Condition Gout
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Gouty Tophi on the Ear: a Review
Gouty Tophi on the Ear: A Review Indy Chabra, MD, PhD; Rajendra Singh, MD Practice Points Consider gout in the differential of papulonodular lesions on the ear. If biopsying to rule out gout, fix the biopsy specimen in ethanol or Carnoy fixative to preserve birefrin- gence of urate crystals. Although the classic location of gouty tophi is the and gout. Presentation of gout in younger patients great toe (podagra), gouty tophi of the ear also is without these risk factors should raise suspicion of common and is worth including in the differential renal disease or an underlying enzyme deficiency, diagnosis in patients presenting with ear lesions. such as hypoxanthine guanine phosphoribosyl- Other entities presenting as papules or nodules transferase deficiency in X-linked recessive Lesch- on the ear include chondrodermatitis nodularis Nyhan syndrome.3 helicis (CNH), actinic keratosis, basal cell carci- noma, squamous cell carcinoma,CUTIS verruca vulgaris, Clinical Features amyloids, rheumatoid nodules, and elastotic nod- Gouty tophi classically present as hard, yellow-white ules. If tophaceous gout is suspected, alcohol papules and nodules of a chalky consistency on the fixation of the biopsy specimen is preferable, as joints of the hands and feet. Less common locations it enables visualization of characteristic needle- for gouty tophi include the ears, elbows (olecranon shaped urate crystals. bursae), and the Achilles tendon. Decreased tem- Cutis. 2013;92:190-192. perature and reduced blood flow in these areas may Do Notexplain Copy the predilection for these locations. The ears are the most common location for gouty tophi in the out is the most common cause of inflamma- head and neck region and may be a heralding sign tory arthritis in men and classically presents of gout.4 Auricular tophi usually are located on the Gas painful acute monoarthritis of the great toe helical rims but also may be located on the antihe- (podagra) or the knee. -

Juvenile Spondyloarthropathies: Inflammation in Disguise
PP.qxd:06/15-2 Ped Perspectives 7/25/08 10:49 AM Page 2 APEDIATRIC Volume 17, Number 2 2008 Juvenile Spondyloarthropathieserspective Inflammation in DisguiseP by Evren Akin, M.D. The spondyloarthropathies are a group of inflammatory conditions that involve the spine (sacroiliitis and spondylitis), joints (asymmetric peripheral Case Study arthropathy) and tendons (enthesopathy). The clinical subsets of spondyloarthropathies constitute a wide spectrum, including: • Ankylosing spondylitis What does spondyloarthropathy • Psoriatic arthritis look like in a child? • Reactive arthritis • Inflammatory bowel disease associated with arthritis A 12-year-old boy is actively involved in sports. • Undifferentiated sacroiliitis When his right toe starts to hurt, overuse injury is Depending on the subtype, extra-articular manifestations might involve the eyes, thought to be the cause. The right toe eventually skin, lungs, gastrointestinal tract and heart. The most commonly accepted swells up, and he is referred to a rheumatologist to classification criteria for spondyloarthropathies are from the European evaluate for possible gout. Over the next few Spondyloarthropathy Study Group (ESSG). See Table 1. weeks, his right knee begins hurting as well. At the rheumatologist’s office, arthritis of the right second The juvenile spondyloarthropathies — which are the focus of this article — toe and the right knee is noted. Family history is might be defined as any spondyloarthropathy subtype that is diagnosed before remarkable for back stiffness in the father, which is age 17. It should be noted, however, that adult and juvenile spondyloar- reported as “due to sports participation.” thropathies exist on a continuum. In other words, many children diagnosed with a type of juvenile spondyloarthropathy will eventually fulfill criteria for Antinuclear antibody (ANA) and rheumatoid factor adult spondyloarthropathy. -
Uncontrolled Gout Fact Sheet
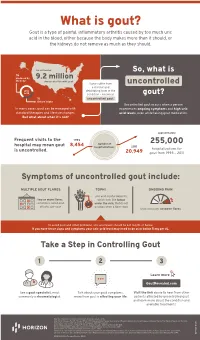
What is gout? Gout is a type of painful, inflammatory arthritis caused by too much uric acid in the blood, either because the body makes more than it should, or the kidneys do not remove as much as they should. An estimated So, what is ⅔ produced by 9.2 million the body Americans live with gout Some suffer from uncontrolled a chronic and uric debilitating form of the acid condition – known as gout? ⅓ uncontrolled gout. dietary intake Uncontrolled gout occurs when a person In many cases, gout can be managed with experiences ongoing symptoms and high uric standard therapies and lifestyle changes. acid levels, even while taking gout medication. But what about when it’s not? approximately Frequent visits to the 1993 number of 255,000 hospital may mean gout 8,454 hospitalizations 2011 is uncontrolled. hospitalizations for 20,949 gout from 1993 – 2011 Symptoms of uncontrolled gout include: MULTIPLE GOUT FLARES TOPHI ONGOING PAIN uric acid crystal deposits, two or more flares, which look like lumps sometimes called gout under the skin, that do not attacks, per year go away when a flare stops that continues between flares To avoid gout and other problems, uric acid levels should be 6.0 mg/dL or below. If you have these signs and symptoms your uric acid level may need to be at or below 5 mg per dL. Take a Step in Controlling Gout 1 2 3 Learn more GoutRevealed.com See a gout specialist, most Talk about your gout symptoms, Visit the link above to hear from other commonly a rheumatologist. -

