Bavarian Nordic, Inc. Study Protocol
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
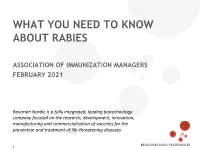
What You Need to Know About Rabies
WHAT YOU NEED TO KNOW ABOUT RABIES ASSOCIATION OF IMMUNIZATION MANAGERS FEBRUARY 2021 Bavarian Nordic is a fully integrated, leading biotechnology company focused on the research, development, innovation, manufacturing and commercialization of vaccines for the prevention and treatment of life-threatening diseases 1 VIRAL DISEASE ALMOST ALWAYS FATAL IF UNTREATED Paralytic rabies Ascending spread of flaccid Classical (furious) rabies Onset of coma DEATH muscle weakness, bilateral Hyper-excitability, periods weakness of facial muscles, of confusion, hallucinations, sphincter involvement agitation and hydrophobia Coma (0–14 days) Acute neurological phase (2–7 days) Nonspecific symptoms Fever, malaise, chills, fatigue, First neurological signs insomnia, anorexia, headache, (>10 days) anxiety, irritability Prodromal phase (2–10 days) Exposure Bite or scratch from, or Incubation of virus mucosal contact with, (20–90 days) a rabid animal 1. Jackson et al. In Rabies (2nd edition). Chapter 7. 2007: 309–340; 2. WHO. Wkly Epidemiol Rec 2018; 93: 201–20; 3. Hemachudha et al. Lancet Neurol 2002;1:101–9; 4. WHO. Rabies: Fact Sheet. https://www.who.int/en/news-room/fact-sheets/Detail/rabies [accesseD July 2020]. PREVALENCE IN THE USA Rabies transmission in dogs has been virtually eliminated in the USA, in part due to widespread canine vaccination programs5 • As a result, wildlife has accounted for >90% of rabid animals reported in the USA since 19805-7 • Primary vectors in this region are skunks, foxes, raccoons, bats and mongooses (in Puerto Rico)5-7 • In the US, the primary rabies vector is the bat due to encounters with bats that may be less recognized e.g. -

Valneva and Bavarian Nordic Announce Marketing and Distribution Partnership
VALNEVA SE Campus Bio-Ouest | 6, Rue Alain Bombard 44800 Saint-Herblain, France Valneva and Bavarian Nordic Announce Marketing and Distribution Partnership Saint-Herblain, France, June 18, 2020 – Valneva SE, (“Valneva”), a specialty vaccine company, and Bavarian Nordic A/S (OMX: BAVA) today announced that they have signed a binding term sheet to establish a partnership for the marketing and distribution of their commercial products. The partnership will provide both companies with additional critical mass, significant commercial synergies and a market leadership position in the specialty vaccine industry. Under the agreed terms, Valneva will commercialize Bavarian Nordic’s marketed vaccines leveraging its commercial infrastructure in Canada, UK, France and Austria. Valneva will also take responsibility for Belgium and the Netherlands where it will set up new commercial operations. Bavarian Nordic will commercialize Valneva’s marketed products in Germany and Switzerland. The partnership includes vaccines that protect against rabies, Japanese Encephalitis, tick-borne encephalitis and cholera. The agreement follows Bavarian Nordic’s recent acquisition of two commercial vaccines from GlaxoSmithKline. The transition from current arrangements will commence later this year and through 2021 in line with existing distribution agreements. Valneva expects limited additional revenues in 2020 with more material impact from 2021 onwards. Thomas Lingelbach, CEO of Valneva, commented, “We are excited to join forces with Bavarian Nordic to continue to build our commercial business and to enhance our product offering to our customers. This partnership provides excellent synergy for both companies as well as greater breadth in our commercial portfolios.” Paul Chaplin, President & CEO of Bavarian Nordic, added, “We are pleased to collaborate with Valneva in the ongoing commercialization of our business. -

