Serco Letterhead
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
MAIB Report No 32/2014
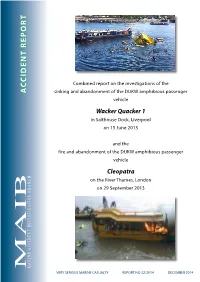
ACCIDENT REPORT ACCIDENT sinking oftheDUKW andabandonment amphibiouspassenger VERY SERIOUS MARINE CASUALTY REPORT NO CASUALTY SERIOUS MARINE VERY fire and abandonment of the DUKW amphibious passenger oftheDUKW andabandonment fire amphibiouspassenger Combined report on the investigations ofthe reportCombined ontheinvestigations on the River Thames, London Thames, on theRiver in Salthouse Dock, Liverpool H Wacker Quacker 1 Quacker Wacker on 29 September 2013 on 29September NC on 15June2013 A Cleopatra R and the vehicle vehicle N B IO T A G TI S 32 /2014 DECEMBER 2014 INVE T DEN I C C A NE RI A M Extract from The United Kingdom Merchant Shipping (Accident Reporting and Investigation) Regulations 2012 – Regulation 5: “The sole objective of the investigation of an accident under the Merchant Shipping (Accident Reporting and Investigation) Regulations 2012 shall be the prevention of future accidents through the ascertainment of its causes and circumstances. It shall not be the purpose of an investigation to determine liability nor, except so far as is necessary to achieve its objective, to apportion blame.” NOTE This report is not written with litigation in mind and, pursuant to Regulation 14(14) of the Merchant Shipping (Accident Reporting and Investigation) Regulations 2012, shall be inadmissible in any judicial proceedings whose purpose, or one of whose purposes is to attribute or apportion liability or blame. © Crown copyright, 2014 You may re-use this document/publication (not including departmental or agency logos) free of charge in any format or medium. You must re-use it accurately and not in a misleading context. The material must be acknowledged as Crown copyright and you must give the title of the source publication. -

OPENING Remarksâ•Fltwelfth VERTEBRATE PEST CONFERENCE
University of Nebraska - Lincoln DigitalCommons@University of Nebraska - Lincoln Proceedings of the Twelfth Vertebrate Pest Vertebrate Pest Conference Proceedings Conference (1986) collection March 1986 OPENING REMARKS—TWELFTH VERTEBRATE PEST CONFERENCE Terrell P. Salmon University of California, Davis, California Follow this and additional works at: https://digitalcommons.unl.edu/vpc12 Part of the Environmental Health and Protection Commons Salmon, Terrell P., "OPENING REMARKS—TWELFTH VERTEBRATE PEST CONFERENCE" (1986). Proceedings of the Twelfth Vertebrate Pest Conference (1986). 1. https://digitalcommons.unl.edu/vpc12/1 This Article is brought to you for free and open access by the Vertebrate Pest Conference Proceedings collection at DigitalCommons@University of Nebraska - Lincoln. It has been accepted for inclusion in Proceedings of the Twelfth Vertebrate Pest Conference (1986) by an authorized administrator of DigitalCommons@University of Nebraska - Lincoln. OPENING REMARKS—TWELFTH VERTEBRATE PEST CONFERENCE TERRELL P. SALMON, Wildlife Specialist, Cooperative Extension, University of California, Davis, California 95616. On behalf of the Vertebrate Pest Council, welcome to the 12th Vertebrate Pest Conference. Every other year since 1962, the Vertebrate Pest Council has sponsored the conference with the primary objective of bringing individuals interested in vertebrate pest control together to discuss problems and solutions of mutual concern. The main objectives of the conference are: 1. To exchange information on vertebrate pest management and related matters. 2. To advance environmentally safe vertebrate pest management methodologies. 3. To build cooperation with public and private agencies in solving vertebrate pest problems. 4. To consider and promote discussion and interaction among agencies and others about problems of mutual concern in the field of vertebrate pest management. -

Defense Intelligence Agency (DIA) Freedom of Information Act Log, Oct 1, 2012 - Dec 15, 2012