Arthritis (Overview)
ARTHRITIS Having arthritis can significantly affect your comfort & ability to walk and move with confidence. This is because it affects your joints, which are responsible for keeping you steady and moving efficiently. Your symptoms and causes will depend on the type of arthritis that you have. At Masterton Foot Clinic, our podiatrists work closely with patients with four types of arthritis. OSTEOARTHRITIS Osteoarthritis is the wear and tear arthritis that develops slowly over time as the cartilage that covers your bone ends wears down. The cause is largely from natural use over many years, though injuries, alignment issues within the joint and other diseases may result in it developing at a faster rate. We work with patients that want to feel more comfortable on their feet, despite having arthritis in their hip, knee, ankle and foot joints. RHEUMATOID ARTHRITIS Rheumatoid arthritis is an autoimmune disease that affects the joints. It occurs when your body’s immune system attacks the joints and causes damage, inflammation and pain. If the effects of rheumatoid arthritis remain uncontrolled, it can cause permanent changes in the appearance of the joints, especially at the feet and hands. We work with patients to help them manage the discomfort associated with rheumatoid arthritis, offloading prominent and painful areas that have developed due to changes in the joints. GOUT Gout is an inflammatory arthritis that results from a high concentration of uric acid in the blood. It is associated with a high intake of purine-containing foods like red meats, shellfish and red wine, hence it was previously referred to as the rich man’s disease. -

Tophus Measurement As an Outcome Measure for Clinical Trials of Chronic Gout: Progress and Research Priorities NICOLA DALBETH, FIONA M
Tophus Measurement as an Outcome Measure for Clinical Trials of Chronic Gout: Progress and Research Priorities NICOLA DALBETH, FIONA M. McQUEEN, JASVINDER A. SINGH, PATRICIA A. MacDONALD, N. LAWRENCE EDWARDS, H. RALPH SCHUMACHER Jr, LEE S. SIMON, LISA K. STAMP, TUHINA NEOGI, ANGELO L. GAFFO, PUJA P. KHANNA, MICHAEL A. BECKER, and WILLIAM J. TAYLOR ABSTRACT. Despite the recognition that tophus regression is an important outcome measure in clinical trials of chronic gout, there is no agreed upon method of tophus measurement. A number of methods have been used in clinical trials of chronic gout, from simple physical measurement techniques to more complex advanced imaging methods. This article summarizes methods of tophus measurement and discusses their properties. Physical measurement using Vernier calipers meets most aspects of the Outcome Measures in Rheumatology (OMERACT) filter. Rigorous testing of the complex methods, particularly with respect to reliability and sensitivity to change, is needed to determine the appropriate use of these methods. Further information is also required regarding which method of physical measurement is best for use in future clinical trials. The need to develop and test a patient-reported outcome measure of tophus burden is also highlighted. (J Rheumatol 2011;38:1458–61; doi:10.3899/jrheum.110272) Key Indexing Terms: GOUT TOPHUS OUTCOME MEASURE The tophus is a pathognomonic feature of chronic gout. This Despite recognition that tophus regression is an important lesion represents a chronic inflammatory response to outcome measure in clinical trials of chronic gout, there is no monosodium urate (MSU) crystals deposited most often with- agreed upon method of tophus measurement6. -