Written Statement for Dr. Anthony Fauci, Director, NIAID
DEPARTMENT OF HEALTH AND HUMAN SERVICES NATIONAL INSTITUTES OF HEALTH The Role of the National Institute of Allergy and Infectious Diseases Research in Addressing Ebola Virus Disease Testimony before the House Foreign Affairs Committee Subcommittee on Africa, Global Health, Global Human Rights, and International Organizations Anthony S. Fauci, M.D. Director National Institute of Allergy and Infectious Diseases September 17, 2014 Mr. Chairman and Members of the Committee: Thank you for the opportunity to discuss the National Institutes of Health (NIH) response to the global health emergency of Ebola virus disease. I direct the National Institute of Allergy and Infectious Diseases (NIAID), the lead institute of the NIH for conducting and supporting research on infectious diseases, including viral hemorrhagic fevers such as those caused by Ebola virus infection. For over six decades, NIAID has made important contributions to advancing the understanding of infectious, immunologic, and allergic diseases, from basic research on mechanisms of disease to applied research to develop diagnostics, therapeutics, and vaccines. NIAID has a dual mandate that balances research addressing current biomedical challenges with the capacity to respond quickly to newly emerging and re-emerging infectious diseases, including bioterror threats. Critical to these efforts are NIAID’s partnerships with academia and pharmaceutical companies, and collaborations with other federal entities, particularly the Centers for Disease Control and Prevention, the Food and Drug Administration (FDA), the Biomedical Advanced Research and Development Authority (BARDA), and the Department of Defense. OVERVIEW OF EBOLA VIRUS DISEASE Viral hemorrhagic fevers are severe illnesses that can be fatal and are caused by a diverse group of viruses including Marburg virus, Lassa virus, and Ebola virus. -

Vaccinia Virus
APPENDIX 2 Vaccinia Virus • Accidental infection following transfer from the vac- cination site to another site (autoinoculation) or to Disease Agent: another person following intimate contact Likelihood of Secondary Transmission: • Vaccinia virus • Significant following direct contact Disease Agent Characteristics: At-Risk Populations: • Family: Poxviridae; Subfamily: Chordopoxvirinae; • Individuals receiving smallpox (vaccinia) vaccination Genus: Orthopoxvirus • Individuals who come in direct contact with vacci- • Virion morphology and size: Enveloped, biconcave nated persons core with two lateral bodies, brick-shaped to pleo- • Those at risk for more severe complications of infec- morphic virions, ~360 ¥ 270 ¥ 250 nm in size tion include the following: • Nucleic acid: Nonsegmented, linear, covalently ᭺ Immune-compromised persons including preg- closed, double-stranded DNA, 18.9-20.0 kb in length nant women • Physicochemical properties: Virus is inactivated at ᭺ Patients with atopy, especially those with eczema 60°C for 8 minutes, but antigen can withstand 100°C; ᭺ Patients with extensive exfoliative skin disease lyophilized virus maintains potency for 18 months at 4-6°C; virus may be stable when dried onto inanimate Vector and Reservoir Involved: surfaces; susceptible to 1% sodium hypochlorite, • No natural host 2% glutaraldehyde, and formaldehyde; disinfection of hands and environmental contamination with soap Blood Phase: and water are effective • Vaccinia DNA was detected by PCR in the blood in 6.5% of 77 military members from 1 to 3 weeks after Disease Name: smallpox (vaccinia) vaccination that resulted in a major skin reaction. • Progressive vaccinia (vaccinia necrosum or vaccinia • In the absence of complications after immunization, gangrenosum) recently published PCR and culture data suggest that • Generalized vaccinia viremia with current vaccines must be rare 3 weeks • Eczema vaccinatum after vaccination. -

