Ghana Laboratory Viral Load
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
![PPA Public Affairs | 7/1/2016 [PDF]](https://docslib.b-cdn.net/cover/8998/ppa-public-affairs-7-1-2016-pdf-28998.webp)
PPA Public Affairs | 7/1/2016 [PDF]
Vol. 7, Issue 4 Public Procurement Authority: Electronic Bulletin May—Jun 2016 E-Bulletin Public Procurement Authority Accounting For Efficiency & Transparency in the Public Procurement System-The Need For Functional Procurement Units Inside this i s s u e : Editorial : Ac- counting For Efficiency &Transparency —Functional Procurement Units Online Activities : Page 2 Challenges With Establishing Functional Pro- curement Units Page 4 & 5 Corruption Along the Public Pro- curement Cycle - Page 6 & 7 (Continued on page 5) Public Procurement (Amendment) Bill, 2015 Passed. More Details Soon ………. Page 1 Public Procurement Authority: Electronic Bulletin July— Aug 2016 Vol. 7, Issue 4 Online Activities List of entities that have submitted their 2016 Procurement Plans Online As At June 30 , 2016 1. Abor Senior High School 58. Fanteakwa District Assembly 2. Accra Polytechnic 59. Fisheries Commission 3. Accra College of Education 60. Foods and Drugs Board 4. Adiembra Senior High School 61. Forestry Commission 5. Adisadel College 62. Ga South Municipal Assembly 6. Aduman Senior High School 63. Ghana Aids Commission 7. Afadzato South District Assembly 64. Ghana Airports Company Limited 8. Agona West Municipal Assembly 65. Ghana Atomic Energy Commission 9. Ahantaman Senior High Schoolool 66. Ghana Audit Service 10. Akatsi South District Assembly 67. Ghana Book Development Council 11. Akatsi College of Education 68. Ghana Broadcasting Corporation 12. Akim Oda Government Hospital 69. Ghana Civil Aviation Authority 13. Akokoaso Day Senior High School 70. Ghana Cocoa Board 14. Akontombra Senior High School 71. Ghana College of Physicians and Surgeons 15. Akrokerri College of Education 72. Ghana Cylinder Manufacturing Company Limited 16. Akuse Government Hospital 73. -

Ketu North District Assembly
MEDIUM TERM DEVELOPMENT PLAN (2010-2013) 5 MINISTRY OF LOCAL GOVERNMENT AND RURAL DEVELOPMENT KETU NORTH DISTRICT ASSEMBLY MEDIUM TERM DEVELOPMENT PLAN 2010- 2013 Under The Ghana shared growth and development agenda (gsgda) 2010- 2013 PREPARED BY: DISTRICT PLANNING CO-ORDINATING UNIT KETU NORTH DISTRICT ASSEMBLY DZODZE, V/R MAY, 2010 KETU NORTH DISTRICT MEDIUM TERM DEVELOPMENT PLAN (2010-2013) TABLE OF CONTENT CONTENTS PAGE TABLE OF CONTENT 2 LIST OF TABLES 7 LIST OF FIGURES 9 LISTS OF ACRONYMS 10 EXECUTIVE SUMMARY 12 CHAPTER ONE: PERFORMANCE REVIEW AND DISTRICT PROFILE 1.0 PERFORMANCE REVIEW 1.0.1 Introduction 18 1.0.1 Private Sector Competitiveness 18 1 .0.2 Human Resources Development 20 1.0.3 Good Governance and Civic Responsibility 21 1.0.4 Projects Implemented Outside the DMTDP (2006-2009) 22 1.0.5 Problems/Challenges Faced During Implementation 24 1.0.6 Lessons Learnt 24 1.1 PHYSICAL CHARACTERISTICS 1.1.1 Location and size 26 1.1.2 Geology and Soil 29 1.1.3 Relief and Drainage 29 1.1.4 Climate 29 1.1.5 Vegetation 29 1.1.6 Implications for Development 29 1.2 SPATIAL DEVELOPMENT 1.2.1 Surface Accessibility 30 1.2.2 Settlements Pattern 32 1.2.3 Geographical Distribution of Services 32 1.2.4 Land Use Planning and Development Control 34 1.2.5 Land Administration and the Land Market 35 1.2.6 Housing 35 1.2.7 Industry, Commerce and Service 35 1.2.8 Small Scale Industrial Activities 36 1.2.9 Trade and Commerce 36 1.2.10 Financial Services 37 1.2.11 Telecommunications and Postal Services 37 1.2.12 Filling Stations/Liquefied Petroleum Gas -
Volta Region
REGIONAL ANALYTICAL REPORT VOLTA REGION Ghana Statistical Service June, 2013 Copyright © 2013 Ghana Statistical Service Prepared by: Martin K. Yeboah Augusta Okantey Emmanuel Nii Okang Tawiah Edited by: N.N.N. Nsowah-Nuamah Chief Editor: Nii Bentsi-Enchill ii PREFACE AND ACKNOWLEDGEMENT There cannot be any meaningful developmental activity without taking into account the characteristics of the population for whom the activity is targeted. The size of the population and its spatial distribution, growth and change over time, and socio-economic characteristics are all important in development planning. The Kilimanjaro Programme of Action on Population adopted by African countries in 1984 stressed the need for population to be considered as a key factor in the formulation of development strategies and plans. A population census is the most important source of data on