The Facial Platysma and Its Underappreciated Role in Lower
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Muscular System Views
1 PRE-LAB EXERCISES Before coming to lab, get familiar with a few muscle groups we’ll be exploring during lab. Using Visible Body’s Human Anatomy Atlas, go to the Views section. Under Systems, scroll down to the Muscular System views. Select the view Expression and find the following muscles. When you select a muscle, note the book icon in the content box. Selecting this icon allows you to read the muscle’s definition. 1. Occipitofrontalis (epicranius) 2. Orbicularis oculi 3. Orbicularis oris 4. Nasalis 5. Zygomaticus major Return to Muscular System views, select the view Head Rotation and find the following muscles. 1. Sternocleidomastoid 2. Scalene group (anterior, middle, posterior) 2 IN-LAB EXERCISES Use the following modules to guide your exploration of the head and neck region of the muscular system. As you explore the modules, locate the muscles on any charts, models, or specimen available. Please note that these muscles act on the head and neck – those that are located in the neck but act on the back are in a separate section. When reviewing the action of a muscle, it will be helpful to think about where the muscle is located and where the insertion is. Muscle physiology requires that a muscle will “pull” instead of “push” during contraction, and the insertion is the part that will move. Imagine that the muscle is “pulling” on the bone or tissue it is attached to at the insertion. Access 3D views and animated muscle actions in Visible Body’s Human Anatomy Atlas, which will be especially helpful to visualize muscle actions. -

Questions on Human Anatomy
Standard Medical Text-books. ROBERTS’ PRACTICE OF MEDICINE. The Theory and Practice of Medicine. By Frederick T. Roberts, m.d. Third edi- tion. Octavo. Price, cloth, $6.00; leather, $7.00 Recommended at University of Pennsylvania. Long Island College Hospital, Yale and Harvard Colleges, Bishop’s College, Montreal; Uni- versity of Michigan, and over twenty other medical schools. MEIGS & PEPPER ON CHILDREN. A Practical Treatise on Diseases of Children. By J. Forsyth Meigs, m.d., and William Pepper, m.d. 7th edition. 8vo. Price, cloth, $6.00; leather, $7.00 Recommended at thirty-five of the principal medical colleges in the United States, including Bellevue Hospital, New York, University of Pennsylvania, and Long Island College Hospital. BIDDLE’S MATERIA MEDICA. Materia Medica, for the Use of Students and Physicians. By the late Prof. John B Biddle, m.d., Professor of Materia Medica in Jefferson Medical College, Phila- delphia. The Eighth edition. Octavo. Price, cloth, $4.00 Recommended in colleges in all parts of the UnitedStates. BYFORD ON WOMEN. The Diseases and Accidents Incident to Women. By Wm. H. Byford, m.d., Professor of Obstetrics and Diseases of Women and Children in the Chicago Medical College. Third edition, revised. 164 illus. Price, cloth, $5.00; leather, $6.00 “ Being particularly of use where questions of etiology and general treatment are concerned.”—American Journal of Obstetrics. CAZEAUX’S GREAT WORK ON OBSTETRICS. A practical Text-book on Midwifery. The most complete book now before the profession. Sixth edition, illus. Price, cloth, $6.00 ; leather, $7.00 Recommended at nearly fifty medical schools in the United States. -

The Articulatory System Chapter 6 Speech Science/ COMD 6305 UTD/ Callier Center William F. Katz, Ph.D
The articulatory system Chapter 6 Speech Science/ COMD 6305 UTD/ Callier Center William F. Katz, Ph.D. STRUCTURE/FUNCTION VOCAL TRACT CLASSIFICATION OF CONSONANTS AND VOWELS MORE ON RESONANCE ACOUSTIC ANALYSIS/ SPECTROGRAMS SUPRSEGMENTALS, COARTICULATION 1 Midsagittal dissection From Kent, 1997 2 Oral Cavity 3 Oral Structures – continued • Moistened by saliva • Lined by mucosa • Saliva affected by meds 4 Tonsils • PALATINE* (laterally – seen in oral periph • LINGUAL (inf.