Spondylodiscitis Andpseudarthrosis in a Patient with Enteropathic
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Juvenile Spondyloarthropathies: Inflammation in Disguise
PP.qxd:06/15-2 Ped Perspectives 7/25/08 10:49 AM Page 2 APEDIATRIC Volume 17, Number 2 2008 Juvenile Spondyloarthropathieserspective Inflammation in DisguiseP by Evren Akin, M.D. The spondyloarthropathies are a group of inflammatory conditions that involve the spine (sacroiliitis and spondylitis), joints (asymmetric peripheral Case Study arthropathy) and tendons (enthesopathy). The clinical subsets of spondyloarthropathies constitute a wide spectrum, including: • Ankylosing spondylitis What does spondyloarthropathy • Psoriatic arthritis look like in a child? • Reactive arthritis • Inflammatory bowel disease associated with arthritis A 12-year-old boy is actively involved in sports. • Undifferentiated sacroiliitis When his right toe starts to hurt, overuse injury is Depending on the subtype, extra-articular manifestations might involve the eyes, thought to be the cause. The right toe eventually skin, lungs, gastrointestinal tract and heart. The most commonly accepted swells up, and he is referred to a rheumatologist to classification criteria for spondyloarthropathies are from the European evaluate for possible gout. Over the next few Spondyloarthropathy Study Group (ESSG). See Table 1. weeks, his right knee begins hurting as well. At the rheumatologist’s office, arthritis of the right second The juvenile spondyloarthropathies — which are the focus of this article — toe and the right knee is noted. Family history is might be defined as any spondyloarthropathy subtype that is diagnosed before remarkable for back stiffness in the father, which is age 17. It should be noted, however, that adult and juvenile spondyloar- reported as “due to sports participation.” thropathies exist on a continuum. In other words, many children diagnosed with a type of juvenile spondyloarthropathy will eventually fulfill criteria for Antinuclear antibody (ANA) and rheumatoid factor adult spondyloarthropathy. -
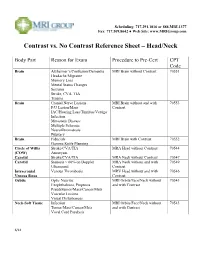
Contrast Vs. No Contrast Reference Sheet – Head/Neck
Scheduling: 717.291.1016 or 888.MRI.1377 Fax: 717.509.8642 ● Web Site: www.MRIGroup.com Contrast vs. No Contrast Reference Sheet – Head/Neck Body Part Reason for Exam Procedure to Pre-Cert CPT Code Brain Alzheimer’s/Confusion/Dementia MRI Brain without Contrast 70551 Headache/Migraine Memory Loss Mental Status Changes Seizures Stroke, CVA, TIA Trauma Brain Cranial Nerve Lesions MRI Brain without and with 70553 F/U Lesion/Mass Contrast IAC/Hearing Loss/Tinnitus/Vertigo Infection Metastatic Disease Multiple Sclerosis Neurofibromatosis Pituitary Brain Fiducials MRI Brain with Contrast 70552 Gamma Knife Planning Circle of Willis Stroke/CVA/TIA MRA Head without Contrast 70544 (COW) Aneurysm Carotid Stroke/CVA/TIA MRA Neck without Contrast 70547 Carotid Stenosis > 60% on Doppler MRA Neck without and with 70549 Ultrasound Contrast Intracranial Venous Thrombosis MRV Head without and with 70546 Venous Sinus Contrast Orbits Optic Neuritis MRI Orbits/Face/Neck without 70543 Exophthalmos, Proptosis and with Contrast Pseudotumor/Mass/Cancer/Mets Vascular Lesions Visual Disturbances Neck-Soft Tissue Infection MRI Orbits/Face/Neck without 70543 Tumor/Mass/Cancer/Mets and with Contrast Vocal Cord Paralysis 6/14 Scheduling: 717.291.1016 or 888.MRI.1377 Fax: 717.509.8642 ● Web Site: www.MRIGroup.com Contrast vs. No Contrast Reference Sheet – Spine Body Part Reason for Exam Procedure to Pre-Cert CPT Code Spine: Cervical Degenerative Disease MRI Cervical Spine without Contrast 72141 Disc Herniation Extremity Pain/Weakness Neck Pain Radiculopathy Trauma Spine: -

