Chromosome Abnormalities and Its Impact on Journal
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Advantage of Genome-Wide Microarrays Over Targeted Approaches
PDF hosted at the Radboud Repository of the Radboud University Nijmegen The following full text is a publisher's version. For additional information about this publication click this link. http://hdl.handle.net/2066/70828 Please be advised that this information was generated on 2021-09-24 and may be subject to change. COPY NUMBER VARIATION AND MENTAL RETARDATION opmaak koolen.indd 1 10-09-2008 10:11:31 Copy number variation and mental retardation The studies presented in this thesis were performed at the Department of Human Genetics, Radboud University Nijmegen Medical Center, Nijmegen, the Netherlands. The research was supported by a grant from the Netherlands Organization for Health Research and Development (ZonMw). Publication of this thesis was financially supported by the Department of Human Genetics, Radboud University Nijmegen Medical Center, Nijmegen, the Netherlands. ISBN/EAN 978-90-6464-290-6 © 2008 D.A. Koolen All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, by print or otherwise, without permission in writing from the author. Cover photo: Printed by: Ponsen & Looijen B.V., Wageningen opmaak koolen.indd 2 10-09-2008 10:11:31 Copy number variation and mental retardation Een wetenschappelijke proeve op het gebied van de Medische Wetenschappen Proefschrift ter verkrijging van de graad doctor aan de Radboud Universiteit Nijmegen op gezag van de rector magnificus prof. mr. S.C.J.J. Kortmann, volgens besluit van het College van Decanen in het openbaar te verdedigen op donderdag 6 november 2008 om 15.30 uur precies door David Aljosja Koolen geboren op 22 juni 1976 te ‘s-Gravenhage opmaak koolen.indd 3 10-09-2008 10:11:32 Promotor: Prof. -

RARE CHROMOSOME DISORDERS the Term, ‘Rare Chromosome Disorders’, Refers to Conditions Which
INFORMATION SHEET Page 1 COMPLEX LEARNING DIFFICULTIES AND DISABILITIES RESEARCH PROJECT (CLDD) RARE CHROMOSOME DISORDERS The term, ‘rare chromosome disorders’, refers to conditions which: 1. occur due to missing, duplicated or re-arranged chromosome material 2. have a low prevalence rate (thus not including chromosomal disorders such as Down syndrome). Chromosomes are structures found in the nuclei of cells in human bodies. Each chromosome contains thousands of genes which determine how we grow and develop. A typically developing person will have 23 pairs of chromosomes with one member of each pair being inherited from each parent, giving a total of 46 individual chromosomes. Two of these are the sex chromosomes which determine whether we are female (XX) or male (XY). The remaining 44 chromosomes are grouped in 22 pairs, numbered 1 to 22. The arms of a chromosome are called ‘p’ (shorter arm) and ‘q’ (long arm) (see Figure 1); these arms are separated into numerical regions, which in turn are divided into bands and sub-bands. p q Figure 1. Diagram of a chromosome Individually, rare chromosome disorders are extremely uncommon, with some being actually unique; however, collectively rare chromosome disorders make up at least one in every 200 live births, with babies either having symptoms from birth or early childhood, or being carriers of a chromosomal abnormality and experiencing the effects when they try to reproduce in later life (Searle and Hultén, 2009). Recent advances in technology and medical expertise has meant that chromosomes can be viewed at ever increasing magnifications, which is resulting in the detection of more complex defects. -

Whole Chromosome Gain Does Not in Itself Confer Cancer-Like Chromosomal Instability
Whole chromosome gain does not in itself confer cancer-like chromosomal instability Anders Valinda,1, Yuesheng Jina, Bo Baldetorpb, and David Gisselssona aDepartment of Clinical Genetics, Lund University, University and Regional Laboratories, Biomedical Center B13, Lund SE22184, Sweden; and bDepartment of Oncology, Lund University, Skåne University Hospital, Lund SE22185, Sweden Edited* by George Klein, Karolinska Institutet, Stockholm, Sweden, and approved November 4, 2013 (received for review June 12, 2013) Constitutional aneuploidy is typically caused by a single-event and chromosomal instability in humans is using constitutional meiotic or early mitotic error. In contrast, somatic aneuploidy, aneuploidy syndromes as a model. Cells from patients with these found mainly in neoplastic tissue, is attributed to continuous syndromes provide a good experimental system for studying the chromosomal instability. More debated as a cause of aneuploidy effects of aneuploidy on overall genome stability on representative is aneuploidy itself; that is, whether aneuploidy per se causes human material. Such cells typically only have a single or a limited chromosomal instability, for example, in patients with inborn set of stem-line chromosome aberrations compared with tumor aneuploidy. We have addressed this issue by quantifying the level cell lines, which typically harbor a multitude of genetic lesions, as of somatic mosaicism, a proxy marker of chromosomal instability, well as a cancer phenotype. The few earlier studies performed on in patients with -