Description of document: Defense Intelligence Agency (DIA) Freedom of Information Act log, Oct 1, 2012 - Dec 15, 2012 Requested date: December 2012 Release date: September 2013 Posted date: 14-September-2020 Source of document: Defense Intelligence Agency ATTN: FAC2C (FOIA) 7400 Pentagon Washington, DC 20301-7400 Online FOIA Request Form The governmentattic.org web site (“the site”) is a First Amendment free speech web site, and is noncommercial and free to the public. The site and materials made available on the site, such as this file, are for reference only. The governmentattic.org web site and its principals have made every effort to make this information as complete and as accurate as possible, however, there may be mistakes and omissions, both typographical and in content. The governmentattic.org web site and its principals shall have neither liability nor responsibility to any person or entity with respect to any loss or damage caused, or alleged to have been caused, directly or indirectly, by the information provided on the governmentattic.org web site or in this file. The public records published on the site were obtained from government agencies using proper legal channels. Each document is identified as to the source. Any concerns about the contents of the site should be directed to the agency originating the document in question. GovernmentAttic.org is not responsible for the contents of documents published on the website. OIAFOIALog 10/1/12 - 12/15/12 Request ID Req'-"•r Name Request DeiCriptlon Request Type FO!A-00001-2013 Slaughter, Keisha Requesting all documents regarding the Oct. -

11 July 2006 Mumbai Train Bombings
11 July 2006 Mumbai train bombings July 2006 Mumbai train bombings One of the bomb-damaged coaches Location Mumbai, India Target(s) Mumbai Suburban Railway Date 11 July 2006 18:24 – 18:35 (UTC+5.5) Attack Type Bombings Fatalities 209 Injuries 714 Perpetrator(s) Terrorist outfits—Student Islamic Movement of India (SIMI), Lashkar-e-Toiba (LeT; These are alleged perperators as legal proceedings have not yet taken place.) Map showing the 'Western line' and blast locations. The 11 July 2006 Mumbai train bombings were a series of seven bomb blasts that took place over a period of 11 minutes on the Suburban Railway in Mumbai (formerly known as Bombay), capital city of the Indian state of Maharashtra and India's financial capital. 209 people lost their lives and over 700 were injured in the attacks. Details The bombs were placed on trains plying on the western line of the suburban ("local") train network, which forms the backbone of the city's transport network. The first blast reportedly took place at 18:24 IST (12:54 UTC), and the explosions continued for approximately eleven minutes, until 18:35, during the after-work rush hour. All the bombs had been placed in the first-class "general" compartments (some compartments are reserved for women, called "ladies" compartments) of several trains running from Churchgate, the city-centre end of the western railway line, to the western suburbs of the city. They exploded at or in the near vicinity of the suburban railway stations of Matunga Road, Mahim, Bandra, Khar Road, Jogeshwari, Bhayandar and Borivali. -
The Lockerbie Terrorist Attack and Libya: a Retrospective Analysis Steve Emerson
Case Western Reserve Journal of International Law Volume 36 | Issue 2 2004 The Lockerbie Terrorist Attack and Libya: A Retrospective Analysis Steve Emerson Follow this and additional works at: https://scholarlycommons.law.case.edu/jil Part of the International Law Commons Recommended Citation Steve Emerson, The Lockerbie Terrorist Attack and Libya: A Retrospective Analysis, 36 Case W. Res. J. Int'l L. 487 (2004) Available at: https://scholarlycommons.law.case.edu/jil/vol36/iss2/13 This Article is brought to you for free and open access by the Student Journals at Case Western Reserve University School of Law Scholarly Commons. It has been accepted for inclusion in Case Western Reserve Journal of International Law by an authorized administrator of Case Western Reserve University School of Law Scholarly Commons. THE LOCKERBIE TERRORIST ATTACK AND LIBYA: A RETROSPECTIVE ANALYSIS* Steve Emersont Following the horrific terrorist crime that saw Pan Am flight 103 literally blown out of the sky, an incredible journey of forensic investigations and intelligence began that ultimately resulted in a momentous court verdict in 2001. The forensic investigation alone into Pan Am 103, was one of the most intense, meticulous and expensive criminal investigations ever undertaken. As many will recall, the initial theory was that Iran had effectively "subcontracted" this murderous project to Syria and Libya in retaliation for the U.S. downing of an Iranian jet. In fact, in the months before the Pan Am 103 bombing, a Syrian cell possessing barometric bombs had been arrested in Frankfurt. It was thought at the time that these bombs were to be placed on aircraft departing from Frankfurt to Britain. -