Ulcerated Tophaceous Gout
Volume 25 Number 3| March 2019| Dermatology Online Journal || Case Presentation 25(3):8 Ulcerated tophaceous gout Michael P Ryan1 BS, Seena Monjazeb2 MD, Brandon P Goodwin2 MD, Ashley R Group2 MD Affiliations: 1School of Medicine, University of Texas Medical Branch, Galveston, Texas, USA, 2Department of Dermatology, University of Texas Medical Branch, Galveston, Texas, USA Corresponding Author: Michael P. Ryan BS, University of Texas Medical Branch, Galveston, Texas 77555-0783, Tel: 409-747-3376, Email: [email protected] premenopausal women and 7mg/dL for men and Abstract postmenopausal women [2]. There are two broad Gout is a common inflammatory arthropathy with a mechanisms that cause hyperuricemia. The first is high prevalence worldwide. Increased levels of uric underexcretion of uric acid by the kidneys, which is acid in the blood lead to deposition of monosodium responsible for about 90% of cases. The second is urate crystals in the joints, inflammation, and pain. overproduction of uric acid, which accounts for the Acute gout attacks are often sudden, monoarticular, other 10% of cases [3]. Acute gout attacks are and typically resolve within a week, whereas chronic typically rapid in onset and monoarticular, gout is often polyarticular with baseline pain between attacks. In chronic gout, depositions of uric presenting as a hot, swollen, erythematous joint. acid known as tophi can form throughout the body. These will often resolve spontaneously within days Despite the high prevalence of gout and the to a week and patients will be asymptomatic frequency with which tophi occur, ulceration over between attacks. Chronic gout typically has tophi is surprisingly rare. -

Gout and Monoarthritis
Gout and Monoarthritis Acute monoarthritis has numerous causes, but most commonly is related to crystals (gout and pseudogout), trauma and infection. Early diagnosis is critical in order to identify and treat septic arthritis, which can lead to rapid joint destruction. Joint aspiration is the gold standard method of diagnosis. For many reasons, managing gout, both acutely and as a chronic disease, is challenging. Registrars need to develop a systematic approach to assessing monoarthritis, and be familiar with the management of gout and other crystal arthropathies. TEACHING AND • Aetiology of acute monoarthritis LEARNING AREAS • Risk factors for gout and septic arthritis • Clinical features and stages of gout • Investigation of monoarthritis (bloods, imaging, synovial fluid analysis) • Joint aspiration techniques • Interpretation of synovial fluid analysis • Management of hyperuricaemia and gout (acute and chronic), including indications and targets for urate-lowering therapy • Adverse effects of medications for gout, including Steven-Johnson syndrome • Indications and pathway for referral PRE- SESSION • Read the AAFP article - Diagnosing Acute Monoarthritis in Adults: A Practical Approach for the Family ACTIVITIES Physician TEACHING TIPS • Monoarthritis may be the first symptom of an inflammatory polyarthritis AND TRAPS • Consider gonococcal infection in younger patients with monoarthritis • Fever may be absent in patients with septic arthritis, and present in gout • Fleeting monoarthritis suggests gonococcal arthritis or rheumatic fever -

