Proctocolitis from Coffee Enema
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Progress of Research of Hyperthermia Integration with TCM in the Treatment of Cancer
Oncothermia Journal 7:36-42 (2013) Progress of research of hyperthermia integration with TCM in the treatment of cancer Prof. Dr. Clifford L.K. Pang1 (1) Clifford Hospital, 8 Shiguang Road, Panyu, Guangzhou, Guangdong Province, China Corresponding author: cpang@ Oncothermia Journal, June 2013 35 Progress of research of hyperthermia integration with TCM in the treatment of cancer With the development of clinical oncotherapies, integrative treatments have generally been recognized by the Oncology Association. Hyperthermia has proven its effectiveness in the treatment of cancer which is different from surgery, radiotherapy, chemotherapy and biotherapy. Besides integration with the above therapies, using this with TCM is a unique approach. The progress of research of hyperthermia integration with TCM in treating cancer will be presented according to the following six aspects:l 1. The advantages of hyperthermia in the treatment of cancer 2. The advantages of TCM in treating cancer 3. The advantages of hyperthermia in combination with TCM 4. An overview of the implementation of hyperthermia integration with TCM in treating cancer in Clifford Hospital 5. Clinical report of integrative therapy 6. The future of hyperthermia integration with TCM in treating cancer 1. The advantages of hyperthermia in treating cancer 1.1. Hyperthermia is part of the field of Natural Medicine. It targets cancer cells directly, improves the immune system, induces apoptosis of cancer cells, suppresses the formation of cancer vessels, destroys cancer vessels, and relieves pain caused by cancer. At the same time, hyperthermia has demonstrated no damage to normal tissue. 1.2. Hyperthermia can be utilized in conjunction with other cancer therapies and integrated into a comprehensive anti-cancer protocol. -

Gastroenterology and the Elderly
3 Gastroenterology and the Elderly Thomas W. Sheehy 3.1. Esophagus 3.1.1. Dysphagia Esophageal disorders, such as esophageal motility disorders, infections, tumors, and other diseases, are common in the elderly. In the elderly, dysphagia usually implies organic disease. There are two types: (1) pre-esophageal and (2) esophageal. Both are further subdivided into motor (neuromuscular) or structural (intrinsic and extrinsic) lesions.! 3.1.2. Pre-esophageal Dysphagia Pre-esophageal dysphagia (PED) usually implies neuromuscular disease and may be caused by pseudobular palsy, multiple sclerosis, amy trophic lateral scle rosis, Parkinson's disease, bulbar poliomyelitis, lesions of the glossopharyngeal nerve, myasthenia gravis, and muscular dystrophies. Since PED is due to inability to initiate the swallowing mechanism, food cannot escape from the oropharynx into the esophagus. Such patients usually have more difficulty swallowing liquid THOMAS W. SHEEHY • The University of Alabama in Birmingham, School of Medicine, Department of Medicine; and Medical Services, Veterans Administration Medical Center, Birming ham, Alabama 35233. 87 S. R. Gambert (ed.), Contemporary Geriatric Medicine © Plenum Publishing Corporation 1983 88 THOMAS W. SHEEHY than solids. They sputter or cough during attempts to swallow and often have nasal regurgitation or aspiration of food. 3.1.3. Dysfunction of the Cricopharyngeus Muscle In the elderly, this is one of the more common forms of PED.2 These patients have the sensation of an obstruction in their throat when they attempt to swallow. This is due to incoordination of the cricopharyngeus muscle. When this muscle fails to relax quickly enough during swallowing, food cannot pass freely into the esophagus. If the muscle relaxes promptly but closes too quickly, food is trapped as it attempts to enter the esophagus. -