Bavarian Nordic Annual Report 2018 Management Commentary | Financial Statements
Unlocking the power of the ANNUAL immune system REPORT 2018 199425 2019 YEARS OF GREAT ACHIEVEMENTS IN THE VACCINE SPACE STIMULATING THE IMMUNE SYSTEM GIVING HOPE TO MILLIONS Management commentary | Financial statements CONTENTS MANAGEMENT FINANCIAL COMMENTARY STATEMENTS INTRODUCTION BUSINESS AND PIPELINE CONSOLIDATED FINANCIAL STATEMENTS Letter from the CEO & chairman .................... 4 Product pipeline.................................. 20 Consolidated income statements .................. 68 At a glance ....................................... 6 Infectious disease ................................ 22 Consolidated statements of comprehensive 25 years of great achievements .................... 8 Our partnership with Janssen ...................... 28 income .......................................... 68 Key developments................................ 10 Cancer immunotherapy ........................... 36 Consolidated statements of cash flow.............. 69 A word from the new CFO......................... 12 Chordoma........................................ 38 Consolidated statements of financial position Strategy track ................................... .16 – assets ......................................... 70 Financial results for 2018 ......................... .18 CORPORATE INFORMATION Consolidated statements of financial position The Bavarian Nordic share ........................ .46 – equity/liabilities ............................... 71 Corporate social responsibility .................... .48 Consolidated statements of changes in -
Harnessing the Immune System to Prevent Cancer: Basic Immunologic Mechanisms & Their Application to Clinical Trials of Vaccines Part 2: the Vaccines Barbara K
Harnessing the Immune System to Prevent Cancer: Basic Immunologic Mechanisms & Their Application to Clinical Trials of Vaccines Part 2: The Vaccines Barbara K. Dunn NCI/Division of Cancer Prevention August 3, 2020 Harnessing the Immune System to Prevent Cancer: Basic Immunologic Mechanisms and Therapeutic Approaches that are Relevant to Cancer Prevention I. Basic immunologic mechanisms II. Application to prevention & treatment of cancer 1. Antibodies: as drugs 2. Vaccines: general principles & your vaccine trials & more… I) Vaccines to prevent cancers caused by infectious agents II) Vaccines to prevent non-infection associated cancer (directed toward tumor associated antigens) Harnessing the Immune System to Prevent Cancer: Basic Immunologic Mechanisms and Therapeutic Approaches that are Relevant to Cancer Prevention I. Basic immunologic mechanisms II. Application to prevention & treatment of cancer 1. Antibodies: as drugs “passive immunity” 2. Vaccines: general principles & your vaccine trials & more… I) Vaccines to prevent cancers caused by infectious agents “active II) Vaccines to prevent immunity” non-infection associated cancer (directed toward tumor associated antigens) Harnessing the Immune System to Prevent Cancer: Basic Immunologic Mechanisms and Therapeutic Approaches that are Relevant to Cancer Prevention I. Basic immunologic mechanisms II. Application to prevention & treatment of cancer 1. Antibodies:Focus as on drugs the Antigen “passive !immunity” 2. Vaccines: general principles & your vaccine trials & more… I) Vaccines -

The Tangible Effects of COVID-19 in Latin American Countries Boletín Del Colegio Mexicano De UROLOGIA´
Care and management in Urology oncology: The tangible effects of COVID-19 in Latin American countries Boletín del Colegio Mexicano de UROLOGIA´ BOLETÍN DEL COLEGIO MEXICANO DE UROLOGÍA, Vol. 36, año 2021, es una revista de publicación continua editada por el Colegio Mexicano de Urología Nacional, A.C., Montecito No. 38, Piso 33, Oficina 32, Col. Nápoles, C.P. 03810 CDMX, México. Tel. directo: (01-55) 9000-8053. http://www.cmu.org.mx Director: Dr. Héctor Berea Domínguez, Editor responsable: Dr. Erick Sierra Díaz, Co-Editores: Dr. Israel Presteguín Rosas, Dr. Rafael Sandoval Gómez, Asistente editorial: Lic. Angélica M. Arévalo Zacarías. Reservas de Derechos al Uso Exclusivo del título (04-2011-12081034400-106). ISNN: (0187-4829). Licitud de Título Núm. 016. Licitud de Contenido Núm. 008, de fecha 15 de agosto de 1979, ambos otorgados por la Comisión Clasifica- dora de Publicaciones y Revistas Ilustradas de la Secretaría de Gobernación. Los conceptos vertidos en los artículos publicados en este Bletín son responsabilidad exclusiva de los autores, y no reflejan necesariamente el criterio de el Colegio Mexicano de Urología Nacional, A.C. Este número se terminó de imprimir en abril de 2021. Publicación realizada, comercializada y distribuida por Edición y Farmacia SA de CV (Nieto Editores®). Cerrada de Antonio Maceo 68, colonia Escandón, 11800 Ciudad de México. Teléfono: 5678-2811. Queda estrictamente prohibida la reproducción total o parcial de los contenidos e imágenes de la publicación sin pevia auto- rización del Colegio Mexicano de Urología Nacional, A.C. Mesa Directiva 2019-2021 Dr. Ignacio López Caballero Presidente Dr. Héctor Raúl Vargas Zamora Vicepresidente Dr. -