the population in a country. It provides information on the size, composition, growth and distribution of the population at the national and sub-national levels. Data from the 2010 Population and Housing Census (PHC) will serve as reference for equitable distribution of resources, government services and the allocation of government funds among various regions and districts for education, health and other social services. The Ghana Statistical Service (GSS) is delighted to provide data users with an analytical report on the 2010 PHC at the regional level to facilitate planning and decision-making. This follows the publication of the National Analytical Report in May, 2013 which contained information on the 2010 PHC at the national level with regional comparisons. Conclusions and recommendations from these reports are expected to serve as a basis for improving the quality of life of Ghanaians through evidence-based policy formulation, planning, monitoring and evaluation of developmental goals and intervention programs. -

Nkwanta North District Assembly
Contents 1 PART A: STRATEGIC OVERVIEW OF THE NKWANTA NORTH DISTRICT ASSEMBLY ......................... 4 1.1 B) ESTABLISHMENT ................................................................................................................ 4 C) POPULATION .................................................................................................................................. 4 1.2 D) DISTRICT ECONOMY .......................................................................................................... 4 1.2.1 I I) AGRICULTURE ............................................................................................................. 4 1.2.2 II) ROADS ......................................................................................................................... 4 REPUBLIC OF GHANA 1.2.3 III) EDUCATION ................................................................................................................ 4 1.2.4 IV) HEALTH ...................................................................................................................... 5 1.2.5 V) ENVIRONMENT ........................................................................................................... 5 COMPOSITE BUDGET VI) TOURISM .................................................................................................................................... 5 THE ASSEMBLY BROAD OBJECTIVES ................................................................................................... 6 FOR 2018-2021 1. GOAL/MISSION .......................................................................................................................... -

A Case Study of Ketu South Municipal Assembly (Ksma)
University of Ghana http://ugspace.ug.edu.gh UNIVERSITY OF GHANA THE IMPACT OF FISCAL DECENTRALISATION ON LOCAL ECONOMIC DEVELOPMENT IN GHANA: A CASE STUDY OF KETU SOUTH MUNICIPAL ASSEMBLY (KSMA) BY EMMANUEL JEFFERSON KWADJO ZUMEGAH (10443139) THIS THESIS IS SUBMITTED TO THE UNIVERSITY OF GHANA, LEGON IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE AWARD OF MPHIL PUBLIC ADMINISTRATION DEGREE JULY, 2015 University of Ghana http://ugspace.ug.edu.gh DECLARATION I EMMANUEL JEFFERSON KWADJO ZUMEGAH hereby declare that this thesis is my own academic research work towards the award of a master of philosophy degree in Public Administration and that no part of this work has been presented or published. All references used in this work has been fully acknowledged. I therefore take full responsibility for any omissions and commissions herein. ……………………………………….. …………………………….. EMMANUEL JEFFERSON KWADJO ZUMEGAH DATE (10443139) i University of Ghana http://ugspace.ug.edu.gh CERTIFICATION I hereby certify that this thesis was supervised in accordance with procedures laid down by the academic board of the University of Ghana, Legon. …………………………………….. ………………………………… DR. KWAME ASAMOAH DATE (SUPERVISOR) ii University of Ghana http://ugspace.ug.edu.gh DEDICATION. To my wife-Mrs. Evelyn Dzifa Melody Zumegah, my kids and to God Almighty iii University of Ghana http://ugspace.ug.edu.gh ACKNOWLEDGMENT The highest form of academic dishonesty I could reach is to assume that the entire work of this thesis is as a result of my individual strength. This thesis has been a solid team work between me and my affable supervisor. I express my sincerest gratitude to Dr. -
Explain & Contain Every Case During 2005!