- root of tongue) • ADENOIDS (sup.) [= pharyngeal] • Palatine, lingual tonsils are larger in children • *removed in tonsillectomy 5 Adenoid Facies • Enlargement from infection may cause problems (adenoid facies) • Can cause problems with nasal sounds or voicing • Adenoidectomy; also tonsillectomy (for palatine tonsils) 6 Adenoid faces (example) 7 Oral structures - frenulum Important component of oral periphery exam Lingual frenomy – for ankyloglossia “tongue-tie” Some doctors will snip for infants, but often will loosen by itself 8 Hard Palate Much variability in palate shape and height Very high vault 9 Teeth 10 Dentition - details Primary (deciduous, milk teeth) Secondary (permanent) n=20: n=32: ◦ 2 incisor ◦ 4 incisor ◦ 1 canine ◦ 2 canine ◦ 2 molar ◦ 4 premolar (bicuspid) Just for “fun” – baby ◦ 6 molar teeth pushing in! NOTE: x 2 for upper and lower 11 Types of malocclusion • Angle’s classification: • I, II, III • Also, individual teeth can be misaligned (e.g. labioversion) Also “Neutrocclusion/ distocclusion/mesiocclusion” 12 Dental Occlusion –continued Other terminology 13 Mandible Action • Primary movements are elevation and depression • Also…. protrusion/retraction • Lateral grinding motion 14 Muscles of Jaw Elevation Like alligators, we are much stronger at jaw elevation (closing to head) than depression 15 Jaw Muscles ELEVATORS DEPRESSORS •Temporalis ✓ •Mylohyoid ✓ •Masseter ✓ •Geniohyoid✓ •Internal (medial) Pterygoid ✓ •Anterior belly of the digastric (- Kent) •Masseter and IP part of “mandibular sling” •External (lateral) pterygoid(?)-- also protrudes and rocks side to side. -

Human Anatomy
Human Anatomy د.فراس عبد الرحمن Lec.13 The neck Overview The neck is the area of the body between the base of the cranium superiorly and the suprasternal notch and the clavicles inferiorly. The neck joins the head to the trunk and limbs, serving as a major conduit for structures passing between them. Many important structures are crowded together in the neck, such as muscles, arteries, veins, nerves, lymphatics, thyroid and parathyroid glands, trachea, larynx, esophagus, and vertebrae. Carotid/jugular blood vessels are the major structures commonly injured in penetrating wounds of the neck. The brachial plexuses of nerves originate in the neck and pass inferolaterally to enter the axillae and continue to supply the upper limbs. Lymph from structures in the head and neck drains into cervical lymph nodes. Skin of the Neck The natural lines of cleavage of the skin (Wrinkle lines) are constant and run almost horizontally around the neck. This is important clinically because an incision along a cleavage line will heal as a narrow scar, whereas one that crosses the lines will heal as a wide or heaped-up scar. Fasciae of the Neck The neck is surrounded by a superficial cervical fascia that lies deep to the skin and invests the platysma muscle (a muscle of facial expression). A second deep cervical fascia tightly invests the neck structures and is divided into three layers. Superficial Cervical Fascia The superficial fascia of the neck forms a thin layer that encloses the platysma muscle. Also embedded in it are the cutaneous nerves, the superficial veins, and the superficial lymph nodes. -
Weakness, Dysphagia, and Stridor After Botulinum Toxin Injections
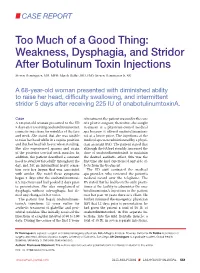
CASE REPORT Too Much of a Good Thing: Weakness, Dysphagia, and Stridor After Botulinum Toxin Injections Steven Dominguez, MD, MPH; Marek Dobke, MD, PhD; Steven Dominguez Jr, BS A 68-year-old woman presented with diminished ability to raise her head, difficulty swallowing, and intermittent stridor 5 days after receiving 225 IU of onabotulinumtoxinA. Case of treatment, the patient was under the care A 68-year-old woman presented to the ED of a plastic surgeon; thereafter, she sought 5 days after receiving onabotulinumtoxinA treatment at a physician-owned medical cosmetic injections for wrinkles of the face spa because it offered onabotulinumtoxi- and neck. She stated that she was unable nA at a lower price. The injections at the to raise her head while in a supine position medical spa were administered by a physi- and that her head felt heavy when standing. cian assistant (PA). The patient stated that She also experienced spasms and strain although the PA had steadily increased the of the posterior cervical neck muscles. In dose of onabotulinumtoxinA to maintain addition, the patient described a constant the desired aesthetic effect, this was the need to swallow forcefully throughout the first time she had experienced any side ef- day, and felt an intermittent heavy sensa- fects from the treatment. tion over her larynx that was associated The ED staff contacted the medical with stridor. She noted these symptoms spa provider, who reviewed the patient’s began 5 days after the onabotulinumtoxi- medical record over the telephone. The nA injections and had peaked 2 days prior PA stated that he had been the only practi- to presentation. -
