One Year Results of Presbylasik Using Hybrid Bi-Aspheric Micro-Monovision Ablation Profile in Correction of Presbyopia and Myopic Astigmatism
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

PRESBYOND Laser Blended Vision Practical Guide
PRESBYOND Laser Blended Vision Practical Guide Disclaimer: This practical guide was produced independently by Dan Z Reinstein, MD MA(Cantab) FRCSC DABO FRCOphth FEBO1, 2, 3, 4 Glenn I Carp, MBBCh, FC Ophth (SA)1 Timothy J Archer, MA(Oxon), DipCompSci(Cantab)1, 4 Sharon Ritchie, BSc (Hons), MCOptom1 1 London Vision Clinic, London, UK 2 Department of Ophthalmology, Columbia University Medical Center, NY, USA 3 Centre Hospitalier National d’Ophtalmologie, Paris, France 4 Biomedical Science Research Institute, University of Ulster, Coleraine, Northern Ireland Financial Disclosure: Dr Reinstein is a consultant for Carl Zeiss Meditec (Carl Zeiss Meditec AG, Jena, Germany) and has a proprietary interest in the Artemis technology (ArcScan Inc, Golden, Colorado) through patents administered by the Center for Technology Licensing at Cornell University (CTL), Ithaca, New York. Dr Carp receives travel expenses from Carl Zeiss Meditec. The remaining authors have no proprietary or financial interest in the materials presented herein. Preoperative 1. Pre-operative testing protocol 2. Manifest refraction 3. Dominance testing 4. Laser Blended Vision tolerance assessment 5. What myopic target to expect 6. Laser Blended Vision explanation and patient counselling Postoperative 7. Postoperative evaluation 8. Postoperative visual course 9. Cross-blur management at final outcome 10. Appendix A – Preoperative tolerance test examples 11. Appendix B – Postoperative cross-blur and enhancement examples 2 1. Pre-operative testing protocol Highlighted topics are particularly relevant for PRESBYOND • History. Motivation for surgery, previous ocular • Cirrus OCT corneal and epithelial pachymetry. history (including detailed history of contact lens wear, • Undilated WASCA aberrometry. period of wear, type of lens, wear modality, last worn, • Ocular Response Analyser. -
Age-Optimized Vision Correction Laser Blended Vision Modulates Spherical Aberration with Corneal Ablation
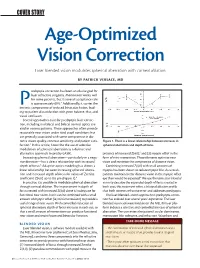
COVER STORY Age-Optimized Vision Correction Laser blended vision modulates spherical aberration with corneal ablation. BY PATRICK VERSACE, MD resbyopia correction has been an elusive goal for laser refractive surgeons. Monovision works well for some patients, but its overall acceptance rate P is approximately 60%.1 Additionally, it carries the intrinsic compromise of reduced binocular fusion, lead- ing to patient dissatisfaction with poor balance, blur, and visual confusion. Several approaches exist for presbyopic laser correc- tion, including multifocal and bifocal corneal optics cre- ated in various patterns. These approaches often provide reasonable near vision under ideal pupil conditions but are generally associated with some compromise in dis- tance vision quality, contrast sensitivity, and patient satis- Figure 1. There is a linear relationship between increases in faction.2 In this article, I describe the use of selective spherical aberration and depth of focus. modulation of spherical aberration as a distinct and alternative approach to presby-LASIK. presence of increased Z(4,0),5 and (3) myopic offset in the Increasing spherical aberration—particularly in a nega- form of mini-monovision. These elements optimize near tive direction—has a direct relationship with increased vision and minimize the compromise of distance vision. depth of focus.3 Adaptive optics modeling has shown a Combining increased Z(4,0) with small amounts of linear relationship between increasing spherical aberra- myopia has been shown to reduce myopic blur. As a result, tion and increased depth of focus for values of Zernike patients maintain better distance vision in the myopic offset coefficient Z(4,0) up to 0.6 µm (Figure 1).4 eye than would be expected.6 We use the term laser blended In practice, it is possible to modulate spherical aberration vision to describe the expanded depth of focus created in through corneal ablation. -

PRESBYOND Laser Blended Vision from ZEISS