Putting Into Perspective the Future of Cancer Vaccines: Targeted Immunotherapy
Putting into Perspective the Future of Cancer Vaccines: Targeted Immunotherapy Authors: Issam Makhoul,1,2 *Thomas Kieber-Emmons2,3 1. Department of Medicine, University of Arkansas for Medical Sciences, Little Rock, Arkansas, USA 2. Winthrop P. Rockefeller Cancer Institute, University of Arkansas for Medical Sciences, Little Rock, Arkansas, USA 3. Department of Pathology, University of Arkansas for Medical Sciences, Little Rock, Arkansas, USA *Correspondence to [email protected] Disclosure: The authors have declared no conflicts of interest. Received: 11.11.19 Accepted: 12.02.20 Keywords: Cancer, cancer vaccine, checkpoint inhibitors. Citation: EMJ. 2020;5[3]:102-113. Abstract Pre-clinical models and human clinical trials have confirmed the ability of cancer vaccines to induce immune responses that are tumour-specific and, in some cases, associated with clinical response. However, cancer vaccines as a targeted immunotherapy strategy have not yet come of age. So, why the discordance after so much research has been invested in cancer vaccines? There are several reasons for this that include: limited tumour immunogenicity (limited targeted antigen expression, antigen tolerance); antigenic heterogeneity in tumours; heterogeneity of individual immune responses; multiple mechanisms associated with suppressed functional activity of immune effector cells, the underlying rationale for the use of immune checkpoint inhibitors; and immune system exhaustion. The success of checkpoint therapy has refocussed investigations into defining relationships between tumours and host immune systems, appreciating the mechanisms by which tumour cells escape immune surveillance and reinforcing recognition of the potential of vaccines in the treatment and prevention of cancer. Recent developments in cancer immunotherapies, together with associated technologies, for instance, the unparalleled achievements by immune checkpoint inhibitors and neo- antigen identification tools, may foster potential improvements in cancer vaccines for the treatment of malignancies. -

ISSN: 2320-5407 Int. J. Adv. Res. 6(3), 1363-1370
ISSN: 2320-5407 Int. J. Adv. Res. 6(3), 1363-1370 Journal Homepage: -www.journalijar.com Article DOI:10.21474/IJAR01/6806 DOI URL: http://dx.doi.org/10.21474/IJAR01/6806 RESEARCH ARTICLE A CRITIQUE ON CANCER VACCINE. Sambathkumar R1, Amala Baby2, Sudha M3 and Venkateswaramurthy N2. 1. Department of Pharmaceutics. 2. Department of Pharmacy Practice. 3. Department of Pharmacology J.K.K. Nattraja College of Pharmacy, Kumarapalayam, Tamilnadu - 638183, India. …………………………………………………………………………………………………….... Manuscript Info Abstract ……………………. ……………………………………………………………… Manuscript History The goal of a successful vaccine is to prepare the immune system for invasion of a foreign pathogen and teach them to recognize antigens as Received: 21 January 2018 well as reduce the risk of transmission. In the field of cancer, vaccines Final Accepted: 23 February 2018 are found to be the latest discovery. Provenge® (Sipuleucel-T) is the Published: March 2018 only vaccine approved by Food and Drug Administration for the Keywords:- treatment of cancer. Vaccines are an appealing therapeutic strategy Cancer vaccine, Cells, Treatment. because they are specific. In addition they stimulate the adaptive immune system, thereby producing a memory response allowing for sustained effect without repeated therapy. Revelation of a potential anticancer treatment is as yet a test to the researchers. Thus, the development of effective cancer vaccines require, thoughtful clinical trials, and scientific progress which might induce long-term specific anticancer response and could contribute to effective and lasting elimination of malignant cells. Copy Right, IJAR, 2018,. All rights reserved. …………………………………………………………………………………………………….... Introduction:- Worldwide 6.7 million deaths were reported due to cancer in 2000. But the WHO has predicted this figure to be 15 million by 2020.[1, 2] Despite great efforts to develop better therapy, in 1997 more than 6 million people worldwide died from cancer. -