The New National Boatmasters' Licence
House of Commons Transport Committee The new National Boatmasters’ Licence Sixth Report of Session 2006–07 Volume II Oral and written evidence Ordered by The House of Commons to be printed 16 May 2007 HC 320-II Published on 25 May 2007 by authority of the House of Commons London: The Stationery Office Limited £16.50 The Transport Committee The Transport Committee is appointed by the House of Commons to examine the expenditure, administration and policy of the Department for Transport and its associated public bodies. Current membership Mrs Gwyneth Dunwoody MP (Labour, Crewe and Nantwich) (Chairman) Mr David Clelland MP (Labour, Tyne Bridge) Mr Jeffrey M Donaldson MP (Democratic Unionist, Lagan Valley) Clive Efford MP (Labour, Eltham) Mrs Louise Ellman MP (Labour/Co-operative, Liverpool Riverside) Mr Philip Hollobone MP (Conservative, Kettering) Mr John Leech MP (Liberal Democrat, Manchester, Withington) Mr Eric Martlew MP (Labour, Carlisle) Mr Lee Scott MP (Conservative, Ilford North) Mr Graham Stringer MP (Labour, Manchester Blackley) Mr David Wilshire MP (Conservative, Spelthorne) Powers The Committee is one of the departmental select committees, the powers of which are set out in House of Commons Standing Orders, principally in SO No 152. These are available on the Internet via www.parliament.uk. Publications The Reports and evidence of the Committee are published by The Stationery Office by Order of the House. All publications of the Committee (including press notices) are on the Internet at www.parliament.uk/transcom. A list of reports of the Committee for the current session is at the back of this Report. Committee staff The current staff of the Committee are Tom Healey (Clerk), Annette Toft (Second Clerk), Clare Maltby (Committee Specialist), Louise Butcher (Inquiry Manager), Alison Mara (Committee Assistant), Ronnie Jefferson (Secretary), Jim Lawford (Senior Office Clerk) and Laura Kibby (Media Officer). -

Tidal Thames Water Safety Forum
Tidal Thames Water Safety Forum Drowning Prevention Strategy: Accidental and Self Harm TIDAL THAMES WATER SAFETY FORUM Drowning Prevention Strategy May 2019 TIDAL THAMES WATER SAFETY FORUM Foreword 1. Background p2 I am delighted to support the Tidal Foreword p3 Thames Water Safety Forum which brings 1. Background together vital agencies across maritime, 1.1 Membership p4 coastal and emergency services to keep 1.2 Scope p4 the tidal Thames safe for everyone. Our aim is to reduce the number of avoidable 1.3 The London picture p4 deaths from drowning in the tidal 1.4 Rising suicide rates p7 Thames targeting a ‘zero harm’ policy. Stretching 95 miles from Teddington in 1.5 Coping with London’s growth p7 the west to the North Sea in the east, the 1.6 The case for community p9 tidal Thames is the UK’s busiest waterway, used all year round by safety commercial and recreational vessels alike. It is iconic and its bridges are known the world over. 2. Strategic objectives p10 In 2018, 30 people drowned in the river, accounting for 8% of 2.1 Overview p11 drowning-related deaths nationally. Over the year, there were 688 recorded cases of people threatening to enter the Thames to take 2.2 Raising awareness p11 their life. 105 people actually entered the water, triggering 2.3 Tackle river-related suicide p12 interventions by the emergency services. As Minister for suicide and self-harm drownings prevention I see all these incidents as preventable. I am determined that we make our public areas safe and put in place 2.4 Implement a robust, multi- p15 appropriate measures to reduce risk. -