CASE STUDIES CASE OF THE MONTH Treatment of presbyopia with Laser Blended Vision to provide a continuous range of station. The procedure compensates for presbyopia by 95% of emmetropes.1-3 Patient satisfaction rates are also combining micro-monovision with a non-linear aspheric high, although if a patient is unhappy for any reason, the ablation profile that induces spherical aberration to in- treatment can be reversed with spectacle wear or even quality vision crease depth of field, and it has many advantages compa- with another laser procedure. Future enhancement is also Liliana Bányai, Dr. medic, Bányai Laser Centre Leonberg, Germany. red with other surgical approaches for reducing spectacle possible to adjust for progressive presbyopia. dependence in presbyopic patients. CONCLUSION PRESBYOND Laser Blended Vision is more attractive I have been using PRESBYOND Laser Blended Vision than clear lens exchange for many patients because it is successfully in my practice to treat presbyopia in pati- CASE HISTORY ness of 110 µm OU in both eyes were created using the less invasive and avoids the risks of intraocular surgery. ents without cataract for 1.5 years, and it is a good choice A 53-year-old male engineer presented requesting a VisuMax® femtosecond laser (Carl Zeiss Meditec AG, Unlike corneal inlay procedures, PRESBYOND Laser for refractive surgeons who are already performing Fem- solution that would give him spectacle independence Jena, Germany). The ablation was performed using the Blended Vision is suitable for patients with a broad to-LASIK because it requires no new skills. As with any for all of his vision needs. -
Chapter 14 Presbyopia Correction
Chapter 14 Presbyopia Correction Introduction ....................................................................................208 Nonsurgical Methods for Correction of Presbyopia............209 Surgical Methods for Correction of Presbyopia ...................210 Laser Assisted Presbyopia Corrections25,26 ........................................................216 Conclusion .......................................................................................217 14. Presbyopia Correction Pulak Agarwal, Chirakshi Dhull, Yogita Gupta, and Sudarshan Khokhar Introduction (AP). Thus, it proposes loss of lens capsule elasticity as the main cause of loss of accommodation. Loss of accommodative amplitude due to aging is known as presbyopia. Symptoms include diminution of vision for near Schachar Theory3 sight, headache, asthenopia, and eye strain. Many plausible mechanisms in the form of theories have It proposes that during ciliary contraction, the tension in been proposed for accommodation (Fig. 14.1), equatorial zonular fibers increases, which leads to steepen- ing of anterior lens capsule. With aging, the distance between Helmholtz Theory1,2 ciliary body and the equatorial lens capsule decreases, which causes ineffective tension generation. Most of the scleral- It proposes that when the ciliary body is relaxed, the based interventions are based on this theory. zonules are stretched, which lead to flattening of anterior lens capsule and decrease in the diameter (AP) of the lens. Catenary Theory As opposed to when the ciliary body contracts, -

Previsit Counseling Is Telling BALAMURALI K
GLOBAL PRACTICE PATTERNS s STRATEGIES FOR CORRECTING PRESBYOPIA | Surgeons share their preferences. Previsit Counseling Is Telling BALAMURALI K. AMBATI, ncreasing maturity (ie, age) comes happens before and after surgery. with reduced focusing adjustment Previsit counseling using Surgiorithm’s MD, PHD, MBA, AND NORALIZ (ie, accommodation). In patients with system has increased the percentage GARCÍA-O’FARRILL, MD cataracts, the restoration of excellent of our patients who elect to undergo visual function can be achieved astigmatic and presbyopia correction Eugene, Oregon Ithrough cataract extraction coupled at the time of cataract surgery from with presbyopia technology. 