CDHO Factsheet Ulcerative Colitis
Disease/Medical Condition ULCERATIVE COLITIS Date of Publication: June 14, 2013 (also referred to as “UC”, “idiopathic proctocolitis”, “pancolitis”, and “inflammatory bowel disease” [IBD]; IBD is an umbrella term that also includes Crohn’s disease and indeterminate/undifferentiated IBD) Is the initiation of non-invasive dental hygiene procedures* contra-indicated? No Is medical consult advised? ...................................... No (assuming patient/client is already under medical care for ulcerative colitis). Is the initiation of invasive dental hygiene procedures contra-indicated?** Possibly, but not typically Is medical consult advised? ....................................... Possibly (depends on severity and level of control of the disease, including the presence/absence of oral lesions). Is medical clearance required? .................................. Possibly (e.g., if the disease is unstable — flare-up — and/or there are active oral lesions). Also, medical clearance may be required if patient/client is being treated with medications associated with immunosuppression +/- increased risk of infection (e.g., corticosteroids [e.g., prednisone], azathioprine, 6-mercaptopurine, methotrexate, cyclosporine, sulfasalazine, biologic response modifier drugs [e.g., anti-tumour necrosis factor drugs — anti-TNFs — such as infliximab, adalimumab, certoluzimab, and golimumab, as well as monoclonal antibody drugs such as vedoluzimab], JAK1 inhibitors [e.g., tofacitinib], etc.). Is antibiotic prophylaxis required? ............................. -

Detoxification Protocol
Dr. Joel Cone/Dr. Alexis Dobson www.diagnosticnaturalmedicine.com (512) 577-7234 Detoxification Protocol Periodic detoxification makes sense in keeping your body as fine tuned and healthy as possible. We know many disease states, including heart disease, cancer, and chronic inflammatory disease states have a strong correlation with diet, lifestyle, and environmental factors. There are many different cleanse ideas, but if we start with the knowledge of the anatomy and physiology of the body we can make the best approach to a detoxification process possible. We know that there are several systems by which toxins and waste products are eliminated through the body. By having knowledge of these systems we can increase our ability to aggressively detoxify our body. There are four major detoxification systems our body uses. The first is the respiratory system which eliminates gaseous waste products such as carbon dioxide, a waste by product of glucose metabolism. Another system is the integumentary system, in which lactic acid and various other wastes are removed. We also use the digestive system, especially the hepatobiliary system to remove some cholesterol, bile secretions, and other toxins bound in bile. The liver is also the primary congugator of metabolic toxins into water soluble products which can be sent to the kidney for removal. The remaining system is the renal system, in which the kidney removed nitrogenous wastes, including urea, ammonia, creatinine, and other drug metabolites from the body. I have also added the lymphatic and circulatory system as an elimination component, as they play a crucial role in the mobilization of compounds that need to be removed from the body. -

COFFEE ENEMAS by Dr
COFFEE ENEMAS By Dr. Lawrence Wilson © April 2016, The Center For Development All information in this article is for educational purposes only. It is not for the diagnosis, treatment, prescription or cure of any disease or health condition. Click here to go directly to the coffee enema procedure. To read a short version of this article in Greek, click here. CONTENTS OF THIS ARTICLE 1. Introduction What Is A Coffee Enema? Why Coffee Enemas? History Of Coffee Enemas Dr. Gerson, Dr. Kelley, Dr. Gonzales, And Others 2. Coffee, A Remarkable Herb What Is Coffee? Growing And Processing Of Coffee The Best Coffee For Coffee Enemas Coffee As A Beverage 3. Effects Of Coffee Enemas Effects Of Coffee Enemas On The Colon Effects Elsewhere 4. Equipment Used For Coffee Enemas Enema Buckets – Plastic And Stainless Steel Enema Bags – Open And Closed Fleet Enema Bottles Enema Nozzles Colon Tubes Colonic Irrigation Machines 5. The Coffee Enema Procedure Safety First Step 1. Decide Where To Do Your Coffee Cleanse Step 2. Gathering The Materials Step 3. Preparing The Coffee Step 4. Preparing To Take The Enema Step 5. Doing The Enema Step 6. Clean Up When To Do Your Enema What To Do While Retaining Your Enema How Often? For How Long? What If You Are Ill? 6. Cautions And Troubleshooting Cautions Troubleshooting 7. Controversy And Myths About Coffee Enemas 8. A Total Healing Program With Coffee Enemas General Dietary Suggestions Food Supplements Other 9. Therapies Related To Coffee Enemas The Vaginal Coffee Implant The Penis Coffee Implant Other Therapeutic Uses Of Coffee Colonic Irrigation Enemas With Other Substances Rectal Ozone After Your Enema Herbs For The Colon And The Liver 10. -