Making Faces
Making Faces Chris Landreth CSC2529, Session 4 31 January 2011 AU1,2 (Frontalis): 2 AU4 (Corrugator): 1 AU5 (Levitor Palpabrae): 3 AU6,44 (Orbicularis Oculi): 6 How AU9 (Alaeque Nasi Labius Superioris): 1 AU10 (Labius Superioris): 3 many AU12 (Zygomatic Major): 3 letters in AU14 (Buccinator): 3 AU15 (Triangularis): 3 this AU16 (Labius Inferioris): 1 alphabet? AU17 (Mentalis): 1 AU18 (Incisivus): 1 AU20 (Risorius/Platysma): 3 AU22,23 (Orbicularis Oris): 6 AU26 (Jaw): 4 _________________________________________________ TOTAL: 41 AU’s Putting the letters together into words: Expressions The six fundamental expressions: 1. Anger 2. Sadness 3. Disgust 4. Surprise 5. Fear 6. Happiness The six fundamental expressions: 1. Anger 2. Sadness 3. Disgust 4. Surprise 5. Fear 6. Happiness A Few Words of Anger Glaring: A Few Words of Anger Glaring: Slight creases in the middle brow (Currogator) Eyelids are slightly raised (Levitor Palpabrae) Lips are clenched backward (Buccinator) Slight downturn in lip corners (Triangularis) A Few Words of Anger Miffed: A Few Words of Anger Miffed: Classic, angry ‘v-shaped’ eyebrows (Currogator) Nasolabial fold deepens, Upper lip is squared off (A.N. Labius Superioris) Lower lip raises into a pout, Dimpling in the chin (Mentalis) A Few Words of Anger Pissed off: A Few Words of Anger Pissed off: Brow raises slightly (Frontalis) Sharper Nasolabial Fold, Raised upper lip (A.N. Labius Superioris) Lower lip juts out (Orb. Oris, Lower Lip out) A Few Words of Anger Very Pissed off: A Few Words of Anger Very Pissed off: Slight squinting (Orb. Oculi) Bared upper teeth (Orb. Oris, Upper Lip Out) Squared lower lip corners, Sharp tendon creases in her neck (Risorius/Platysma) A Few Words of Anger Consumed in Rage: A Few Words of Anger Consumed in Rage: Intense, asymmetrical squinting (Orb. -

Yagenich L.V., Kirillova I.I., Siritsa Ye.A. Latin and Main Principals Of
Yagenich L.V., Kirillova I.I., Siritsa Ye.A. Latin and main principals of anatomical, pharmaceutical and clinical terminology (Student's book) Simferopol, 2017 Contents No. Topics Page 1. UNIT I. Latin language history. Phonetics. Alphabet. Vowels and consonants classification. Diphthongs. Digraphs. Letter combinations. 4-13 Syllable shortness and longitude. Stress rules. 2. UNIT II. Grammatical noun categories, declension characteristics, noun 14-25 dictionary forms, determination of the noun stems, nominative and genitive cases and their significance in terms formation. I-st noun declension. 3. UNIT III. Adjectives and its grammatical categories. Classes of adjectives. Adjective entries in dictionaries. Adjectives of the I-st group. Gender 26-36 endings, stem-determining. 4. UNIT IV. Adjectives of the 2-nd group. Morphological characteristics of two- and multi-word anatomical terms. Syntax of two- and multi-word 37-49 anatomical terms. Nouns of the 2nd declension 5. UNIT V. General characteristic of the nouns of the 3rd declension. Parisyllabic and imparisyllabic nouns. Types of stems of the nouns of the 50-58 3rd declension and their peculiarities. 3rd declension nouns in combination with agreed and non-agreed attributes 6. UNIT VI. Peculiarities of 3rd declension nouns of masculine, feminine and neuter genders. Muscle names referring to their functions. Exceptions to the 59-71 gender rule of 3rd declension nouns for all three genders 7. UNIT VII. 1st, 2nd and 3rd declension nouns in combination with II class adjectives. Present Participle and its declension. Anatomical terms 72-81 consisting of nouns and participles 8. UNIT VIII. Nouns of the 4th and 5th declensions and their combination with 82-89 adjectives 9. -

A Comprehensive Review of Anatomy and Regional Anesthesia Techniques of Clavicle Surgeries