43% to 53%. This system synergizes educational videos, a lifestyle PREFERENCES AND PROCESSES questionnaire, and information on In the surgical suite. Table 1 shows our available options. preferences for correcting presbyopia. During the preoperative visit, patients preoperative measurements in these Although most presbyopia-correcting learn that they may see rings after eyes and the higher touch-up rate as IOLs can correct only 2.57 D of surgery because of lens-edge effects, will a result. No matter the patient, it is astigmatism, that is not an upper likely have dry eyes for a few months essential to optimize the corneal surface limit because lens technology can be postoperatively, will likely need laser before planning presbyopic cataract combined with intrastromal corneal treatment for scar tissue behind the surgery (Table 2). ring segments, laser arcuate incisions, lens implant in 4 to 12 months after Younger patients without cataracts and limbal relaxing incisions to allow surgery, and may need a free touch-up are offered refractive lens exchange presbyopia correction even in patients for residual astigmatism or refractive (RLE), especially if they have high with 6.00 or 7.00 D of preoperative error. -

Non-Linear Aspheric Ablation Profile for Presbyopic Corneal Treatment Using the Mel80/90 and Crs Master Presbyond Module
NON-LINEAR ASPHERIC ABLATION PROFILE FOR PRESBYOPIC CORNEAL TREATMENT USING THE MEL80/90 AND CRS MASTER PRESBYOND MODULE Dan Z Reinstein, MD MA(Cantab) FRCSC DABO FRCOphth FEBO1,2,3,4 Timothy J Archer, MA(Oxon) DipCompSci(Cantab)1 Glenn I Carp, MBBCh, FC Ophth (SA)1 1 London Vision Clinic, London, UK 2 Biomedical Science Research Institute, Ulster University, Belfast, UK 3 Department of Ophthalmology, Weill Medical College of Cornell University, NY, USA 4 Centre Hospitalier National d’Ophtalmologie, Paris, France Financial disclosure: Dr Reinstein is a consultant for Carl Zeiss Meditec (Jena, Germany) and has a financial interest in ArcScan Inc (Morrison, CO).. The remaining authors have no proprietary or financial interest in the materials presented herein. Correspondence: Dan Z Reinstein, MD MA(Cantab) FRCSC DABO FRCOphth FEBO, London Vision Clinic, 138 Harley Street, London W1G 7LA, United Kingdom. Tel +44 207 224 1005, Fax +44 207 224 1055, email [email protected] Disclaimer: Not all recommendations, treatment ranges and protocols in this document are officially approved or supported by the products intended use. Where relevant, a comment will be made regarding the official intended use. Also, note that not all products, services or offers are approved or offered in every market and approved labeling and instructions may vary from one country to another. 1 Introduction There has recently been a tremendous increase in interest of surgical presbyopic correction. The effective treatment of presbyopia combined with any refractive -

Study of the Orthoptic Assessment in Refractive Eye Surgery
Open Journal of Ophthalmology, 2020, 10, 55-58 https://www.scirp.org/journal/ojoph ISSN Online: 2165-7416 ISSN Print: 2165-7408 Study of the Orthoptic Assessment in Refractive Eye Surgery L. Sabetti1, M. Ciancaglini2, F. Guetti1, L. Laglia1, G. Murano2* 1Department of Biotechnological and Applied Clinical Sciences, University of L’Aquila, L’Aquila, Italy 2Departmente of Life, Health & Environmental Sciences, L’Aquila, Italy How to cite this paper: Sabetti, L., Cian- Abstract caglini, M., Guetti, F., Laglia, L. and Murano, G. (2020) Study of the Orthoptic Assessment Purpose: The aim of our study was to assess the variations in fusion and in Refractive Eye Surgery. Open Journal of stereopsis before and after refractive surgery. Methods: We conducted a retro- Ophthalmology, 10, 55-58. spective study. 140 patients (78 M, 62 F) were selected, aged 20 - 59 years (mean https://doi.org/10.4236/ojoph.2020.101007 age 36 ± 10 DS). All patients received a comprehensive ophtalmological and Received: November 20, 2019 orthoptic examination. Surgery was performed using a MEL-80 excimer laser Accepted: January 5, 2020 (Carl Zeiss Meditec, Jena, Germany). Results. Fusional convergence ampli- Published: January 8, 2020 tudes after refractive eye surgery range from at near 18 - 20 PD in 42 (30%) patients; 25 - 30 PD in 56 (40%) patients; 35 - 40 PD in 42 (30%) patients, at Copyright © 2020 by author(s) and far 20 - 25 PD in 84 (60%) patients; 30 - 40 PD in 56 (40%) patients, fusional Scientific Research Publishing Inc. This work is licensed under the Creative divergence at near after refractive eye surgery range from at near 6 - 8 PD in Commons Attribution International 108 (75.7%) patients; 10 - 12 PD in 52 (37.1%), at far 6 - 8 PD in 126 (90%) License (CC BY 4.0). -