Advice Note: Infant Proctocolitis – Fresh Blood PR in a Thriving Infant
Advice Note: Infant proctocolitis – Fresh blood PR in a thriving infant Dear GP, Thank you for your referral. The most common cause for small amounts of fresh blood PR in a well, thriving infant is infant proctocolitis. This is a benign condition in vast majority of cases and does not require a secondary care input. This is a food protein related reaction most commonly caused by cow’s milk protein (CMP) but other common causes include soy, egg, corn and cereal grains. Rarely other foods can trigger a reaction. Typically infants can tolerate the previously causative proteins by 1 year of age. It does not increase the risk of IgE mediated food allergy. It is common in both breast and formula fed babies. There are no diagnostic tests and the diagnosis relies on exclusion of other causes and resolution of symptoms with dietary manipulations. Features of a typical presentation include: Mucousy loose stools with spots or streaks of bright red blood in a well thriving infant Age at presentation: 1 week to 5 months (although can present earlier and later) It can be associated with mild to moderate diarrhea, excessive crying / fussiness/ sleep disturbance, apparent pain on defecation. It may also be associated with mild anemia, hypoalbuminaemia, mild peripheral eosinophilia and family history of same. Features indicating other disorders include: No IM vitamin K at birth Severe bleeding Abdominal distension / tenderness on examination Faltering growth Signs / symptoms of malabsorption Severe diarrhea Vomiting Anaphylaxis Rash, including petechiae, purpura or urticarial Significant anaemia Persistent perianal dermatitis Anal fissures Management: Referral to ED if the infant : o is unwell and or febrile o is haemodynamically unstable o has a history of severe bleeding o has significant vomiting o has abdominal distension or tenderness on examination o has features of anaphylaxis o has severe anaemia Management in the community if the child is well and there are no worrying features on history or examination: o Investigations: . -
Diagnostic Codes
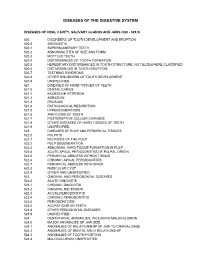
DISEASES OF THE DIGESTIVE SYSTEM DISEASES OF ORAL CAVITY, SALIVARY GLANDS AND JAWS (520 - 529.9) 520 DISORDERS OF TOOTH DEVELOPMENT AND ERUPTION 520.0 ANODONTIA 520.1 SUPERNUMERARY TEETH 520.2 ABNORMALITIES OF SIZE AND FORM 520.3 MOTTLED TEETH 520.4 DISTURBANCES OF TOOTH FORMATION 520.5 HEREDITARY DISTURBANCES IN TOOTH STRUCTURE, NOT ELSEWHERE CLASSIFIED 520.6 DISTURBANCES IN TOOTH ERUPTION 520.7 TEETHING SYNDROME 520.8 OTHER DISORDERS OF TOOTH DEVELOPMENT 520.9 UNSPECIFIED 521 DISEASES OF HARD TISSUES OF TEETH 521.0 DENTAL CARIES 521.1 EXCESSIVE ATTRITION 521.2 ABRASION 521.3 EROSION 521.4 PATHOLOGICAL RESORPTION 521.5 HYPERCEMENTOSIS 521.6 ANKYLOSIS OF TEETH 521.7 POSTERUPTIVE COLOUR CHANGES 521.8 OTHER DISEASES OF HARD TISSUES OF TEETH 521.9 UNSPECIFIED 522 DISEASES OF PULP AND PERIAPICAL TISSUES 522.0 PULPITIS 522.1 NECROSIS OF THE PULP 522.2 PULP DEGENERATION 522.3 ABNORMAL HARD TISSUE FORMATION IN PULP 522.4 ACUTE APICAL PERIODONTITIS OF PULPAL ORIGIN 522.5 PERIAPICAL ABSCESS WITHOUT SINUS 522.6 CHRONIC APICAL PERIODONTITIS 522.7 PERIAPICAL ABSCESS WITH SINUS 522.8 RADICULAR CYST 522.9 OTHER AND UNSPECIFIED 523 GINGIVAL AND PERIODONTAL DISEASES 523.0 ACUTE GINGIVITIS 523.1 CHRONIC GINGIVITIS 523.2 GINGIVAL RECESSION 523.3 ACUTE PERIODONTITIS 523.4 CHRONIC PERIODONTITIS 523.5 PERIODONTOSIS 523.6 ACCRETIONS ON TEETH 523.8 OTHER PERIODONTAL DISEASES 523.9 UNSPECIFIED 524 DENTOFACIAL ANOMALIES, INCLUDING MALOCCLUSION 524.0 MAJOR ANOMALIES OF JAW SIZE 524.1 ANOMALIES OF RELATIONSHIP OF JAW TO CRANIAL BASE 524.2 ANOMALIES OF DENTAL ARCH -

