Aircraft Accident Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
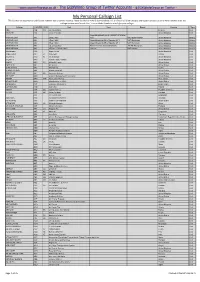
My Personal Callsign List This List Was Not Designed for Publication However Due to Several Requests I Have Decided to Make It Downloadable
- www.egxwinfogroup.co.uk - The EGXWinfo Group of Twitter Accounts - @EGXWinfoGroup on Twitter - My Personal Callsign List This list was not designed for publication however due to several requests I have decided to make it downloadable. It is a mixture of listed callsigns and logged callsigns so some have numbers after the callsign as they were heard. Use CTL+F in Adobe Reader to search for your callsign Callsign ICAO/PRI IATA Unit Type Based Country Type ABG AAB W9 Abelag Aviation Belgium Civil ARMYAIR AAC Army Air Corps United Kingdom Civil AgustaWestland Lynx AH.9A/AW159 Wildcat ARMYAIR 200# AAC 2Regt | AAC AH.1 AAC Middle Wallop United Kingdom Military ARMYAIR 300# AAC 3Regt | AAC AgustaWestland AH-64 Apache AH.1 RAF Wattisham United Kingdom Military ARMYAIR 400# AAC 4Regt | AAC AgustaWestland AH-64 Apache AH.1 RAF Wattisham United Kingdom Military ARMYAIR 500# AAC 5Regt AAC/RAF Britten-Norman Islander/Defender JHCFS Aldergrove United Kingdom Military ARMYAIR 600# AAC 657Sqn | JSFAW | AAC Various RAF Odiham United Kingdom Military Ambassador AAD Mann Air Ltd United Kingdom Civil AIGLE AZUR AAF ZI Aigle Azur France Civil ATLANTIC AAG KI Air Atlantique United Kingdom Civil ATLANTIC AAG Atlantic Flight Training United Kingdom Civil ALOHA AAH KH Aloha Air Cargo United States Civil BOREALIS AAI Air Aurora United States Civil ALFA SUDAN AAJ Alfa Airlines Sudan Civil ALASKA ISLAND AAK Alaska Island Air United States Civil AMERICAN AAL AA American Airlines United States Civil AM CORP AAM Aviation Management Corporation United States Civil -

Ársskýrsla Flugmálastjórnar Íslands 2007
ÁRSSKÝRSLA FLUGMÁLASTJÓRNAR ÍSLANDS 2007 Ágúst 2008 Efnisyfirlit Efnisyfirlit ........................................................................................................................... 2 1.0 Flugmál á árinu 2007 ................................................................................................ 3 2.0 Alþjóðleg samskipti .................................................................................................. 5 3.0 Skipurit og starfsmenn .............................................................................................. 6 4.0 Stefnumótun Flugmálastjórnar Íslands ..................................................................... 7 4.1 Hlutverk og meginmarkmið.................................................................................. 7 4.2 Gildi ...................................................................................................................... 8 4.3 Stefnumið............................................................................................................ 10 4.4 Ímynd .................................................................................................................. 12 4.5 Eðli samskipta við viðskiptavini og hagsmunaaðila og væntingar þeirra........... 12 5.0 Sérverkefnastofa ..................................................................................................... 13 6.0 Stjórnsýslusvið........................................................................................................ 14 6.1 Laga- og reglugerðarmál.................................................................................... -