Arthritis and Joint Pain
Fact Sheet News from the IBD Help Center ARTHRITIS AND JOINT PAIN Arthritis, or inflammation (pain with swelling) of the joints, is the most common extraintestinal complication of IBD. It may affect as many as 30% of people with Crohn’s disease or ulcerative colitis. Although arthritis is typically associated with advancing age, in IBD it often strikes younger patients as well. In addition to joint pain, arthritis also causes swelling of the joints and a reduction in flexibility. It is important to point out that people with arthritis may experience arthralgia, but many people with arthralgia may not have arthritis. Types of Arthritis • Peripheral Arthritis. Peripheral arthritis usually affects the large joints of the arms and legs, including the elbows, wrists, knees, and ankles. The discomfort may be “migratory,” moving from one joint to another. If left untreated, the pain may last from a few days to several weeks. Peripheral arthritis tends to be more common among people who have ulcerative colitis or Crohn’s disease of the colon. The level of inflammation in the joints generally mirrors the extent of inflammation in the colon. Although no specific test can make an absolute diagnosis, various diagnostic methods—including analysis of joint fluid, blood tests, and X-rays—are used to rule out other causes of joint pain. Fortunately, IBD-related peripheral arthritis usually does not cause any lasting damage and treatment of the underlying IBD typically results in improvement in the joint discomfort. • Axial Arthritis. Also known as spondylitis or spondyloarthropathy, axial arthritis produces pain and stiffness in the lower spine and sacroiliac joints (at the bottom of the back). -

Cervical Neck Pain Or Cervical Radiculopathy
Revised 2018 American College of Radiology ACR Appropriateness Criteria® Cervical Neck Pain or Cervical Radiculopathy Variant 1: New or increasing nontraumatic cervical or neck pain. No “red flags.” Initial imaging. Procedure Appropriateness Category Relative Radiation Level Radiography cervical spine Usually Appropriate ☢☢ MRI cervical spine without IV contrast May Be Appropriate (Disagreement) O CT cervical spine without IV contrast May Be Appropriate ☢☢☢ CT cervical spine with IV contrast Usually Not Appropriate ☢☢☢ MRI cervical spine without and with IV Usually Not Appropriate contrast O CT cervical spine without and with IV Usually Not Appropriate contrast ☢☢☢ CT myelography cervical spine Usually Not Appropriate ☢☢☢☢ CTA neck with IV contrast Usually Not Appropriate ☢☢☢ Discography cervical spine Usually Not Appropriate ☢☢ Facet injection/medial branch block cervical Usually Not Appropriate spine ☢☢ MRA neck with IV contrast Usually Not Appropriate O MRA neck without IV contrast Usually Not Appropriate O MRI cervical spine with IV contrast Usually Not Appropriate O Bone scan whole body with SPECT or Usually Not Appropriate SPECT/CT neck ☢☢☢ X-ray myelography cervical spine Usually Not Appropriate ☢☢☢ ACR Appropriateness Criteria® 1 Cervical Neck Pain or Cervical Radiculopathy Variant 2: New or increasing nontraumatic cervical radiculopathy. No “red flags.” Initial imaging. Procedure Appropriateness Category Relative Radiation Level MRI cervical spine without IV contrast Usually Appropriate O CT cervical spine without IV contrast -

Acute Calcific Discitis with Intravertebral Disc Herniation in the Dorsolumbar Spine
Published online: 2021-08-02 MUSCULOSKELETAL Case report: Acute calcific discitis with intravertebral disc herniation in the dorsolumbar spine Puneet Mittal, Kavita Saggar, Parambir Sandhu, Kamini Gupta Department of Radiodiagnosis, Dayanand Medical College & Hospital, Ludhiana, Punjab, India Correspondence: Dr. Puneet Mittal, Department of Radiodiagnosis, Dayanand Medical College & Hospital, Tagore Nagar, Civil Lines, Ludhiana, Punjab - 141 001, India. E-mail: [email protected] Abstract Acute calcific discitis is a rare but well-known condition of unknown etiology. In symptomatic cases, the most common site is the cervical spine. We describe the CT scan and MRI findings in a symptomatic patient, with a lesion in the dorsolumbar spine. Key words: Acute; calcific; discitis; dorsolumbar; MR Introduction Acute calcifc discitis is a rare condition. When symptomatic, it can be mistaken for infection.[1] Most of the symptomatic cases present in the cervical spine.[1-3] We present the CT scan and MRI findings in a patient who had involvement of the dorsolumbar spine, with associated intravertebral disc herniation. Case Report A 10-year-old boy presented with a 2-week history of pain in the lower back following a yoga session in school. The pain had gradually worsened over the last 5 days. The patient was afebrile. The total white blood cell (WBC) count was normal. The erythrocyte sedimentation rate (ESR) was raised (52 mm/h). The Mantoux test was negative. A radiograph obtained elsewhere and repeated a day after the MRI [Figure 1], showed calcification of the D12-L1 intervertebral disc. MRI showed hypointense signal in the D12-L1 intervertebral disc on T1W [Figure 2A] and T2W [Figure 2B and C] images. -