vv ISSN: 2641-3116 DOI: https://dx.doi.org/10.17352/ojor CLINICAL GROUP Received: 31 March, 2021 Research Article Accepted: 07 April, 2021 Published: 10 April, 2021 *Corresponding author: Dr. Kartik Sonawane, Uncovering secrets of the Junior Consultant, Department of Anesthesiol- ogy, Ganga Medical Centre & Hospitals, Pvt. Ltd. Coimbatore, Tamil Nadu, India, E-mail: beauty bone: A comprehensive Keywords: Clavicle fractures; Floating shoulder sur- gery; Clavicle surgery; Clavicle anesthesia; Procedure review of anatomy and specific anesthesia; Clavicular block regional anesthesia techniques https://www.peertechzpublications.com of clavicle surgeries Kartik Sonawane1*, Hrudini Dixit2, J.Balavenkatasubramanian3 and Palanichamy Gurumoorthi4 1Junior Consultant, Department of Anesthesiology, Ganga Medical Centre & Hospitals, Pvt. Ltd., Coimbatore, Tamil Nadu, India 2Fellow in Regional Anesthesia, Department of Anesthesiology, Ganga Medical Centre & Hospitals, Pvt. Ltd., Coimbatore, Tamil Nadu, India 3Senior Consultant, Department of Anesthesiology, Ganga Medical Centre & Hospitals, Pvt. Ltd., Coimbatore, Tamil Nadu, India 4Consultant, Department of Anesthesiology, Ganga Medical Centre & Hospitals, Pvt. Ltd., Coimbatore, Tamil Nadu, India Abstract The clavicle is the most frequently fractured bone in humans. General anesthesia with or without Regional Anesthesia (RA) is most frequently used for clavicle surgeries due to its complex innervation. Many RA techniques, alone or in combination, have been used for clavicle surgeries. These include interscalene block, cervical plexus (superficial and deep) blocks, SCUT (supraclavicular nerve + selective upper trunk) block, and pectoral nerve blocks (PEC I and PEC II). The clavipectoral fascial plane block is also a safe and simple option and replaces most other RA techniques due to its lack of side effects like phrenic nerve palsy or motor block of the upper limb. -

Chin Ptosis: Classification, Anatomy, and Correction/Garfein, Zide 3
Chin Ptosis: Classification, Anatomy, and Correction Evan S. Garfein, M.D.,1 and Barry M. Zide, D.M.D., M.D.1 ABSTRACT For years, the notion of chin ptosis was somehow integrated with the concept of witch’s chin. That was a mistake on many levels because chin droop has four major causes, all different and with some overlap. With this article, the surgeon can quickly diagnose which type and which therapeutic modality would work best. In some cases the problem is a simple fix, in others the droop can only be stabilized, and in the final two, definite corrective procedures are available. Of note, in certain situations two types of chin ptosis may overlap because both the patient and the surgeon may each contribute to the problems. For example, in dynamic ptosis, a droop that occurs with smile in the unoperated patient can be exacerbated and further produced by certain surgical methods also. This paper classifies the variations of the problems and explains the anatomy with the final emphasis on long-term surgical correction, well described herein. This article is the ninth on this subject and a review of them all would be helpful (greatly) for understanding the enigmas of the lower face. KEYWORDS: Lip incompetence, chin ptosis, witch’s chin, chin droop, mentalis muscle All chin ptosis patients are not alike. The abnormal anatomy, diagnosis, and management of the proper diagnosis of the type of chin ptosis places the four types of chin ptosis, as well as how to manage patient into one of four categories, which will deter- dynamic ptosis in the presence of other problems— mine who can and who cannot be helped and by which surgeon-caused or not. -

Appendix B: Muscles of the Speech Production Mechanism
Appendix B: Muscles of the Speech Production Mechanism I. MUSCLES OF RESPIRATION A. MUSCLES OF INHALATION (muscles that enlarge the thoracic cavity) 1. Diaphragm Attachments: The diaphragm originates in a number of places: the lower tip of the sternum; the first 3 or 4 lumbar vertebrae and the lower borders and inner surfaces of the cartilages of ribs 7 - 12. All fibers insert into a central tendon (aponeurosis of the diaphragm). Function: Contraction of the diaphragm draws the central tendon down and forward, which enlarges the thoracic cavity vertically. It can also elevate to some extent the lower ribs. The diaphragm separates the thoracic and the abdominal cavities. 