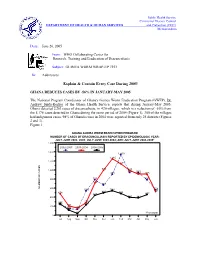
Public Health Service Centers for Disease Control DEPARTMENT OF HEALTH & HUMAN SERVICES and Prevention (CDC) Memorandum Date: June 20, 2005 From: WHO Collaborating Center for Research, Training and Eradication of Dracunculiasis Subject: GUINEA WORM WRAP-UP #153 To: Addressees Explain & Contain Every Case During 2005! GHANA REDUCES CASES BY -56% IN JANUARY-MAY 2005 The National Program Coordinator of Ghana's Guinea Worm Eradication Program (GWEP), Dr. Andrew_Seidu-Korkor of the Ghana Health Service, reports that during January-May 2005, Ghana detected 2,263 cases of dracunculiasis, in 420 villages, which is a reduction of -56% from the 5,176 cases detected in Ghana during the same period of 2004 (Figure 1). 300 of the villages had indigenous cases. 98% of Ghana's cases in 2004 were reported from only 25 districts (Figures 2 and 3). Figure 1 GHANA GUINEA WORM ERADICATION PROGRAM NUMBER OF CASES OF DRACUNCULIASIS REPORTED BY EPIDEMIOLOGIC YEAR: JULY-JUNE 2002- 2003; JULY-JUNE 2003-2004; AND JULY-JUNE 2004-2005* 1,600 2002-2003 2003-2004 2004-2005 1,400 1,339 1,245 1,200 1,133 996 990 1,000 944 940 903 907 905 800 785 785 712 665 NUMBER OF CASES 600 558 539 544 520 474 496 482 439 457 400 393 387 257 278 234 230 203 200 142 158 115 131 38 *Provisional 0 Jul Aug Sept Oct Nov Dec Jan Feb Mar Apr May Jun Two districts, Nkwanta (Volta Region) and Tolon-Kumbungu (Northern Region), that together reported 35% of Ghana's cases in 2004, have recorded reductions of -90% (from 1,006 to 97 cases) and -11% (from 452 to 404 cases), respectively, in cases during Jan. -

GNHR) P164603 CR No 6337-GH REF No.: GH-MOGCSP-190902-CS-QCBS
ENGAGEMENT OF A FIRM FOR DATA COLLECTION IN THE VOLTA REGION OF GHANA FOR THE GHANA NATIONAL HOUSEHOLD REGISTRY (GNHR) P164603 CR No 6337-GH REF No.: GH-MOGCSP-190902-CS-QCBS I. BACKGROUND & CONTEXT The Ministry of Gender, Children and Social Protection (MGCSP) as a responsible institution to coordinate the implementation of the country’s social protection system has proposed the establishment of the Ghana National Household Registry (GNHR), as a tool that serves to assist social protection programs to identify, prioritize, and select households living in vulnerable conditions to ensure that different social programs effectively reach their target populations. The GNHR involves the registry of households and collection of basic information on their social- economic status. The data from the registry can then be shared across programs. In this context, the GNHR will have the following specific objectives: a) Facilitate the categorization of potential beneficiaries for social programs in an objective, homogeneous and equitable manner. b) Support the inter-institutional coordination to improve the impact of social spending and the elimination of duplication c) Allow the design and implementation of accurate socioeconomic diagnoses of poor people, to support development of plans, and the design and development of specific programs targeted to vulnerable and/or low-income groups. d) Contribute to institutional strengthening of the MoGCSP, through the implementation of a reliable and central database of vulnerable groups. For the implementation of the Ghana National Household Registry, the MoGCSP has decided to use a household evaluation mechanism based on a Proxy Means Test (PMT) model, on which welfare is determined using indirect indicators that collectively approximate the socioeconomic status of individuals or households. -