CP-162837 Johnson & Johnson Announces European Commission
News Release Media Contacts: Seema Kumar +1 908-405-1144 [email protected] Sarah Smith +44 7920 082012 [email protected] Investor Relations: Jennifer McIntyre +1 732-524-3922 Chris DelOrefice +1 732-524-2955 Johnson & Johnson Announces European Commission Approval for Janssen’s Preventive Ebola Vaccine This marks the first major regulatory approval of a vaccine developed by Janssen The Ebola vaccine regimen leverages Janssen’s AdVac® technology, plus Bavarian Nordic’s established MVA-BN® technology Janssen’s AdVac® technology is also being used to develop a vaccine candidate to prevent COVID-19 NEW BRUNSWICK, N.J., 1 July 2020 – Johnson & Johnson today announced that the European Commission (EC) has granted Marketing Authorisation for its Janssen Pharmaceutical Companies’ Ebola vaccine regimen for the prevention of Ebola Virus Disease. Enabled by this approval, Janssen is now collaborating with the World Health Organization (WHO) on vaccine pre-qualification, which should help accelerate registration of its preventive Ebola vaccine regimen in African countries and facilitate broader access to those most in need. Two Marketing Authorisation Applications (MAAs) were submitted to the European Medicines Agency (EMA) for the vaccines composing the two-dose regimen, Zabdeno® (Ad26.ZEBOV) and Mvabea® (MVA-BN-Filo). Marketing Authorisation under exceptional circumstances has been granted following Accelerated Assessment of the MAAs and a positive opinion by the EMA’s Committee for Medicinal Products for Human Use (CHMP). Janssen’s Ebola vaccine regimen is indicated for active immunization for the prevention of Ebola Virus Disease caused by the Zaire ebolavirus species in individuals aged one year and above. -

Immunological Approaches for Treatment of Advanced Stage Cancers Invariably Refractory to Drugs Talwar GP*, Jagdish C
C al & ellu ic la n r li Im C m f u Journal of o n l o a l n o r g Talwar et al., J Clin Cell Immunol 2014, 5:4 u y o J DOI: 10.4172/2155-9899.1000247 ISSN: 2155-9899 Clinical & Cellular Immunology Review Article Open Access Immunological Approaches for Treatment of Advanced Stage Cancers Invariably Refractory to Drugs Talwar GP*, Jagdish C. Gupta, Yogesh Kumar, Kripa N. Nand, Neha Ahlawat, Himani Garg, Kannagi Rana and Hilal Bhat Talwar Research Foundation, New Delhi, India *Corresponding author: Prof. G.P. Talwar, Talwar Research Foundation, E-8, Neb Valley Neb Sarai, New Delhi 110068, India, Tel: 91-011-65022405, 65022404; E- mail: [email protected] Received date: June 18, 2014, Accepted date: August 08, 2014, Published date: August 18, 2014 Copyright: © 2014 Talwar GP, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract Worldwide, deaths due to cancers are taking an increasing toll. Invariably over time cancer cells become refractory to available drugs. At this stage, the tumor is largely metastasized and not amenable to radical surgery or focal radiations. This review seeks to bring out the existence of heterogeneity of cell types in each cancer, and proposes adoption of a combined approach employing more than one therapeutic agent for a more lasting treatment. Also proposed is the use of monoclonal therapeutic antibodies and vaccines against ectopically expressed key molecules for killing of cancer cells and prevention of their multiplication. -

(ACIP) General Best Guidance for Immunization
Appendix 1: Glossary Adverse event. An undesirable medical condition that occurs following vaccination which might be truly caused by a vaccine, or it might be pure coincidence. Adverse reaction. An undesirable medical condition that has been demonstrated to be caused by a vaccine. Evidence for the causal relation is usually obtained through randomized clinical trials, controlled epidemiologic studies, isolation of the vaccine strain from the pathogenic site, or recurrence of the condition with repeated vaccination (i.e., rechallenge); synonyms include side effect and adverse effect. Adjuvant. A vaccine component distinct from the antigen that enhances the immune response to the antigen. Antitoxin. A solution of antibodies against a toxin. Antitoxin can be derived from either human (e.g., tetanus immune globulin) or animal (usually equine) sources (e.g., diphtheria and botulism antitoxin). Antitoxins are used to confer passive immunity and for treatment. Hyperimmune globulin (specific). Special preparations obtained from blood plasma from donor pools preselected for a high antibody content against a specific antigen (e.g., hepatitis B immune globulin, varicella-zoster immune globulin, rabies immune globulin, tetanus immune globulin, vaccinia immune globulin, cytomegalovirus immune globulin, botulism immune globulin). Immune globulin. A sterile solution containing antibodies, which are usually obtained from human blood. It is obtained by cold ethanol fractionation of large pools of blood plasma and contains 15%-18% protein. Intended for intramuscular administration, immune globulin is primarily indicated for routine maintenance of immunity among certain immunodeficient persons and for passive protection against measles and hepatitis A. General Best Practice Guidelines for Immunization: Appendix 1: Glossary 189 Immunobiologic. Antigenic substances (e.g., vaccines and toxoids) or antibody- containing preparations (e.g., globulins and antitoxins) from human or animal donors.