Cervical Spondylodiscitis in an Infant with Torticollis
Cervical Spondylodiscitis in IMAGES IN CLINICAL an Infant with Torticollis RADIOLOGY BRECHT VAN BERKEL KRISTIN SUETENS LUC BREYSEM *Author affiliations can be found in the back matter of this article ABSTRACT CORRESPONDING AUTHOR: Brecht Van Berkel Teaching point: Narrowing of the intervertebral space and destruction of the adjacent UZ Leuven, BE vertebral end plates on conventional radiography or CT should raise suspicion for brecht.vanberkel@student. spondylodiscitis in symptomatic infants. kuleuven.be KEYWORDS: Spondylodiscitis; MRI; pediatric; torticollis; cervical; CT TO CITE THIS ARTICLE: Van Berkel B, Suetens K, Breysem L. Cervical Spondylodiscitis in an Infant with Torticollis. Journal of the Belgian Society of Radiology. 2021; 105(1): 35, 1–4. DOI: https://doi.org/10.5334/ jbsr.2454 Van Berkel et al. Journal of the Belgian Society of Radiology DOI: 10.5334/jbsr.2454 2 CASE REPORT disc space and loss of height of vertebral bodies C3 and C4 and irregular alignment of the end plates. On An eight-month-old infant presented at the emergency the sagittal T1-weighted Short-tau inversion-recovery department with a history of torticollis for six weeks. (STIR) images, the hyperintense signal in the vertebral Blood results showed no elevated inflammatory bodies of C3 and C4, as well as in the surrounding tissues parameters. Vertical lateral X-ray of the cervical spine (arrowheads) were compatible with a widespread area demonstrated a kyphotic angulation at the level of C3– of bone and soft tissue oedema (Figure 2). There were C4, narrowing of the intervertebral disc space, irregular no diffusion-restricted areas and no accompanying fluid end plates, and loss of height of the vertebral body of collections. -
Spondyloarthropathies and Reactive Arthritis
RHEUMATOLOGY SPONDYLOARTHRITIS ROBERT L. DIGIOVANNI, DO, FACOI PROGRAM DIRECTOR LMC RHEUMATOLOGY FELLOWSHIP [email protected] DISCLOSURES •NONE SERONEGATIVE SPONDYLOARTHROPATHIES SLIDES PREPARED BY GENE JALBERT, DO SENIOR RHEUMATOLOGY FELLOW THE SPONDYLOARTHROPATHIES: • Ankylosing Spondylitis (A.S.) • Non-radiographic Axial spondyloarthropathies (nr-axSpA) • Psoriatic Arthritis (PsA) • Inflammatory Bowel Disease Associated (Enteropathic) • Crohn and Ulcerative Colitis • +/- Microscopic colitis • Reactive Arthritis (ReA) • Juvenile-Onset SpA • Others: Bechet’s dz, Celiac, Whipples, pouchitis. THE FAMOUS VENN DIAGRAM: SPONDYLOARTHROPATHY: • First case of Axial SpA was reported in 1691 however some believe Ramses II has A.S. • 2.4 million adults in the United States have Seronegative SpA • Compare with RA, which affects about 1.3 million Americans • Prevalence variation for A.S.: Europe (0.12-1%), Asia (0.17%), Latin America (0.1%), Africa (0.07%), USA (0.34%). • Pathophysiology in general: • Responsible Interleukins: IL-12, IL17, IL-22, and IL23. SPONDYLOARTHROPATHY: • Axial SpA: • Radiographic (Sacroiliitis seen on X- ray) • No Radiographic features non- radiographic SpA (nr-SpA) • Nr-SpA was formally known as undifferentiated SpA • Peripheral SpA: • Enthesitis, dactylitis and arthritis • Eventually evolves into a specific diagnosis A.S., PsA, etc. • Can be a/w IBD, HLA-B27 positivity, uveitis SHARED CLINICAL FEATURES: • Axial joint disease (especially SI joints) • Asymmetrical Oligoarthritis (2-4 joints). • Dactylitis (Sausage -