National Communications Authority List Of
NATIONAL COMMUNICATIONS AUTHORITY LIST OF AUTHORISED VHF-FM RADIO STATIONS IN GHANA AS AT THIRD QUARTER, 2019 Page 1 of 74 OVERVIEW OF FM RADIO BROADCASTING STATIONS IN GHANA Section 2 of the Electronic Communications Act, 2008, Act 775 mandates that the National Communications Authority “shall regulate the radio spectrum designated or allocated for use by broadcasting organisations and providers of broadcasting services”; “… determine technical and other standards and issue guidelines for the operation of broadcasting organisations …” “… may adopt policies to cater for rural communities and for this purpose may waive fees wholly or in part for the grant of a frequency authorisation”. The Broadcasting service is a communication service in which the transmissions are intended for direct reception by the general public. The sound broadcasting service involves the broadcasting of sound which may be accompanied by associated text/data. Sound broadcasting is currently deployed in Ghana using analogue transmission techniques: Amplitude Modulation (AM) and Frequency Modulation (FM). Over the last two decades, AM sound broadcasting has faded, leaving FM radio as the only form of sound broadcasting in Ghana. FM radio broadcasting stations are classified for the purpose of regulatory administration of the service towards the attainment of efficient use of frequency. The following is the classification of FM radio broadcasting stations in Ghana. (1) Classification by Purpose: a) Public – all stations owned and operated by the Ghana Broadcasting Corporation (GBC) and/or any other station established by the Government of Ghana by a statutory enactment. b) Public Foreign – stations established by Foreign Governments through diplomatic arrangements to rebroadcast/relay content from foreign countries e.g. -

SUSTAINABLE FISHERIES MANAGEMENT PROJECT (SFMP) Post Harvest Loss Reduction Study
SUSTAINABLE FISHERIES MANAGEMENT PROJECT (SFMP) Post Harvest Loss Reduction Study October 2015 This publication is available electronically on the Coastal Resources Center’s website at http://www.crc.uri.edu/projects_page/ghanasfmp/ For more information on the Ghana Sustainable Fisheries Management Project, contact: USAID/Ghana Sustainable Fisheries Management Project Coastal Resources Center Graduate School of Oceanography University of Rhode Island 220 South Ferry Rd. Narragansett, RI 02882 USA Tel: 401-874-6224 Fax: 401-874-6920 Email: [email protected] Citation: Dapaah, G., Samey, B. (2015). Post Harvesting Loss Reduction Study Report. The USAID/Ghana Sustainable Fisheries Management Project (SFMP). Narragansett, RI: Coastal Resources Center, Graduate School of Oceanography, University of Rhode Island and SNV Netherlands Development Organization. GH2014_ACT016_SNV. 90 