Global Volatility Steadies the Climb
WORLD AIRLINER CENSUS Global volatility steadies the climb Cirium Fleet Forecast’s latest outlook sees heady growth settling down to trend levels, with economic slowdown, rising oil prices and production rate challenges as factors Narrowbodies including A321neo will dominate deliveries over 2019-2038 Airbus DAN THISDELL & CHRIS SEYMOUR LONDON commercial jets and turboprops across most spiking above $100/barrel in mid-2014, the sectors has come down from a run of heady Brent Crude benchmark declined rapidly to a nybody who has been watching growth years, slowdown in this context should January 2016 low in the mid-$30s; the subse- the news for the past year cannot be read as a return to longer-term averages. In quent upturn peaked in the $80s a year ago. have missed some recurring head- other words, in commercial aviation, slow- Following a long dip during the second half Alines. In no particular order: US- down is still a long way from downturn. of 2018, oil has this year recovered to the China trade war, potential US-Iran hot war, And, Cirium observes, “a slowdown in high-$60s prevailing in July. US-Mexico trade tension, US-Europe trade growth rates should not be a surprise”. Eco- tension, interest rates rising, Chinese growth nomic indicators are showing “consistent de- RECESSION WORRIES stumbling, Europe facing populist backlash, cline” in all major regions, and the World What comes next is anybody’s guess, but it is longest economic recovery in history, US- Trade Organization’s global trade outlook is at worth noting that the sharp drop in prices that Canada commerce friction, bond and equity its weakest since 2010. -

Airliner Census Western-Built Jet and Turboprop Airliners
World airliner census Western-built jet and turboprop airliners AEROSPATIALE (NORD) 262 7 Lufthansa (600R) 2 Biman Bangladesh Airlines (300) 4 Tarom (300) 2 Africa 3 MNG Airlines (B4) 2 China Eastern Airlines (200) 3 Turkish Airlines (THY) (200) 1 Equatorial Int’l Airlines (A) 1 MNG Airlines (B4 Freighter) 5 Emirates (300) 1 Turkish Airlines (THY) (300) 5 Int’l Trans Air Business (A) 1 MNG Airlines (F4) 3 Emirates (300F) 3 Turkish Airlines (THY) (300F) 1 Trans Service Airlift (B) 1 Monarch Airlines (600R) 4 Iran Air (200) 6 Uzbekistan Airways (300) 3 North/South America 4 Olympic Airlines (600R) 1 Iran Air (300) 2 White (300) 1 Aerolineas Sosa (A) 3 Onur Air (600R) 6 Iraqi Airways (300) (5) North/South America 81 RACSA (A) 1 Onur Air (B2) 1 Jordan Aviation (200) 1 Aerolineas Argentinas (300) 2 AEROSPATIALE (SUD) CARAVELLE 2 Onur Air (B4) 5 Jordan Aviation (300) 1 Air Transat (300) 11 Europe 2 Pan Air (B4 Freighter) 2 Kuwait Airways (300) 4 FedEx Express (200F) 49 WaltAir (10B) 1 Saga Airlines (B2) 1 Mahan Air (300) 2 FedEx Express (300) 7 WaltAir (11R) 1 TNT Airways (B4 Freighter) 4 Miat Mongolian Airlines (300) 1 FedEx Express (300F) 12 AIRBUS A300 408 (8) North/South America 166 (7) Pakistan Int’l Airlines (300) 12 AIRBUS A318-100 30 (48) Africa 14 Aero Union (B4 Freighter) 4 Royal Jordanian (300) 4 Europe 13 (9) Egyptair (600R) 1 American Airlines (600R) 34 Royal Jordanian (300F) 2 Air France 13 (5) Egyptair (600R Freighter) 1 ASTAR Air Cargo (B4 Freighter) 6 Yemenia (300) 4 Tarom (4) Egyptair (B4 Freighter) 2 Express.net Airlines -