Letters to the Editor 155
LETTERS TO THE EDITOR 155 indicates increased risk for microvascular disease. N murmur was audible along the left sternal border EnglJMed 1981;305:191-4. and/or a typical diastolic Doppler signal was 4. Pal B, Anderson J, Griffiths ID, Dick WC. Rheumatic demonstrated under the aortic valve on the Echo- disorders in diabetes mellitus: association between lim- ited joint mobility and Dupuytren's contracture Doppler as well as a diastolic fluttering of the [Abstract]. Br J Rheumawl 1986;25:122-3. anterior leaflet of the mitral valve. Severity of AI 5. Prokop DJ, Tuderman L, Guzman NA. Collagen in was arbitrarily assessed in relation to clinical and normal and diseased connective tissue. In: McCarty echocardiographic data. AI was considered as mild JD, ed. Arthritis and allied conditions. 9th edn. Phila- in asymptomatic patients if auscultation and Echo- delphia: Lea & Febiger, 1979. Doppler revealed a typical AI in the absence of an 6. Buckingham BA, Vitto J, Sandbork C, et al. increased left ventricular cavity. The Doppler sig- Scleroderma like syndrome and non-enzymatic glyco- nal of regurgitation had to be recorded in the left sylation of collage in children with poorly controlled ventricle only below the aortic leaflets. It was con- insulin dependent diabetes [Abstract]. Paediatr Res 1981;5:626. sidered severe when patients were symptomatic, 7. Schnider SL, Kohn RR. Effects of age and diabetes on the left ventricular cavity enlarged and AI recorded the solubility and non-enzymatic glycosylation of in the left ventricle beyond the tip of the mitral human skin collage. J Clin Invest 981;67:1630-5. -

Cervical Radiculopathy Clinical Guidelines for Medical Necessity Review
Cervical Radiculopathy Clinical Guidelines for Medical Necessity Review Version: 3.0 Effective Date: November 13, 2020 Cervical Radiculopathy (v3.0) © 2020 Cohere Health, Inc. All Rights Reserved. 2 Important Notices Notices & Disclaimers: GUIDELINES SOLELY FOR COHERE’S USE IN PERFORMING MEDICAL NECESSITY REVIEWS AND ARE NOT INTENDED TO INFORM OR ALTER CLINICAL DECISION MAKING OF END USERS. Cohere Health, Inc. (“Cohere”) has published these clinical guidelines to determine medical necessity of services (the “Guidelines”) for informational purposes only, and solely for use by Cohere’s authorized “End Users”. These Guidelines (and any attachments or linked third party content) are not intended to be a substitute for medical advice, diagnosis, or treatment directed by an appropriately licensed healthcare professional. These Guidelines are not in any way intended to support clinical decision making of any kind; their sole purpose and intended use is to summarize certain criteria Cohere may use when reviewing the medical necessity of any service requests submitted to Cohere by End Users. Always seek the advice of a qualified healthcare professional regarding any medical questions, treatment decisions, or other clinical guidance. The Guidelines, including any attachments or linked content, are subject to change at any time without notice. ©2020 Cohere Health, Inc. All Rights Reserved. Other Notices: CPT copyright 2019 American Medical Association. All rights reserved. CPT is a registered trademark of the American Medical Association. -

Lumbar Spinal Stenosis Clinical Guidelines for Medical Necessity Review
Lumbar Spinal Stenosis Clinical Guidelines for Medical Necessity Review Version: 4.0 Effective Date: November 13, 2020 Lumbar Spinal Stenosis (v4.0) © 2020 Cohere Health, Inc. All Rights Reserved. Important Notices Notices & Disclaimers: GUIDELINES SOLELY FOR COHERE’S USE IN PERFORMING MEDICAL NECESSITY REVIEWS AND ARE NOT INTENDED TO INFORM OR ALTER CLINICAL DECISION MAKING OF END USERS. Cohere Health, Inc. (“Cohere”) has published these clinical guidelines to determine medical necessity of services (the “Guidelines”) for informational purposes only, and solely for use by Cohere’s authorized “End Users”. These Guidelines (and any attachments or linked third party content) are not intended to be a substitute for medical advice, diagnosis, or treatment directed by an appropriately licensed healthcare professional. These Guidelines are not in any way intended to support clinical decision making of any kind; their sole purpose and intended use is to summarize certain criteria Cohere may use when reviewing the medical necessity of any service requests submitted to Cohere by End Users. Always seek the advice of a qualified healthcare professional regarding any medical questions, treatment decisions, or other clinical guidance. The Guidelines, including any attachments or linked content, are subject to change at any time without notice. ©2020 Cohere Health, Inc. All Rights Reserved. Other Notices: CPT copyright 2019 American Medical Association. All rights reserved. CPT is a registered trademark of the American Medical Association. Guideline Information: Specialty Area: Diseases of the musculoskeletal system and connective tissue (M00-M99) CarePath Group: Spine CarePath Name: Lumbar Spinal Stenosis (M48) Physician author: Mandy Armitage, MD (Sports Medicine) Peer reviewed by: Adrian Thomas, MD (Orthopedic Spine Surgeon) Literature review current through: June 22, 2020 Document last updated: November 13, 2020 Type: [X] Adult (18+ yo) | [_] Pediatric (0-17yo) Page 2 of 57 Lumbar Spinal Stenosis (v4.0) © 2020 Cohere Health, Inc. -