Lab 17. Chromosomes and Karyotypes: How Do Two Physically Healthy Parents Produce a Child with Down Syndrome and a Second Child
Lab 17. Chromosomes and Karyotypes: How Do Two Physically Healthy Parents Produce a Child With Down Syndrome and a Second Child With Cri Du Chat Syndrome? Introduction Mendel’s model of inheritance is the basis for modern genetics. This important model can be broken down into four main ideas. First, and foremost, the fundamental unit of inheritance is the gene and alternative versions of a gene (alleles) account for the variation in inheritable characters. Second, an organism inherits two alleles for each character, one from each parent. Third, if the two alleles differ, then one is fully expressed and determines the nature of the specific trait (this version of the gene is called the dominant allele) while the other one has no noticeable effect (this version of the gene is called the recessive allele). Fourth, the two alleles for each character segregate (or separate) during gamete production. Therefore, an egg or a sperm cell only gets one of the two alleles that are present in the somatic cells of the organism. This idea is known as the law of segregation. It was brilliant (or lucky) that Mendel chose plant traits that turned out to have a relatively simple genetic basis. Each trait that he studied is determined by only one gene, and each of these genes only consists of two alleles. These conditions, however, are not met by all inheritable traits. The relationship between traits and genes is not always a simple one. In this investigation, you will use what you know about the relationship between traits and genes to explain how two children from the same family inherited two different genetic disorders. -