How to Build a Nuclear Bomb and Other Weapons of Mass Destruction
Frank Barnaby is a nuclear physicist by training. He worked at the Atomic Weapons Research Establishment, Aldermaston and University College, London. He was Director of the Stockholm International Peace Research Institute (SIPRI) from 1971 to 1981 and Guest Professor at the Free University, Amsterdam. He currently works for the Oxford Research Group on research into military technology, civil and military nuclear issues, and the terrorist use of weapons of mass destruction. How to Build a Nuclear Bomb and other weapons of mass destruction FRANK BARNABY For Wendy, Sophie, and Ben How To BUILD A NUCLEAR BOMB and Other Weapons of Mass Destruction Copyright © 2004 by Frank Barnaby Published by Nation Books An Imprint of Avalon Publishing Group Incorporated 245 West 17th St., 11th Floor New York, NY 10011 Nation Books is a co-publishing venture of the Nation Institute and Avalon Publishing Group Incorporated. All rights reserved. No part of this publication may be repro- duced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system now known or to be invented, with- out permission in writing from the publisher, except by a reviewer who wishes to quote brief passages in connection with a review written for inclusion in a magazine, newspaper, or broadcast. Library of Congress Cataloging-in-Publication Data is available. ISBN 1-56025-603-6 987654321 Printed in the United States of America Distributed by Publishers Group West Contents Preface to US edition -

Congressional Record United States Th of America PROCEEDINGS and DEBATES of the 112 CONGRESS, FIRST SESSION
E PL UR UM IB N U U S Congressional Record United States th of America PROCEEDINGS AND DEBATES OF THE 112 CONGRESS, FIRST SESSION Vol. 157 WASHINGTON, FRIDAY, JUNE 24, 2011 No. 92 Senate The Senate was not in session today. Its next meeting will be held on Monday, June 27, 2011, at 2 p.m. House of Representatives FRIDAY, JUNE 24, 2011 The House met at 9 a.m. and was Pursuant to clause 1, rule I, the Jour- in restraint on the President, and this called to order by the Speaker. nal stands approved. is where I disagree. I believe the word- f f ing is different. It says no funds for ground troops. But then it has excep- PRAYER PLEDGE OF ALLEGIANCE tions, and the exceptions are for all the The Chaplain, the Reverend Patrick The SPEAKER. Will the gentleman things that we’re already doing. So I J. Conroy, offered the following prayer: from Mississippi (Mr. NUNNELEE) come believe if we vote and pass the second Eternal God, we give You thanks for forward and lead the House in the one, it will be the first time this Con- giving us another day. We pause in Pledge of Allegiance. gress has given authority to the Presi- Your presence and ask guidance for the Mr. NUNNELEE led the Pledge of Al- dent for what he is doing right now. men and women of the people’s House. legiance as follows: So I urge my colleagues to look at Enable them, O God, to act on what I pledge allegiance to the Flag of the both of these carefully. -
Table of Contents
THE CAPE Military Space Operations 1971-1992 by Mark C. Cleary 45th Space Wing History Office Table of Contents Preface Chapter I -USAF Space Organizations and Programs Table of Contents Section 1 - Air Force Systems Command and Subordinate Space Agencies at Cape Canaveral Section 2 - The Creation of Air Force Space Command and Transfer of Air Force Space Resources Section 3 - Defense Department Involvement in the Space Shuttle Section 4 - Air Force Space Launch Vehicles: SCOUT, THOR, ATLAS and TITAN Section 5 - Early Space Shuttle Flights Section 6 - Origins of the TITAN IV Program Section 7 - Development of the ATLAS II and DELTA II Launch Vehicles and the TITAN IV/CENTAUR Upper Stage Section 8 - Space Shuttle Support of Military Payloads Section 9 - U.S. and Soviet Military Space Competition in the 1970s and 1980s Chapter II - TITAN and Shuttle Military Space Operations Section 1 - 6555th Aerospace Test Group Responsibilities Section 2 - Launch Squadron Supervision of Military Space Operations in the 1990s Section 3 - TITAN IV Launch Contractors and Eastern Range Support Contractors Section 