Choosing HEALTH
“Natural forces are the healers of disease.” Hippocrates choosing By Choosing HEALTH – choosing • Know precisely how to heal your body to be symptom free, robust and vital • Distinguish all of the lifestyle elements that restore, protect and enhance your health • Discover how proper diet, exercise, rest and relaxation can improve your energy and well-bHEALTH HEAHEALLTHTH Interpret questionnaires, home tests and read your own lab work Learn how to harness natural forces to know how each system of your body functions Understand with certainty the exact the cause of your symptoms or illnesses to restore, protect and enhance your health Validate the results of your selfcare by actually measuring the improvements in your health Dr. Force’s Functional Selfcare Workbook Force’s Dr. Take control of your own health now and for the future Doctor Force has been practicing natural health care since 1984 and has always been a strong advocate for people being in control of their own health. His focus in practice is the diagnoses and treatment of complex and chronic illnesses. He has published numerous professional papers, been a technical contributor to manuals on laboratory diagnosis and clinical nutrition, taught diagnostics and natural therapies to physicians, and aided nutritional manufacturers in developing nutritional formulas. U.S. $29.95 Dr. Force’s Functional Selfcare Workbook choosing HEALTH Dr. Forces Functional Selfcare Workbook © 2003 Mark Force, D.C. All rights reserved. Printed in the United States of America The Elements of Health 233 Fourth Street Ashland, Oregon 97520 © 2003 Mark Force, D.C. No part of this workbook may be reproduced in any manner whatsoever without written permission except: H Forms from the CD may This workbook is not for the treatment or cure of any disease. -

Together Against Cancer
1 Together Against Cancer Newsletter Issue 2 August 2017 Welcome to our Second edition! We’ve been super busy at our Education and Wellness Centre recently. Amongst planning our 1st birthday party and holding Very educational, left more workshops and therapy sessions, we’ve also been putting inspired to spread together something brand new and exciting for November, so the knowledge and watch this space ! gain some more. The Education and Wellness Centre is open Monday to Friday offering information and advice. We also hold a good selection - Anon of reference books for you to browse through—just pop in, we’re Comment from recent Nutrition for Life Workshop always happy to see new faces. WIN a Tropic Ocean Fizz Foot Soak: See Page 5 for details and how to enter! In This Issue: Reiki TAC 1st Birthday • Feature Article ‘What Aromatherapy is Reiki? by Natalya Celebrations Kotadia Pg 1 Access Bars Come and join our 1st birthday celebrations • Steve’s Insight on Sunday 15th October 2017. Swedish Massage ‘Coffee Enemas’ Pg 3 Starting at 10am till 4 pm. Reflexology • Mel’s Meals Autumn Recipe Pg 5 Talks, Therapy sessions & much more… Life Alignment • Book of the moment Unit S1 Troon way business centre, Crystal Healing Pg 5 Humberstone Lane,Leicester,LE4 9HA. Nutritional Counselling • Upcoming Work- All welcome. EFT shops & Events Pg 5 Inner Dance 2 WHAT IS REIKI? BY NATALYA KOTADIA Reiki as defined by the Oxford English dictionary is: “A healing technique based on the principle that the therapist can channel energy into the patient by means of touch, to activate the natural healing processes of the patient’s body and restore physical and emotional well-being”. -

The British Society of Gastroenterology
Gut: first published as 10.1136/gut.16.10.821 on 1 October 1975. Downloaded from Gut, 1975, 16, 821-845 The British Society of Gastroenterology The 36th annual meeting was held in Oxford on 25-27 September under the Presidency of Dr S. C. Truelove. The meeting proper was preceded by a teaching day on 24 September when there were two sessions, one on liver disease (Chairman: Dr J. Badenoch), and the other on gastrointestinal disorders (Chairman: Sir Francis Avery Jones). There were 14 sessions each allocated to a different subject, and in addition there was a plenary session and panel discussion on 'The management of ulcerative colitis'. The Sir Arthur Hurst Memorial Lecture, 'Towards an artificial liver', was given on this occasion by Dr Roger Williams. Abstracts of the scientific papers follow and a more general report of the meeting and of the social events can be found on page 846. Distribution of gut hormones monkeys though some variation in total influx mechanism is inhibited by cAMP, amount was seen due to different organ this model also satisfies the paradoxical S. R. BLOOM, M. G. BRYANT, AND J. M. weights. Immunocytochemical data on effect of bile acids in congenital chlor- POLAK (Departments of Medicine and hormone distribution were in substantial idorrhoea. Subsequently, a clinical trial Histochemistry, The Royal Postgraduate agreement. was done. Following oral administration Medical School, Hammersmith Hospital, These hormone maps provide baseline of coated theophylline the frequency and London) Although several new gut hor- data for physiological studies. the volume of the diarrhoeas decreased mones have recently been described there significantly. -