Sema4 Noninvasive Prenatal Select
Sema4 Noninvasive Prenatal Select Noninvasive prenatal testing with targeted genome counting 2 Autosomal trisomies 5 Trisomy 21 (Down syndrome) 6 Trisomy 18 (Edwards syndrome) 7 Trisomy 13 (Patau syndrome) 8 Trisomy 16 9 Trisomy 22 9 Trisomy 15 10 Sex chromosome aneuploidies 12 Monosomy X (Turner syndrome) 13 XXX (Trisomy X) 14 XXY (Klinefelter syndrome) 14 XYY 15 Microdeletions 17 22q11.2 deletion 18 1p36 deletion 20 4p16 deletion (Wolf-Hirschhorn syndrome) 20 5p15 deletion (Cri-du-chat syndrome) 22 15q11.2-q13 deletion (Angelman syndrome) 22 15q11.2-q13 deletion (Prader-Willi syndrome) 24 11q23 deletion (Jacobsen Syndrome) 25 8q24 deletion (Langer-Giedion syndrome) 26 Turnaround time 27 Specimen and shipping requirements 27 2 Noninvasive prenatal testing with targeted genome counting Sema4’s Noninvasive Prenatal Testing (NIPT)- Targeted Genome Counting analyzes genetic information of cell-free DNA (cfDNA) through a simple maternal blood draw to determine the risk for common aneuploidies, sex chromosomal abnormalities, and microdeletions, in addition to fetal gender, as early as nine weeks gestation. The test uses paired-end next-generation sequencing technology to provide higher depth across targeted regions. It also uses a laboratory-specific statistical model to help reduce false positive and false negative rates. The test can be offered to all women with singleton, twins and triplet pregnancies, including egg donor. The conditions offered are shown in below tables. For multiple gestation pregnancies, screening of three conditions -
Molecular Delineation of Small Supernumerary Marker
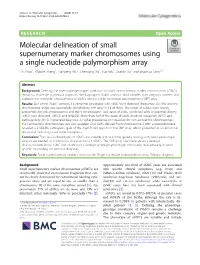
Zhou et al. Molecular Cytogenetics (2020) 13:19 https://doi.org/10.1186/s13039-020-00486-2 RESEARCH Open Access Molecular delineation of small supernumerary marker chromosomes using a single nucleotide polymorphism array Lili Zhou1, Zhaoke Zheng1, Lianpeng Wu2, Chenyang Xu1, Hao Wu1, Xueqin Xu1 and Shaohua Tang1,2* Abstract Background: Defining the phenotype-genotype correlation of small supernumerary marker chromosomes (sSMCs) remains a challenge in prenatal diagnosis. We karyotyped 20,481 amniotic fluid samples from pregnant women and explored the molecular characteristics of sSMCs using a single nucleotide polymorphism (SNP) array. Results: Out of the 20,481 samples, 15 abnormal karyotypes with sSMC were detected (frequency: 0.073%) and the chromosomal origin was successfully identified by SNP array in 14 of them. The origin of sSMCs were mainly acrocentric-derived chromosomes and the Y chromosome. Two cases of sSMC combined with uniparental disomy (UPD) were detected, UPD(1) and UPD(22). More than half of the cases of sSMC involved mosaicism (8/15) and pathogenicity (9/15) in prenatal diagnosis. A higher prevalence of mosaicism for non-acrocentric chromosomes than acrocentric chromosomes was also revealed. One sSMC derived from chromosome 3 with a neocentromere revealed a 24.99-Mb pathogenic gain of the 3q26.31q29 region on the SNP array, which presented as an abnormal ultrasound indicating nasal bone hypoplasia. Conclusion: The clinical phenotypes of sSMCs are variable and so further genetic testing and parental karyotype analysis are needed to confirm the characteristics of sSMCs. The SNP array used here allows a detailed characterisation of the sSMC and establishes a stronger genotype-phenotype correlation, thus allowing detailed genetic counselling for prenatal diagnosis. -
Trisomy 5P Inverted Duplication & Deletion of 5Pftnwdraft3
Trisomy 5p: Inverted duplication and deletion of 5p rarechromo.org Inverted duplication with deletion of 5p Inverted duplication with deletion of 5p, known as inv dup del 5p, is a very rare genetic condition in which there is an extra copy of part of the genetic material (DNA) that makes up the body’s 46 chromosomes, and a missing copy of another part. Like most other chromosome disorders, this usually affects development, and sometimes health and behaviour as well. It is likely that both the extra and missing parts of chromosome 5p have an effect, but a lot depends on their position and size. The precise effects of gaining material from a chromosome vary depending on how large the duplication is, how many genes it contains and what those genes do. The same applies to deletions. The effects may not be limited to the genes within the duplicated or deleted piece of chromosome because these genes may interact with other genes on the same chromosome or other chromosomes. Chromosomes usually come in pairs, and we inherit one chromosome from each parent. Of the 46 chromosomes, two are a pair of sex chromosomes: two Xs for a girl and an X and a Y for a boy. The remaining 44 chromosomes are grouped into 22 pairs and are numbered 1 to 22, approximately from largest to smallest. Each chromosome has a short (p) arm (from petit, the French for small) and a long (q) arm. The diagram below shows the short arm. Chromosome 5 Short (p) arm Bands Base pairs 0Mb 5Mb 10Mb 15Mb 20Mb 25Mb 30Mb 35Mb 40Mb 45Mb 48.4Mb Long (q) arm 2 People have 2 copies of chromosome 5 in most of their body cells. -