2. External Intercostals Attachments: The external intercostals run from the lip on the lower border of each rib inferiorly and medially to the upper border of the rib immediately below. Function: These muscles may have several functions. They serve to strengthen the thoracic wall so that it doesn't bulge between the ribs. They provide a checking action to counteract relaxation pressure. Because of the direction of attachment of their fibers, the external intercostals can raise the thoracic cage for inhalation. 3. Pectoralis Major Attachments: This muscle attaches on the anterior surface of the medial half of the clavicle, the sternum and costal cartilages 1-6 or 7. All fibers come together and insert at the greater tubercle of the humerus. Function: Pectoralis major is primarily an abductor of the arm. It can, however, serve as a supplemental (or compensatory) muscle of inhalation, raising the rib cage and sternum. (In other words, breathing by raising and lowering the arms!) It is mentioned here chiefly because it is encountered in the dissection. -
![Anatomy of the Face] 2018-2019](https://docslib.b-cdn.net/cover/5898/anatomy-of-the-face-2018-2019-1375898.webp)
Anatomy of the Face] 2018-2019
By Dr. Hassna B. Jawad [ANATOMY OF THE FACE] 2018-2019 Objective : At the end of this lecture you should be able to : 1. Identify the extent of the face. 2. Enlist the layers of the face and recognize their importance 3. Recognize the groups of the muscles of facial expression its origin ,insertion and function 4. Test the muscle of facial expression clinically 5. Discuss some clinical notes regarding the face Extends from lower border of mandible to the hair line (forehead is common for face and scalp) and laterally to the ear auricle Layers Of the Face 1.SKIN The face has elastic and vascular skin. The skin of the face has large number of sweat and sebaceous glands. The sebaceous glands keep the face greasy by their secretion and sweat glands help modulate the body temperature *Applied Anatomy :Face is also the common site for acne as a result of presence of large number of sebaceous glands in this region. 2. SUPERFICIAL FASIA It includes muscles of facial expression, vessels and nerves and varying amount of fat. The fat is absent in the eyelids but is well grown in cheeks creating buccal pad of fat, which gives rounded contour to cheeks. 3. DEEP FASCIA The deep fascia is absent in the region of face with the exception of over the parotid gland and masseter muscle that are covered by parotidomasseteric fascia. The absence of deep fascia in the face is important for the facial expression. The majority of them originate from bones of the skull and are added into the skin. -

Understanding the Perioral Anatomy
2.0 ANCC CE Contact Hours Understanding the Perioral Anatomy Tracey A. Hotta , RN, BScN, CPSN, CANS gently infl ate and cause lip eversion. Injection into Rejuvenation of the perioral region can be very challenging the lateral upper lip border should be done to avoid because of the many factors that affect the appearance the fade-away lip. The client may also require injec- of this area, such as repeated muscle movement caus- tions into the vermillion border to further highlight ing radial lip lines, loss of the maxillary and mandibular or defi ne the lip. The injections may be performed bony support, and decrease and descent of the adipose by linear threading (needle or cannula) or serial tissue causing the formation of “jowls.” Environmental puncture, depending on the preferred technique of issues must also be addressed, such as smoking, sun the provider. damage, and poor dental health. When assessing a client Group 2—Atrophic lips ( Figure 2 ): These clients have for perioral rejuvenation, it is critical that the provider un- atrophic lips, which may be due to aging or genetics, derstands the perioral anatomy so that high-risk areas may and are seeking augmentation to make them look be identifi ed and precautions are taken to prevent serious more youthful. After an assessment and counseling adverse events from occurring. as to the limitations that may be achieved, a treat- ment plan is established. The treatment would begin he lips function to provide the ability to eat, speak, with injection into the wet–dry junction to achieve and express emotion and, as a sensory organ, to desired volume; additional injections may be per- T symbolize sensuality and sexuality.