN-dimethylformamide 47 Furfural 48 N-hexane 49 © Ampath Medical Surveillance Guideline 1 Isocyanate 50 Methanol 51 Methyl chloroform 52 Methyl ethyl ketone 53 Methyl isobutyl ketone 54 Nitrobenzene 55 Organophosphorous cholinesterase inhibitors 56 Paraquat 57 Parathion 58 Pentachlorophenol 59 Perchloroethylene 60 Phenol 61 Polycyclic aromatic hydrocarbon(PAH) 62 Styrene 64 Toluene 65 Trichloroethylene 67 Xylene 68 Metals 69 Diagnosis and investigation of occupational exposure to metals; a general review 69 Target organs for metal exposure -

Guideline for Disinfection and Sterilization in Healthcare Facilities, 2008
Guideline for Disinfection and Sterilization in Healthcare Facilities, 2008 Guideline for Disinfection and Sterilization in Healthcare Facilities, 2008 William A. Rutala, Ph.D., M.P.H.1,2, David J. Weber, M.D., M.P.H.1,2, and the Healthcare Infection Control Practices Advisory Committee (HICPAC)3 1Hospital Epidemiology University of North Carolina Health Care System Chapel Hill, NC 27514 2Division of Infectious Diseases University of North Carolina School of Medicine Chapel Hill, NC 27599-7030 1 Guideline for Disinfection and Sterilization in Healthcare Facilities, 2008 3HICPAC Members Robert A. Weinstein, MD (Chair) Cook County Hospital Chicago, IL Jane D. Siegel, MD (Co-Chair) University of Texas Southwestern Medical Center Dallas, TX Michele L. Pearson, MD (Executive Secretary) Centers for Disease Control and Prevention Atlanta, GA Raymond Y.W. Chinn, MD Sharp Memorial Hospital San Diego, CA Alfred DeMaria, Jr, MD Massachusetts Department of Public Health Jamaica Plain, MA James T. Lee, MD, PhD University of Minnesota Minneapolis, MN William A. Rutala, PhD, MPH University of North Carolina Health Care System Chapel Hill, NC William E. Scheckler, MD University of Wisconsin Madison, WI Beth H. Stover, RN Kosair Children’s Hospital Louisville, KY Marjorie A. Underwood, RN, BSN CIC Mt. Diablo Medical Center Concord, CA This guideline discusses use of products by healthcare personnel in healthcare settings such as hospitals, ambulatory care and home care; the recommendations are not intended for consumer use of the products discussed. 2 -
Saudi FDA Products Classification Guidance
Saudi FDA Products Classification Guidance دليل تصنيف المنتجات في الهيئة العامة للغذاء والدواء Version 4.0 Date of publication 21/4/2020 Date of implementation 21/5/2020 1 Saudi FDA Products Classification Guidance Version 4.0 Saudi Food & Drug Authority Kingdom of Saudi Arabia Please review and send your comments and suggestions to [email protected] Please visit SFDA’s website at www.sfda.gov.sa for the latest update 2 Saudi Food & Drug Authority Vision and Mission الرؤية وا لرسالة Vision To be a leading international science-based regulator to protect and promote public health. الرؤي ة أن تكو ن هي ئة رائد ة عالمي ا تستن د إلى أسس علمية لتعزيز وحما ية الصحة العامة Mission Protecting the community through regulations and effective controls to ensure the safety of food, drugs, medical devices, cosmetics, pesticides and feed. الرسالة حماية المجتمع من خﻻل تشريعات ومنظومة رقابية فعالة لضمان سﻻمة الغذاء والدواء واﻷجهزة الطبية ومنتجات التجميل والمبيدات واﻷع ﻻف 3 Document Control Version Author Date Comments 3.0 Products Classification Department 11/04/2019 Final 3.1 Products Classification Department 21/10/2019 Final 4.0 Products Classification Department 21/4/2020 Draft 4 Table of Contents 1. INTRODUCTION ............................................................................................................................... 6 1.1 OBJECTIVES ................................................................................................................................... 6 1.2 BACKGROUND ..............................................................................................................................