General Contribution
24 Abstracts of 37th Annual Meeting A1 A SCREENING METHOD FOR FRAGILE X MUTATION: DETECTION OF THE CGG REPEAT IN FMR-1 GENE BY PCR WITH BIOTIN-LABELED PRIMER. ..Eiji NANBA, Kousaku OHNO and Kenzo TAKESHITA Division of Child Neurology, Institute of Neurological Sciences, Tot- tori University School of Medicine. Yonago We have developed a new polymerase chain reaction(PCR)-based method for detection of the CGG repeat in FMR-1 gene. No specific product from PCR was detected on the gel with ethidium bromide staining, because 7-deaza-2'-dGTP is necessary for amplification of this repeat. Biotin-labeled primer was used for PCR and the product was transferred to a nylon membrane followed the detection of biotin by Smilight kit. The size of PCR product from normal control were slightly various and around 300bp. No PCR product was detected from 3 fragile X male patients in 2 families diagnosed by cytogenetic examination. This method is useful for genetic screen- ing of male mental retardation patients to exclude the fragile X mutation. A2 DNA ANALYSISFOR FRAGILE X SYNDROME Osamu KOSUDA,Utak00GASA, ~.ideynki INH, a~ji K/NAGIJCltI, and Kazumasa ]tIKIJI (SILL Inc., Tokyo) Fragile X syndrome is X-linked disease having the amplification of (CG6)n repeat sequence in the chromsomeXq27.3. We performed Southern blot analysis using three probes recognized repetitive sequence resion. Normal controle showed 5.2Kb with Eco RI digest and 2.7Kb with Eco RI/Bss ttII digest as the germ tines by the Southern blot analysis. However, three cell lines established fro~ unrelated the patients with fragile X showed the abnormal bands between 5.2 and 7.7Kb with Eco RI digest, and between 2.7 and 7.7Kb with Eco aI/Bss HII digest. -

Diseases of the Digestive System (KOO-K93)
CHAPTER XI Diseases of the digestive system (KOO-K93) Diseases of oral cavity, salivary glands and jaws (KOO-K14) lijell Diseases of pulp and periapical tissues 1m Dentofacial anomalies [including malocclusion] Excludes: hemifacial atrophy or hypertrophy (Q67.4) K07 .0 Major anomalies of jaw size Hyperplasia, hypoplasia: • mandibular • maxillary Macrognathism (mandibular)(maxillary) Micrognathism (mandibular)( maxillary) Excludes: acromegaly (E22.0) Robin's syndrome (087.07) K07 .1 Anomalies of jaw-cranial base relationship Asymmetry of jaw Prognathism (mandibular)( maxillary) Retrognathism (mandibular)(maxillary) K07.2 Anomalies of dental arch relationship Cross bite (anterior)(posterior) Dis to-occlusion Mesio-occlusion Midline deviation of dental arch Openbite (anterior )(posterior) Overbite (excessive): • deep • horizontal • vertical Overjet Posterior lingual occlusion of mandibular teeth 289 ICO-N A K07.3 Anomalies of tooth position Crowding Diastema Displacement of tooth or teeth Rotation Spacing, abnormal Transposition Impacted or embedded teeth with abnormal position of such teeth or adjacent teeth K07.4 Malocclusion, unspecified K07.5 Dentofacial functional abnormalities Abnormal jaw closure Malocclusion due to: • abnormal swallowing • mouth breathing • tongue, lip or finger habits K07.6 Temporomandibular joint disorders Costen's complex or syndrome Derangement of temporomandibular joint Snapping jaw Temporomandibular joint-pain-dysfunction syndrome Excludes: current temporomandibular joint: • dislocation (S03.0) • strain (S03.4) K07.8 Other dentofacial anomalies K07.9 Dentofacial anomaly, unspecified 1m Stomatitis and related lesions K12.0 Recurrent oral aphthae Aphthous stomatitis (major)(minor) Bednar's aphthae Periadenitis mucosa necrotica recurrens Recurrent aphthous ulcer Stomatitis herpetiformis 290 DISEASES OF THE DIGESTIVE SYSTEM Diseases of oesophagus, stomach and duodenum (K20-K31) Ill Oesophagitis Abscess of oesophagus Oesophagitis: • NOS • chemical • peptic Use additional external cause code (Chapter XX), if desired, to identify cause. -