COFFEE ENEMAS by Dr
COFFEE ENEMAS By Dr. Lawrence Wilson © April 2016, L.D. Wilson Consultants, Inc. All information in this article is for educational purposes only. It is not for the diagnosis, treatment, prescription or cure of any disease or health condition. Click here to go directly to the coffee enema procedure. To read a short version of this article in Greek, click here. CONTENTS OF THIS ARTICLE 1. Introduction What Is A Coffee Enema? Why Coffee Enemas? History Of Coffee Enemas Dr. Gerson, Dr. Kelley, Dr. Gonzales, And Others 2. Coffee, A Remarkable Herb What Is Coffee? Growing And Processing Of Coffee The Best Coffee For Coffee Enemas Coffee As A Beverage 3. Effects Of Coffee Enemas Effects Of Coffee Enemas On The Colon Effects Elsewhere 4. Equipment Used For Coffee Enemas Enema Buckets – Plastic And Stainless Steel Enema Bags – Open And Closed Fleet Enema Bottles Enema Nozzles Colon Tubes Colonic Irrigation Machines 5. The Coffee Enema Procedure Safety First Step 1. Decide Where To Do Your Coffee Cleanse Step 2. Gathering The Materials Step 3. Preparing The Coffee Step 4. Preparing To Take The Enema Step 5. Doing The Enema Step 6. Clean Up When To Do Your Enema What To Do While Retaining Your Enema How Often? For How Long? What If You Are Ill? Page 1 of 37 6. Cautions And Troubleshooting Cautions Troubleshooting 7. Controversy And Myths About Coffee Enemas 8. A Total Healing Program With Coffee Enemas General Dietary Suggestions Food Supplements Other 9. Therapies Related To Coffee Enemas The Vaginal Coffee Implant The Penis Coffee Implant Other Therapeutic Uses Of Coffee Colonic Irrigation Enemas With Other Substances Rectal Ozone After Your Enema Herbs For The Colon And The Liver 10. -

IAOMT ACCREDITATION-- Checklist for Completing Unit 4: Clinical Nutrition and Heavy Metal Detoxification for Biological Dentistry
IAOMT ACCREDITATION-- Checklist for Completing Unit 4: Clinical Nutrition and Heavy Metal Detoxification for Biological Dentistry INTRODUCTION TO UNIT 4 Take the Unit 4 Pre-test. Click here to go to page 3. Read the “Clinical Nutrition for Biological Dentistry” article by Rehme. Click here to go to pages 4-19. REQUIRED (MANDATORY) CONTENT OF UNIT 4 Read the “Relationship between Vitamin D and Periodontal Pathology” article by Jagelaviciene et al. Click here to go to pages 20-27. View the IAOMT online learning video activity “Nutrition in Dentistry” at https://iaomt.org/nutrition-dentistry-video-activity. Click here to go to page 28. Read the “A Hypothetical Role for Vitamin K2 in the Endocrine and Exocrine Aspects of Dental Caries” article by Southward. Click here to go to pages 29-33. Read the “Heavy Metal Detoxification for Biological Dentistry” article by Kall and Just. Click here to go to pages 34-43. View the IAOMT online learning video activity “Mercury Detoxification” at https://iaomt.org/mercury-detoxification-video- activity. Click here to go to page 44. Continued on next page… Checklist for Unit 4; Page 1 Read “Chelation Therapy to Prevent Diabetes-associated Cardiovascular Events” by Diaz et al. article. Click here to go to pages 45-61. Read the “Integrative Medicine Approach To Peripheral Neuropathy- -Avoiding Pitfalls Of Ineffective Current Standards In Assessing Chronic Low-Grade Mercury Toxicity And Functional Musculoskeletal Lesions” article by Carter et al. Click here to go to pages 62-68. TEST FOR UNIT 4 Take the Post-Test for Unit 4 at https://www.cvent.com/d/pvq54h.