pp. Authority/Disclaimer: Prepared for USAID/Ghana under Cooperative Agreement (AID-641-A-15-00001) awarded on October 22, 2014 to the University of Rhode Island and entitled; the USAID/Ghana Sustainable Fisheries Management Project (SFMP). This document is made possible by the support of the American People through the United States Agency for International Development (USAID). The views expressed and opinions contained in this report are those of the SFMP team and are not intended as statements of policy of either USAID or the cooperating organizations. As such, the contents of this report are the sole responsibility of the SFMP Project team and do not necessarily reflect -
![PPA Public Affairs | 1/7/2016 [PDF]](https://docslib.b-cdn.net/cover/9264/ppa-public-affairs-1-7-2016-pdf-1799264.webp)
PPA Public Affairs | 1/7/2016 [PDF]
Vol. 7, Issue 1 Public Procurement Authority: Electronic Bulletin Jan-Feb 2016 E-Bulletin Public Procurement Authority THE PERCEPTION OF SINGLE SOURCE AS A Inside this MAJOR METHOD OF PROCUREMENT- i s s u e : HOW REAL IS IT ? Editorial : Perception of Single Source Online Activities : Page 2 Benefits Of Procurement Processes-Page 3 Legal Framework for Use of Single Source -Page 5 Annex 1: Single Source Contract Awards Publication 2013 Page 8 Annex 2: Single Source Contract Awards Publication 2014 Page 37 (Continued on page 3) Has Your Entity Submitted Its 2016 Procurement Plan—Using PPA’s Online System ? Page 1 Public Procurement Authority: Electronic Bulletin Jan-Feb 2015 Vol. 7, Issue 1 Online Activities List of entities that have submitted their 2014 Procurement Plans online As At December 31 , 2015 1. Akwapim South Municipal Assembly 2. Bank of Ghana 3. Council of State 4. Economic and Organised Crime Office 5. Energy Commission 6. Environmental Protection Agency 7. Ghana Cocoa Board 8. Ghana College of Physicians and Surgeons 9. Ghana Grid Company Limited 10. Ghana Police Service 11. Ghana Standards Authority 12. Ketu District Hospital 13. Korle Bu Teaching Hospital 14. Management Development And Productivity In- stitute 15. Ministry of Fisheries and Aquaculture Develop- ment 16. Ministry Of Foreign Affairs And Regional Integra- tion 17. Ministry Of Health 18. Ministry Of Roads And Highways 19. National Pensions Regulatory Authority 20. National Service Secretariat 21. Nyakrom Day Senior High School 22. Petroleum Commission 23. Pharmacy Council 24. Presby College of Education - Akropong 25. St. Monica College of Education 26. Suhum Government Hospital 27. -

Certified Electrical Wiring Professionals Volta Regional Register Certification No
CERTIFIED ELECTRICAL WIRING PROFESSIONALS VOLTA REGIONAL REGISTER CERTIFICATION NO. NAME PHONE NUMBER PLACE OF WORK PIN NUMBER CLASS 1 ABOTSI FELIX GBOMOSHOW 0246296692 DENU EC/CEWP1/06/18/0020 DOMESTIC 2 ACKUAYI JOSEPH DOTSE 0244114574 ANYAKO EC/CEWP1/12/14/0021 DOMESTIC 3 ADANU KWASHIE WISDOM 0245768361 DZODZE, VOLTA REGION EC/CEWP1/06/16/0025 DOMESTIC 4 ADEVOR FRANCIS 0241658220 AVE-DAKPA EC/CEWP1/12/19/0013 DOMESTIC 5 ADISENU ADOLF QUARSHIE 0246627858 AGBOZUME EC/CEWP1/12/14/0039 DOMESTIC 6 ADJEI-DZIDE FRANKLIN ELENUJOR NOVA KING 0247928015 KPANDO, VOLTA EC/CEWP1/12/18/0025 