4 - Quality Assurance and Payload Processing Agencies Section 5 - TITAN IIIC Military Space Missions after 1970 Section 6 - TITAN 34D Military Space Operations and Facilities at the Cape Section 7 - TITAN IV Program Activation and Completion of the TITAN 34D Program Section 8 - TITAN IV Operations after First Launch Section 9 - Space Shuttle Military Missions Chapter III - Medium and Light Military Space Operations Section 1 - Medium Launch Vehicle and Payload Operations Section 2 - Evolution of the NAVSTAR Global Positioning System and Development of the DELTA II Section 3 - DELTA II Processing and Flight Features Section 4 - NAVSTAR II Global Positioning System Missions Section 5 - Strategic Defense Initiative Missions and the NATO IVA Mission Section 6 - ATLAS/CENTAUR Missions at the Cape Section 7 - Modification of Cape Facilities for ATLAS II/CENTAUR Operations Section 8 - ATLAS II/CENTAUR Missions Section 9 - STARBIRD and RED TIGRESS Operations Section 10 - U.S. -

MRC News July Issue9
9 E U S S I N C O R P O R A T I N G M R C N E W S I T H E O F F I C I A L M A G A Z I N E F O R M O U N T A I N R E S C U E I N E N G L A N D , W A L E S & I R E L A N D JJ UU LL YY 22 00 00 44 AA WWAALLKK IINN TTHHEE WWOOOODDSS SSeeaarrcchhiinngg ffoorr ssaallaammaannddeerrss iinn tthhee BBlluuee RRiiddggee MMoouunnttaaiinnss WWHHAATT AA LLOONNGG SSTTRRAANNGGEE TTRRIIPP IITT’’SS BBEEEENN...... BBiillll BBaattssoonn bboowwss oouutt DDIIVVIINNGG EEMMEERRGGEENNCCIIEESS AANNDD CCAAVVEE RREESSCCUUEE AAddvviiccee ffoorr mmoouunnttaaiinn rreessccuueerrss PPlluuss NNEEWWSS && VVIIEEWWSS FFRROOMM TTHHEE MMRRCC AANNDD AARROOUUNNDD TTHHEE RREEGGIIOONNSS wwwwww..mmoouunnttaaiinn..rreessccuuee..oorrgg..uukk £2.50 ...A WORD reactive, fire-fighting issues, or even having I N C O R P O R A T I N G M R C N E W S FROM THE directives imposed upon us. E D I T O R I A L I wrote a short piece in a previous edition TOP TABLE... about the formation of the new Duddon and Editor Furness team. The process of amalgamation, the Judy Whiteside thinking about the future, and review of systems Years ago, when I was approached by Rossendale & Pendle MRT and operating procedures has convinced me that Stewart Hulse and David Allan to stand as 8 bridgefoot close . boothstown . worsley many other teams might benefit from a similar manchester M28 1UG Equipment Officer, taking over from Joe Walmsley, process, should look with a hard critical eye at the telephone 0161 702 6080 little did I realise what I was taking on! I can still future, and look and think outside the box. -

View on Contactpoint Carried out by Secondary Schools
Monday Volume 497 12 October 2009 No. 121 HOUSE OF COMMONS OFFICIAL REPORT PARLIAMENTARY DEBATES (HANSARD) Monday 12 October 2009 £5·00 © Parliamentary Copyright House of Commons 2009 This publication may be reproduced under the terms of the Parliamentary Click-Use Licence, available online through the Office of Public Sector Information website at www.opsi.gov.uk/click-use/ Enquiries to the Office of Public Sector Information, Kew, Richmond, Surrey TW9 4DU; e-mail: [email protected] HER MAJESTY’S GOVERNMENT MEMBERS OF THE CABINET (FORMED BY THE RT.HON.GORDON BROWN,MP,JUNE 2007) PRIME MINISTER,FIRST LORD OF THE TREASURY AND MINISTER FOR THE CIVIL SERVICE—The Rt. Hon. Gordon Brown, MP LEADER OF THE HOUSE OF COMMONS,LORD PRIVY SEAL AND MINISTER FOR WOMEN AND EQUALITY—The Rt. Hon. Harriet Harman, QC, MP FIRST SECRETARY OF STATE,SECRETARY OF STATE FOR BUSINESS,INNOVATION AND SKILLS AND LORD PRESIDENT OF THE COUNCIL—The Rt. Hon. The Lord Mandelson CHANCELLOR OF THE EXCHEQUER—The Rt. Hon. Alistair Darling, MP SECRETARY OF STATE FOR FOREIGN AND COMMONWEALTH AFFAIRS—The Rt. Hon. David Miliband, MP SECRETARY OF STATE FOR JUSTICE AND LORD CHANCELLOR—The Rt. Hon. Jack Straw, MP SECRETARY OF STATE FOR THE HOME DEPARTMENT—The Rt. Hon. Alan Johnson, MP SECRETARY OF STATE FOR ENVIRONMENT,FOOD AND RURAL AFFAIRS—The Rt. Hon. Hilary Benn, MP SECRETARY OF STATE FOR INTERNATIONAL DEVELOPMENT—The Rt. Hon. Douglas Alexander, MP SECRETARY OF STATE FOR COMMUNITIES AND LOCAL GOVERNMENT—The Rt. Hon. John Denham, MP SECRETARY OF STATE FOR CHILDREN,SCHOOLS AND FAMILIES—The Rt.