Prospectus February 2007
PROSPECTUS FEBRUARY 2007 ICELANDAIR GROUP HF. This page is intentionally left blank TABLE OF CONTENTS I. Summary II. Securities Note III. Registration Document This Prospectus is published on 12 February 2007. The Prospectus has been scrutinised and approved by the Iceland Stock Exchange (ICEX) on behalf of the Financial Service Authority in Iceland. It was prepared for the listing of Icelandair Group hf. on the ICEX Main List. This Prospectus, published in English only, consists of three documents: Summary, Securities Note and Registration Document. For the timeframe of 12 months from the date of the Prospectus (lifetime of the document), the Prospectus is available on the website: www.icelandairgroup.is. I. SUMMARY This summary should be read as an introduction to the Prospectus dated 12 February 2007 containing this Summary, a Securities Note and a Registration Document. Prospective investors should read the Prospectus in its entirety. Because this is a summary, it does not contain all the information that may be important to you. You should read this summary in conjunction with the more detailed information in the rest of the Prospectus, including the “Risk Factors” sections and the financial statements and the notes thereto. Any decision to invest in the Shares should be based on consideration of the Prospectus as a whole. Following the implementation of the relevant provisions of the Prospectus Directive in each member state of the European Economic Area, no civil liability will attach to us or our board of directors in any such member state in respect of this summary, including any translation hereof, unless it is misleading, inaccurate or inconsistent when read together with the other parts of the Prospectus. -

Company Title AIR Convention 2018 Current Attendee List 2018-09-06
AIR Convention 2018 Current Attendee list 2018-09-06 Company Title AVICO Founder and CEO AVICO General Manager All Nippon Airways Trading Co., Ltd. Sales & Marketing, Purchasing 15below Business Development Manager AAR International INC Regional Sales Manager Aarya airlines Manager,Product Engineering ABA Law Senior Partner ABU Dhabi Aviation Line Captain Head of Operational Excellence and Industrial Abu Dhabi university Engineering Adria Airways Emergency and Safety Adria Airways Head Of Purchasing Adria Airways Tehnika Deputy CEO ADZ NAGANO GmbH General Manager Aegean airlines sa Chief Intructor Aegean airlines sa Head of Purchasing Aer Lingus Executive Director Aer Lingus Recruitment Manager AerFin n/a Aero Caribe de Honduras CEO Aero Surveys Chief Commercial Officer AEROBAY sas Sales Vice President Aeroflot Director of fleet planning and aircraft procurement Aeroflot General Director Aeroflot - russian airlines Captain Aerolineas Argentinas Snr. Sales Manager Aerologic CEO Aeromexico Head of training Aeromexico Training instructor Commercial Director Aéroport Paris-Vatry Aeroporto Milano Linate / Malpensa Environment and Airport Safety Manager Aerospace Asset Trading VP / General Manager Aerotask CEO & VP Financial Solutions Afex Aviation FX Hedging Specialist Afiqiyiah air ways Training excutive A-Group / Moscow Sheremetyevo and President St.Petersbirg Pulokov, Termial A AY Jones MRO General Merchants Air Annobon Technical Director Air Arabia Human Resources Manager -Business support Air Astana Director Air Astana Technical Procurement -