Abstracts from the 50Th European Society of Human Genetics Conference: Electronic Posters
European Journal of Human Genetics (2019) 26:820–1023 https://doi.org/10.1038/s41431-018-0248-6 ABSTRACT Abstracts from the 50th European Society of Human Genetics Conference: Electronic Posters Copenhagen, Denmark, May 27–30, 2017 Published online: 1 October 2018 © European Society of Human Genetics 2018 The ESHG 2017 marks the 50th Anniversary of the first ESHG Conference which took place in Copenhagen in 1967. Additional information about the event may be found on the conference website: https://2017.eshg.org/ Sponsorship: Publication of this supplement is sponsored by the European Society of Human Genetics. All authors were asked to address any potential bias in their abstract and to declare any competing financial interests. These disclosures are listed at the end of each abstract. Contributions of up to EUR 10 000 (ten thousand euros, or equivalent value in kind) per year per company are considered "modest". Contributions above EUR 10 000 per year are considered "significant". 1234567890();,: 1234567890();,: E-P01 Reproductive Genetics/Prenatal and fetal echocardiography. The molecular karyotyping Genetics revealed a gain in 8p11.22-p23.1 region with a size of 27.2 Mb containing 122 OMIM gene and a loss in 8p23.1- E-P01.02 p23.3 region with a size of 6.8 Mb containing 15 OMIM Prenatal diagnosis in a case of 8p inverted gene. The findings were correlated with 8p inverted dupli- duplication deletion syndrome cation deletion syndrome. Conclusion: Our study empha- sizes the importance of using additional molecular O¨. Kırbıyık, K. M. Erdog˘an, O¨.O¨zer Kaya, B. O¨zyılmaz, cytogenetic methods in clinical follow-up of complex Y. -

95 Birth Defects Exec Summ
Executive Summary In 1995, 865 cases of birth defects were detected among live born infants and fetuses of 20 or more weeks gestation delivered to mothers residing in Texas Public Health Regions 6 and 11 (Houston/Galveston region and Lower Rio Grande Valley). In this first full year of the Registry, surveillance was limited to approximately 23 major categories of birth defects, comprising 30 to 40 percent of all known structural malformations. Down syndrome, oral clefts, and spina bifida were the most common birth defects, although some major structural malformations were not yet monitored in 1995. Age Patterns: Both trisomy 21 (Down syndrome) and trisomy 18 (Edwards syndrome) demonstrated an age-specific rate pattern that was J-shaped, with the highest birth prevalence (“rates”) observed among mothers 35 years of age and older. Gastroschisis, a malformation of the abdominal wall, exhibited highest rates among the youngest mothers and decreased with each older age group. Racial/Ethnic Patterns: Anencephaly and spina bifida were lowest among African Americans; however, rates were similar in whites and Hispanics. Among the heart defects, relatively high rates of tetralogy of Fallot were observed among African Americans, although they exhibited relatively low rates of hypoplastic left heart. Cleft palate alone was more likely to occur among whites and Hispanics. Rates of trisomy 18 (Edwards syndrome) were highest among African Americans and whites. Gender Patterns: With regard to sex, higher rates were documented among females for anencephaly, and to a lesser extent, spina bifida. Females experienced two-fold higher rates of trisomy 18 (Edwards syndrome). Males had higher rates of cleft lip with or without cleft palate. -

Application of Neural Networks for Classification of Patau, Edwards
Catic et al. BMC Medical Genomics (2018) 11:19 DOI 10.1186/s12920-018-0333-2 RESEARCHARTICLE Open Access Application of Neural Networks for classification of Patau, Edwards, Down, Turner and Klinefelter Syndrome based on first trimester maternal serum screening data, ultrasonographic findings and patient demographics Aida Catic1,2* , Lejla Gurbeta1,4, Amina Kurtovic-Kozaric1,3, Senad Mehmedbasic2 and Almir Badnjevic1,4,5,6 Abstract Background: The usage of Artificial Neural Networks (ANNs) for genome-enabled classifications and establishing genome-phenotype correlations have been investigated more extensively over the past few years. The reason for this is that ANNs are good approximates of complex functions, so classification can be performed without the need for explicitly defined input-output model. This engineering tool can be applied for optimization of existing methods for disease/syndrome classification. Cytogenetic and molecular analyses are the most frequent tests used in prenatal diagnostic for the early detection of Turner, Klinefelter, Patau, Edwards and Down syndrome. These procedures can be lengthy, repetitive; and often employ invasive techniques so a robust automated method for classifying and reporting prenatal diagnostics would greatly help the clinicians with their routine work. Methods: The database consisted of data collected from 2500 pregnant woman that came to the Institute of Gynecology, Infertility and Perinatology “Mehmedbasic” for routine antenatal care between January 2000 and December 2016. During first trimester all women were subject to screening test where values of maternal serum pregnancy- associated plasma protein A (PAPP-A) and free beta human chorionic gonadotropin (β-hCG) were measured. Also, fetal nuchal translucency thickness and the presence or absence of the nasal bone was observed using ultrasound.