Surgical Management of a Large, Gouty Tophus
Case in Point Surgical Management of a Large, Gouty Tophus Scott Glassburn, DPM This patient, who could not tolerate medical therapy for his chronic gout, eventually consented to surgery to remove a tophus on his left foot that was severely affecting his quality of life. out is a metabolic disease InITIaL ExaM plantarly. It extended distally to the that occurs when excess A 56-year-old man was referred to interphalangeal joint of the hallux amounts of uric acid cir- a VA podiatry clinic by his primary and proximally toward the plantar Gculating in the blood crys- care provider (PCP). He presented medial arch, approximately mid-shaft tallize and subsequently deposit in with a large, indurated mass about of the first metatarsal bone. joints or soft tissue. Hyperuricemia his left first metatarsophalangeal Radiographs revealed a large, con- is the condition most often associ- (MTP) joint (Figure 1). The lesion tiguous, soft tissue density about the ated with an acute gouty attack or, in was not focally tender, but its girth first MTP joint as described (Figure chronic states, with the formation of hindered the patient’s ability to wear 2). There were no lytic osseous le- tophi.1,2 In all cases, the demonstra- shoes. The patient had similar masses sions or areas in proximity with tion of monosodium urate crystals in and symptoms of intermittent pain diminished bone density. Examina- the joint or surrounding soft tissues and swelling in multiple other joints, tion revealed excellent pedal pulses is sufficient to make a definitive diag- including his hands, knees, wrists, (dorsalis pedis, +2/4; posterior tibial, nosis of gout.3–5 and elbows. -

19120 Arthritis Aus Gout Booklet
Taking control of your Gout A practical guide to treatments, services and lifestyle choices How can this booklet help you This booklet is designed for people who have gout. It will help you understand your • make healthy choices for your condition so that you can better general health and wellbeing manage your symptoms and continue • find support and additional to lead an active and healthy life. information to cope with the This booklet offers information and impact of gout. practical advice to help you: The information inside is based • understand what gout is and on the latest research and what it means for you recommendations, and has been reviewed by Australian experts in the • understand how medicines can field of arthritis to make sure it is help treat gout attacks and current and relevant to your needs. prevent future attacks So go ahead — take control of • work with your healthcare team your gout! to manage the disease in the short and long term © Copyright Arthritis Australia 2014 Supported by: AstraZeneca Pty Limited ABN 54 009 682 311 Alma Road, North Ryde NSW 2113 2 Taking control of your Gout Contents Understanding gout 4 Treating gout 10 Diet and lifestyle 16 Who can help? 21 Working with your GP 22 Seeing a rheumatologist 23 Other health professionals 24 Seeking support 26 Glossary of terms 28 Useful resources 29 Medical and consumer consultants Tanya deKroo, Information Resources Coordinator, Arthritis Australia Wendy Favorito, Arthritis Australia Consumer Representative and Board Member Assoc Prof Neil McGill, Rheumatologist Assoc Prof Julian McNeil, Rheumatologist and Chair of Australian Rheumatology Association’s Therapeutics Committee Assoc Prof Peter Youssef, Rheumatologist and Chair of Arthritis Australia’s Scientific Advisory Committee Arthritis Australia 3 Understanding gout What is gout? the main reason for more than Gout is an extremely painful form nine out of ten people with gout). -

21362 Arthritis Australia a to Z List
ARTHRITISINFORMATION SHEET Here is the A to Z of arthritis! A D Goodpasture’s syndrome Achilles tendonitis Degenerative joint disease Gout Achondroplasia Dermatomyositis Granulomatous arteritis Acromegalic arthropathy Diabetic finger sclerosis Adhesive capsulitis Diffuse idiopathic skeletal H Adult onset Still’s disease hyperostosis (DISH) Hemarthrosis Ankylosing spondylitis Discitis Hemochromatosis Anserine bursitis Discoid lupus erythematosus Henoch-Schonlein purpura Avascular necrosis Drug-induced lupus Hepatitis B surface antigen disease Duchenne’s muscular dystrophy Hip dysplasia B Dupuytren’s contracture Hurler syndrome Behcet’s syndrome Hypermobility syndrome Bicipital tendonitis E Hypersensitivity vasculitis Blount’s disease Ehlers-Danlos syndrome Hypertrophic osteoarthropathy Brucellar spondylitis Enteropathic arthritis Bursitis Epicondylitis I Erosive inflammatory osteoarthritis Immune complex disease C Exercise-induced compartment Impingement syndrome Calcaneal bursitis syndrome Calcium pyrophosphate dehydrate J (CPPD) F Jaccoud’s arthropathy Crystal deposition disease Fabry’s disease Juvenile ankylosing spondylitis Caplan’s syndrome Familial Mediterranean fever Juvenile dermatomyositis Carpal tunnel syndrome Farber’s lipogranulomatosis Juvenile rheumatoid arthritis Chondrocalcinosis Felty’s syndrome Chondromalacia patellae Fibromyalgia K Chronic synovitis Fifth’s disease Kawasaki disease Chronic recurrent multifocal Flat feet Kienbock’s disease osteomyelitis Foreign body synovitis Churg-Strauss syndrome Freiberg’s disease -