All Carriers
Summary of Disability-Related Complaint Data All Carriers Total number of complaints submitted: 15,290 Carrier Name Number of Complaints AER LINGUS LIMITED 14 AERODYNAMICS, INC. 0 AEROFLOT RUSSIAN AIRLINES 1 AEROLINEAS ARGENTINAS 0 AEROMEXICO 2 AEROPOSTAL ALAS DE VENEZUEL 0 AEROSUR USA 0 AEROSVIT AIRLINES 0 AIR ATLANTA ICELANDIC 0 AIR CANADA 282 AIR CANADA JAZZ 40 AIR CHINA 0 AIR EUROPA LINEAS AEREAS 0 AIR FRANCE 87 AIR GREENLAND 0 AIR JAMAICA LIMITED 8 AIR JAPAN, CO. 1 AIR NEW ZEALAND 7 AIR PACIFIC, LTD. 0 AIR TAHITI NUI 3 AIR TRANSAT 6 AIR-INDIA 2 AIRTRAN 190 ALASKA AIRLINES 184 ALITALIA-LINEE AEREE ITALIA 13 ALL NIPPON AIRWAYS CO. 4 ALLEGIANT 35 ALOHA AIRLINES 19 AMERICAN AIRLINES 3,187 AMERICAN EAGLE AIRLINES 500 AMERISTAR AIR CARGO, INC. 0 ARKIA ISRAELI AIRLINES, LTD. 0 ASIANA AIRLINES, INC. 2 ATA 60 ATLANTIC SOUTHEAST AIRLINES 289 AUSTRIAN AIRLINES 6 AVIACSA AIRLINES 1 AVIANCA 0 AVIATION CONCEPTS 0 BAHAMASAIR HOLDING LIMITED 0 BELAIR AIRLINES 0 BOSTON-MAINE AIRWAYS 0 BRITISH AIRWAYS PLC 73 BRITISH MIDLAND AIRWAYS LTD. 15 BWIA WEST INDIES LIMITED 5 TEM ENTERPRISES/XTRA AIRWAYS 1 CATHAY PACIFIC AIRWAYS, LTD. 8 CAYMAN AIRWAYS LTD. 1 CHAMPION AIR 11 CHINA AIRLINES, LTD. 0 CHINA EASTERN AIRLINES 0 COMAIR 245 COMLUX AVIATION 0 COMPANIA MEXICANA DE AVIACION 3 COMPANIA PANAMENA (COPA) 4 COMPASS 4 CONDOR FLUGDIENST 0 CONTINENTAL 499 CONTINENTAL MICRONESIA 0 CZECH AIRLINES 4 DALAVIA-FAR EAST AIRWAYS 0 DC AVIATION GMBH 0 DELTA AIR LINES 2,532 EGYPTAIR 0 EL AL ISRAEL AIRLINES LTD. 21 ELYSAIR SAS 1 EMIRATES AIRLINE 2 EOS AIRLINES 1 ETHIOPIAN AIRLINES 0 ETIHAD AIRWAYS 0 EUROFLY, S.P.A. -
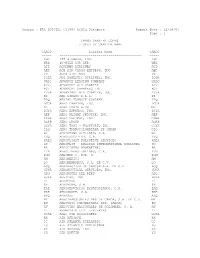
FAA DOT/TSC CY1997 ACAIS Database Report Date : 12/18/97 Page : 1
Source : FAA DOT/TSC CY1997 ACAIS Database Report Date : 12/18/97 Page : 1 CARGO CARRIER CODES LISTED BY CARRIER NAME CARCD Carrier Name CARCD ----- ------------------------------------------ ----- KHC 135 AIRWAYS, INC. KHC WRB 40-MILE AIR LTD. WRB ACD ACADEMY AIRLINES ACD AER ACE AIR CARGO EXPRESS, INC. AER VX ACES AIRLINES VX IQDA ADI DOMESTIC AIRLINES, INC. IQDA UALC ADVANCE LEASING COMPANY UALC ADV ADVANCED AIR CHARTER ADV ACI ADVANCED CHARTERS INT ACI YDVA ADVANTAGE AIR CHARTER, INC. YDVA EI AER LINGUS P.L.C. EI TPQ AERIAL TRANSIT COMPANY TPQ DGCA AERO CHARTER, INC. DGCA ML AERO COSTA RICA ML DJYA AERO EXPRESS, INC. DJYA AEF AERO FLIGHT SERVICE, INC. AEF GSHA AERO FREIGHT, INC. GSHA AGRP AERO GROUP AGRP CGYA AERO TAXI - ROCKFORD, INC. CGYA CLQ AERO TRANSCOLOMBIANA DE CARGA CLQ G3 AEROCHAGO AIRLINES, S.A. G3 EVQ AEROEJECUTIVO, C.A. EVQ XAES AEROFLIGHT EXECUTIVE SERVICES XAES SU AEROFLOT - RUSSIAN INTERNATIONAL AIRLINES SU AR AEROLINEAS ARGENTINAS AR LTN AEROLINEAS LATINAS, C.A. LTN ROM AEROMAR C. POR. A. ROM AM AEROMEXICO AM QO AEROMEXPRESS, S.A. DE C.V. QO ACQ AERONAUTICA DE CANCUN S.A. DE C.V. ACQ HUKA AERONAUTICAL SERVICES, INC. HUKA ADQ AERONAVES DEL PERU ADQ HJKA AEROPAK, INC. HJKA PL AEROPERU PL 6P AEROPUMA, S.A. 6P EAE AEROSERVICIOS ECUATORIANOS, C.A. EAE KRE AEROSUCRE, S.A. KRE ASQ AEROSUR ASQ MY AEROTRANSPORTES MAS DE CARGA, S.A. DE C.V. MY ZU AEROVAIS COLOMBIANAS LTD. (ARCA) ZU AV AEROVIAS NACIONALES DE COLOMBIA, S. A. AV ZL AFFRETAIR LTD. (PRIVATE) ZL UCAL AGRO AIR ASSOCIATES UCAL RK AIR AFRIQUE RK CC AIR ATLANTA ICELANDIC CC LU AIR ATLANTIC DOMINICANA LU AX AIR AURORA, INC. -

Inhaltsverzeichnis