Tuberculous Spondylodiscitis in A
ISSN: 2474-3658 Mangouka et al. J Infect Dis Epidemiol 2019, 5:083 DOI: 10.23937/2474-3658/1510083 Volume 5 | Issue 4 Journal of Open Access Infectious Diseases and Epidemiology RESEARCH ARTICLE Tuberculous Spondylodiscitis in a Military Hospital in Gabon: Report of Eleven Patients Mangouka Guingali Laurette1, Iroungou Berthe A2, Bivigou-Mboumba Berthold3*, Oura Landry4, Mwanyombet Lucien4 and Nzenze Jean Raymond1 Check for 1Service de Médecine Interne, Hôpital d’Instruction des Armées Omar Bongo Ondimba (HIA OBO), Gabon updates 2École d’Application su Service de Santé Militaire de Libreville (EASSML), Gabon 3Unité mixte de Recherches sur le VIH et les Maladies Infectieuses Associées (UMR VIH-MIA), Centre Internationale de Recherche Médicale de Franceville (CIRMF), Gabon 4Service de Neurochirurgie, Hôpital d’Instruction des Armées Omar Bongo Ondimba (HIA OBO), Gabon *Corresponding authors: Dr. Bivigou-Mboumba Berthold, PhD, Unité mixte de Recherches sur le VIH et les Maladies Infectieuses Associées (UMR VIH-MIA), Centre Internationale de Recherche Médicale de Franceville (CIRMF), BP: 8507, Libreville, Gabon Abstract Background Background: Extrapulmonary forms of tuberculosis (TB) Tuberculosis (TB) is endemic in sub-Saharan Africa are on the rise in sub-Saharan Africa and pose a major and Asia [1]. It is caused by the Mycobacterium tuber- public health problem. The spine is the most frequent culosis and most commonly affects the lungs. However, location of musculoskeletal tuberculosis. Involvement of the spine causes severe back pain and weakness in the lower in TB endemic countries, extrapulmonary presentations extremities. We report 11 cases of TB spondylodiscitis, are reported frequently and include spinal tuberculo- commonly referred to as Pott's disease, who presented to sis, ganglionic tuberculosis, and urogenital involvement the internal medicine department at the Military Hospital of also known as Pott’s disease. -

Ankylosing Spondylitis Versus Internal Disc Disruption
Case Report iMedPub Journals Spine Research 2017 http://www.imedpub.com/ Vol.3 No.1:4 ISSN 2471-8173 DOI: 10.21767/2471-8173.10004 Ankylosing Spondylitis Versus Internal Disc Disruption: A Case Report Treated Successfully with Intradiscal Platelet-Rich Plasma Injection Richard G Chang, Nicole R Hurwitz, Julian R Harrison, Jennifer Cheng, and Gregory E Lutz Department of Physiatry, Hospital for Special Surgery, New York, USA Rec date: Feb 25, 2017; Acc date: April 7, 2017; Pub date: April 11, 2017 Corresponding author: Gregory E Lutz, Department of Physiatry, Hospital for Special Surgery, New York, USA, E-mail: [email protected] Citation: Chang RG, Hurwitz NR, Harrison JR, et al. Ankylosing Spondylitis Versus Internal Disc Disruption: A Case Report Treated Successfully with Intradiscal Platelet-Rich Plasma Injection. Spine Res 2017, 3: 4. Abbreviations: AS: Ankylosing Spondylitis; IDD: Internal Disc Disruption; IVD: Intervertebral Disc; MRI: Magnetic Abstract Resonance Imaging; NSAID: Non-Steroidal Anti- Inflammatory Drug; PRP: Platelet-Rich Plasma; PSIS: We report the case of a 21-year-old female who Posterior Superior Iliac Spines; SI: Sacroiliac presented with severe disabling low back pain radiating to both buttocks for 1 year. She was initially diagnosed with ankylosing spondylitis (AS) based on her complaints of persistent low back pain with bilateral sacroiliitis found on Introduction magnetic resonance imaging (MRI) of the sacroiliac joints. The differential diagnosis of patients who present with Despite testing negative for HLA-B27 and lack of other positive imaging to support the diagnosis, she was still primarily low back and bilateral buttock pain without any clear treated presumptively as a patient with this disease.