CONCOMITANT GOUT and RHEUMATOID ARTHRITIS - a CASE Presented with Multiple Nodular Swellings on REPORT Feet, Hands, Wrists and Elbows
349 350 INDIAN JOURNAL OF MEDICAL SCIENCES CASE REPORT consulted various practitioners and took allopathic and indigenous medications but to no relief. Two months prior to admission he CONCOMITANT GOUT AND RHEUMATOID ARTHRITIS - A CASE presented with multiple nodular swellings on REPORT feet, hands, wrists and elbows. Patient’s past medical history is significant for hypertension, POOJA KHOSLA*, ATUL GOGIA**, P. K. AGARWAL***, AMIT PAHUJA**, SUNIL JAIN***, K. K. SAXENA# diabetes mellitus, chronic ethanolism and renal stones for which he underwent left nephrectomy about 25 years ago. Family Abstract history is non-contributory. Figure 1: Multiple nodules present on metatarsal joints of both feet (Gouty Tophi) We report a case of definite rheumatoid arthritis and co-existing gout. Although gout On examination multiple nodules were present and rheumatoid arthritis are relatively common entities individually, the co-existence on metatarsal joints of both feet, Achilles of these two conditions is rare. tendon bilaterally, left prepatellar bursa, bilateral metacarpophalangeal joint, right KEY WORDS: Gout, Rheumatoid Arthritis olecranon process. There was swelling and tenderness of PIP and MCP joints of both feet. (Figure 1) Laboratory data revealed INTRODUCTION metatarsophalangeal joint. He had hemoglobin - 8.9gm/dl, ESR 124 mm at the asymmetrical joint pains and swelling at end of first hour, leucocyte count 7400/cmm Gout and rheumatoid arthritis rarely co-exist in irregular intervals with exacerbations and with normal differential count. Random blood the same patient. As separate disease entities remissions. The symptoms subsided in sugar was 139 mg/dl, Creatinine- 1.6 mg/dl; they are relatively common. Rheumatoid between but there was no period when patient serum uric acid level was 10.9 mg/dl. -

Spot the Diagnosis
Spot the diagnosis Gouty tophi of small joints of hand: A classical presentation Manju Kumari1, Mukul Singh2 From 1Senior resident, 2Professor, Department of Pathology, V.M.M.C and Safdarjung Hospital, New Delhi, India. Correspondence to: Dr. Manju Kumari, Department of Pathology, Flat No.45, United India Apartments, Mayur Vihar Phase-I Extension-110091, New Delhi, India. E-mail: [email protected] Received - 09 June 2019 Initial Review - 30 June 2019 Accepted - 18 July 2019 ABSTRACT Gout is an acute inflammatory disorder caused by deposition of monosodium urate crystals. Gouty tophus can be the initial presenting feature of chronic disease. Diagnosis of periarticular nodules can be a challenge for clinicians. Fine needle aspiration can provide quick, cost-effective and definitive diagnosis for the early management of these patients. Here, we present the case of gouty tophi of the right-hand index finger in a 45-years-old male leading to restricted finger movements. Keywords: Crystals, Fine needle aspiration cytology, Gouty tophus. out is a metabolic disorder characterized by an yellowish nodules were present ranging in size from 0.1X 0.1 to inflammatory response to the deposition of monosodium 0.3X 0.3 cm2.The flexion and extension movements of the finger Gurate crystals secondary to hyperuricemia. The prevalence were restricted (Fig. 1). No specific clinical diagnosis/ differential of gout in India is 0.12% with those with tophus on the finger are diagnosis were given. further very rare [1]. It is more common in males than in females. On a radiograph, there was a soft tissue swelling in the finger The hyperuricemia developed may be either due to increased which was eroding the middle and distal phalanx of the finger production or decreased excretion of uric acid.