Inhaltsverzeichnis Vorwort 3 AIR VIA 67 DELTA AIR LINES 134 ALASKA AIRLINES 68: DELTA CONNECTION 135 Inhaltsverzeichnis 4 ALASKA-HORIZON AIR 69 DHL AVIATIONA-EAT 136 ALITALIA 70 DONAVIA 137 Betriebseinstellungen, Pleiten, Fusionen 6 ALLEGIANT AIR 71 DRAGONAIR 138 und sonstige Veränderungen zur Vorauf ALLIANCE AIRLINES 72 DRUKAIR 139 lage ALL NIPPON AIRWAYS-ANA 73 AMERICAN AIRLINES 74 E Die Fluggesellschaften A-Z AMERICAN EAGLE AIRLINES 76 EASTERN AIRWAYS 140 AMERIJET INTERNATIONAL 77 EASY JET 141 A ANADOLU JET 78 EDELWEISSAIR 142 ABXAIR 7 ANTONÖV AIRLINES 79 EGVPTAIR 143 ADRIA AIRWAYS 8 ARIANA AFGHAN AIRLINES 80 EL AL ISRAEL AIRLINES 144 AEGEAN AIRLINES 9 ARKE 81 EMIRATES 145 AER LINGUS 10 ARKIA ISRAELI AIRLINES 82 ENTER AIR 146 AER LINGUS REGIONAL 11 ASERCA 83 ESTONIAN AIR 147 AEROFLOT-RUSS1AN AIRLINES 12 ASIANA 84 ETHIOPIAN AIRLINES 148 ÄEROÜNEAS ARGENfINAS 13 ATLANTIC AIRWAYS 85 ETIHAD AIRWAYS 149 AEROLOGIC 14 ATLAS AIR 86 ETIHAD REGIONAL 150 AEROMEXICO 15 ATLASJET INTERNATIONAL AIRWAYS 87 EURO ATLANTIC AIRWAYS 151 AEROMEXICO CONNECT 16 AURIGNY AIR SERVICE 88 EUROPE AIRPOST 152 AEROPOSTAL 17 AURORA AIRLINES 89 EUROWINGS 153 AFRIQIYAH AIRWAYS 18 AUSTRAL LINEAS AEREAS 90 EVA AIR 154 AIGLE AZÜR 19 AUSTRIAN AIRLINES 91. EXPRESS JET AIRLINES 155 AIR ALGERIE 20 AVIANCA 93 A1RARABIA 21 AZAL-AZERBAIJAN AIRLINES 95 F A1RASIA 22 AZUL-LINHAS AEREAS BRASILEIRAS 96 FEDEX 156 AIR ASTANA 24 FIJ1 AIRWAYS 157 AIR ATLANTA ICELANDIC 25 B FINNAIR 158 AIR AUSTRAL 26 BAHAMASAIR 97 FIRST AIR 159 AIR AZORES 27 BANGKOK AIRWAYS 98 FLYBE 160 AIR BALTIC 28 BELAVIA-BELARUSSIAN -

Air Cargo Tracing
AIR CARGO TRACING (HAVE YOUR AWB TRACKING NO. AND CLICK THE AIRLINE YOUR SHIPMENT IS BOOKED TO, TYPE THE AWB NO. IN THE TRACING BLOCK) ABSA Cargo Airline / LATAM Cargo Brasil M3 549 ABX Air GB 832 Adria Airways JP 165 Aegean Airlines A3 390 Aer Lingus Cargo EI 053 (alternate tracking site) Aeroflot SU 507 Aeroflot SU 555 (alternate tracking site) (from/to Germany: Aeroflot Germany) Aerolineas Argentinas AR 044 (alternate tracking site) Aerosvit VV 870 Aeromexico Cargo AM 139 (alternate tracking site) AeroUnion 6R 873 Aigle Azur ZI 439 Air Algerie AH 124 Air Arabia G9 514 AirAsia D7 843 AirAsia Berhad AK 807 Air Astana KC 465 Air Atlanta Icelandic CC 318 Air Baltic BT 657 Air Berlin AB 745 AirBridge Cargo RU 580 Air Canada AC 014 Air China CA 999 Air Europa Cargo UX 996 Air France AF 057 (Skyteam tracking) Air Greenland GL 631 Air Hong Kong LD 288 Air Incheon KJ 994 Air India AI 098 Air Jamaica JM 201 Air Macau NX 675 Air Madagascar MD 258 Air Malawi QM 167 Air Malta KM 643 Air Mauritius MK 239 (alternate tracking site) Airmax Cargo M8 658 Air Moldova 9U 572 Air Namibia SW 186 Air New Zealand NZ 086 Air Niugini PX 656 Air Serbia (JAT) JU 115 Air Seychelles HM 061 Air Tahiti Nui TN 244 Air Transat TS 649 Alaska Airlines AS 027 (alternate tracking site) Alitalia AZ 055 (alternate tracking site) Allied Air 4W 574 Aloha Air Cargo KH 687 American Airlines AA 001 Amerijet International M6 810 ANA All Nippon Cargo NH 205 Asiana Airlines OZ 988 (alternate tracking site) ASL Airlines Belgium (formerly TNT) 3V 756 Astral Aviation 8V 485 (more tracking) -

Air Atlanta Is the Launch Customer for IQSMS in Iceland