DOMESTIC 7 ADOR AFEAFA 0246740864 SOGAKOPE EC/CEWP1/12/19/0018 DOMESTIC 8 ADZALI PAUL KOMLA 0245789340 TAFI MADOR EC/CEWP1/12/14/0054 DOMESTIC 9 ADZAMOA DIVINE MENSAH 0242769759 KRACHI EC/CEWP1/12/18/0031 DOMESTIC 10 ADZRAKU DODZI 0248682929 ALAVANYO EC/CEWP1/12/18/0033 DOMESTIC 11 AFADZINOO MIDAWO 0243650148 ANLO AFIADENYIGBA EC/CEWP1/06/14/0174 DOMESTIC 12 AFUTU BRIGHT 0245156375 HOHOE EC/CEWP1/12/18/0035 DOMESTIC 13 AGBALENYO CHRISTIAN KOFI 0285167920 ANLOKODZI, HO EC/CEWP1/12/13/0024 DOMESTIC 14 AGBAVE KINDNESS JERRY 0505231782 AKATSI, VOLTA REGION EC/CEWP1/12/15/0040 DOMESTIC 15 AGBAVOR SIMON 0243436475 KPANDO EC/CEWP1/12/16/0050 DOMESTIC 16 AGBAVOR VICTOR KWAKU 0244298648 AKATSI EC/CEWP1/06/14/0177 DOMESTIC 17 AGBEKO MICHEAL 0557912356 SOGAKOFE EC/CEWP1/06/19/0095 DOMESTIC 18 AGBEMADE SIMON 0244049157 DABALA, SOGAKOPE,VOLTA REGIONEC/CEWP1/12/16/0052 DOMESTIC 19 AGBEMAFLE MICHAEL 0248481385 HOHOE EC/CEWP1/12/18/0038 DOMESTIC 20 AGBENORKU KWAKU EMMANUEL 0506820579 DABALA JUNCTION- SOGAKOPE, VOLEC/CEWP1/12/17/0053 DOMESTIC 21 AGBENYEFIA SENANU FRANCIS 0244937008 CENTRAL TONGU EC/CEWP1/06/17/0046 DOMESTIC 22 AGBODOVI K. -

A Strategy for Church Planting Among the Ewe-Speaking People of the Volta Region, Ghana
Andrews University Digital Commons @ Andrews University Dissertation Projects DMin Graduate Research 1997 A Strategy For Church Planting Among The Ewe-Speaking People Of The Volta Region, Ghana Emmanuel Osei Andrews University Follow this and additional works at: https://digitalcommons.andrews.edu/dmin Part of the Practical Theology Commons Recommended Citation Osei, Emmanuel, "A Strategy For Church Planting Among The Ewe-Speaking People Of The Volta Region, Ghana" (1997). Dissertation Projects DMin. 344. https://digitalcommons.andrews.edu/dmin/344 This Project Report is brought to you for free and open access by the Graduate Research at Digital Commons @ Andrews University. It has been accepted for inclusion in Dissertation Projects DMin by an authorized administrator of Digital Commons @ Andrews University. For more information, please contact [email protected]. ABSTRACT A STRATEGY FOR CHURCH PLANTING AMONG THE EWE-SPEAKING PEOPLE OF THE VOLTA REGION, GHANA by Emmanuel Osei Adviser: Douglas R. Kilcher ABSTRACT OF GRADUATE STUDENT RESEARCH Dissertation Andrews University Seventh-day Adventist Theological Seminary Title: A STRATEGY FOR CHURCH PLANTING AMONG THE EWE- SPEAKING PEOPLE OF THE VOLTA REGION, GHANA Name of researcher: Emmanuel Osei Name of degree of faculty chair: Douglas R. Kilcher, D.Min Date completed: August 1997 Problem Since the Seventh-day Adventist Church came to Ghana over one hundred years ago, there has not been any concrete and coordinated plan to establish SDA churches among the Ewe-speaking people of the Volta Region, Ghana. Unconsciously or otherwise, the Volta Region has been left unentered by the church, particularly the area from Ho southward to the sea. This study was undertaken to develop a strategy for reaching the Ewe-speaking people group (of the Volta Region Ghana) through church-planting ministry by which converts won would be gathered to form congregations of the Seventh- day Adventist Church.