__________________________________________________________________________________________ Press Release H O L D R E L E A S E U N T I L February 2nd, 2021 ___________________________________________________________________________ Air Atlanta Icelandic is the launch customer for IQSMS in Iceland ASQS goes north supporting Air Atlanta Icelandic in taking its safety processes to the next level VIENNA – February 2nd, 2021 – ASQS GmbH, the Vienna-based global provider of integrated aviation Quality and Safety Management Solutions, today announced that the largest ACMI and charter service provider in the world, Air Atlanta Icelandic, has chosen IQSMS (Integrated Quality and Safety Management System) to further optimize safety and quality standards within the organization. The company is ASQS’s first customer in Iceland enabling the Austrian aviation IT company to further expand its global footprint and presence in the Nordic region. The demand for uncomplicated, intuitive and powerful safety management solutions is what leads aviation companies of all kinds to ASQS. With its core product IQSMS, the company supports the daily operations of more than 200 operators worldwide. The web-based integrated SMS (Safety Management System) and QMS (Quality Management System) software enables users to automate daily processes, increasing safety compliance and business performance. In over thirty years of business history, the largest globally operating ACMI (Aircraft, Crew, Maintenance, Insurance) and charter service provider in the world, Air Atlanta Icelandic, has continuously demonstrated a strong focus on excellent customer service while meeting the highest national and international safety standards. To further optimize safety processes, the company has put together its personal IQSMS Suite to meet the organization’s individual needs and has opted for a multi-phased implementation of the IQSMS core modules, including the respective offline applications, as well as two additional modules. -

Air Transport Industry
ANALYSIS OF THE EU AIR TRANSPORT INDUSTRY Final Report 2006 Contract no: TREN/05/MD/S07.52077 by Cranfield University Department of Air Transport Disclaimer and copyright: This report has been carried out for the Directorate-General for Energy and Transport in the European Commission and expresses the opinion of the organisation undertaking the contract TREN/05/MD/S07.52077. These views have not been adopted or in any way approved by the European Commission and should not be relied upon as a statement of the European Commission's or the Transport and Energy DG's views. The European Commission does not guarantee the accuracy of the information given in the report, nor does it accept responsibility for any use made thereof. Copyright in this report is held by the European Communities. Persons wishing to use the contents of this report (in whole or in part) for purposes other than their personal use are invited to submit a written request to the following address: EUROPEAN COMMISSION - DG ENERGY AND TRANSPORT - LIBRARY (DM28, 0/36) - B-1049 BRUSSELS E-MAIL (HTTP://EC.EUROPA.EU/DGS/ENERGY_TRANSPORT/CONTACT/INDEX_EN.HTM) Analysis of the EU Air Transport Industry, 2006 1 CONTENTS 1 AIR TRANSPORT INDUSTRY OVERVIEW........................................................................................9 2 REGULATORY DEVELOPMENTS.....................................................................................................15 2.1 GLOBAL DEVELOPMENTS....................................................................................................................15