An Advanced Laser Procedure, This Procedure Involves Making a Thin
SURGICAL INFORMATION PACKAGE www.lasikprovision.com 6800 Morrison Street, Unit 4, Niagara Falls, Ontario,L2E 6Z8 Canada 1-888-510-2020 1 Welcome 3 How the Eye Works 3 Nearsightedness 4 Farsightedness 4 Astigmatism 4 Presbyopia 4 Monovision/ Blended Vision 5 Surgical Procedures 6 PRK 6 LASIK 7 Visumax (Blade-Free) 8 Benefits of Blade Free LASIK 9 Potential Complications 9 Laser Technologies 10 Zeiss Mel 80 Excimer Laser 10 Benefits of the Mel 80 11 Benefits of the Mel 80 (continued) 11 Zeiss Mel 80 Clinical Study 12 Allegretto Wavelight 400 HZ Laser 13 Perfect Pulse Technology 14 Eye Tracking Technology 14 Better Night Vision and Glare Control 14 Topolyzer 14 Wavelight Technology 15 Wavefront Optimized 15 Wavefront Guided 15 Topography Guided 15 ICL 16 CLE 16 Candidacy 16 Contact Lens Policy 16 Pre-Operative Assessment 17 Informed Consent 18 What to Expect 19 Before Surgery 19 How to Prepare for the Pre-Operative Assessment 19 Pre-Operative Assessment Day 19 How to Prepare for Surgery 20 Time Off Work Information Table 20 During Surgery 21 Surgery Day 21 After Surgery 21 Immediate Post-Operative Care 21 Follow-up Visits 22 Post-LASIK Activity Schedule 23 Potential Complications 24 LASIK 24 LASIK & PRK 26 PRK 27 Retreatment Policy 28 Eligibility/ Clear Vision Plan 28 Dr. Andrew Taylor Biography 29 Contact Us 30 2 WELCOME! Your vision is a precious commodity, so we appreciate the trust you’ve put in LASIK PROVISON and Dr. Taylor to perform your laser vision correction. We know this procedure has the potential to change your life immensely and this is an exciting time for you, anticipating the comfort of being able to perform daily activities without glasses or contacts. -
The Ebb and Flow of Presbyopic Correction
The Ebb and Flow of Presbyopic Correction Dan Z Reinstein, MD, MA(Cantab), FRCSC, DABO, FRCOphth, FEBO1,2,3 Ryan S Vida, OD, FAAO1 Timothy J Archer, MA(Oxon), DipCompSci(Cantab), PhD1 1. London Vision Clinic, London UK 2. Columbia University Medical Center, New York, NY, USA 3. Sorbonne Université, Paris, France 4. Biomedical Science Research Institute, Ulster University, Coleraine, UK Financial Disclosure • The author (DZ Reinstein) is a consultant for Carl Zeiss Meditec AG (Jena, Germany) • The author (DZ Reinstein) acknowledges a financial interest in Insight 100 VHF digital ultrasound (ArcScan Inc, Golden, CO) ©DZ Reinstein 2019 [email protected] Presbyopic Correction: Cornea & Lens Multifocal Sph Ab EDoF Monovision ©DZ Reinstein 2019 [email protected] Trends in presbyopic correction Full multifocality Reduced Extended DoF + Reduced Full Monovision multifocality µ-anisometropia Monovision OD OS OD OS OD OS OD OS OD OS Distance Challenges Intermediate Monovision Maximise Range of Vision Improve SafetyTolerance & Poor Safety / Low Tolerance Low / Safety Poor Near ©DZ Reinstein 2019 [email protected] Trends in presbyopic correction: Multifocality Full multifocality Reduced Extended DoF + CornealReduced Full Monovision multifocality µ-anisometropia Monovision OD OS OD OS OD OS OD OS OD OS Distance “Multi-focality attempts to substitute the loss of a dynamic system (accommodation) with a static system (multiple foci Challenges in one eye)” Intermediate John Marshall, AECOS 2013 Monovision Maximise Range of Vision -

Walking the Walk: How Laser Blended Vision for Presbyopia Improved My
CASE STUDIES CASE OF THE MONTH gery, I do have a relatively large pupil which he took into clinic’s range of services, so I am optimistic that we will account in the treatment plan and which ensured that I be able to offer it very soon to our patients. In the future, Walking the walk: How laser blended vision for would experience no discomfort in low-light conditions my goal is to develop presbyopia correction surgery into after surgery. Three months after surgery, the uncorrect- the technical specialty of our hospital. This will repre- presbyopia improved my vision and quality of life ed visual acuity for my dominant eye was 1.0 (20/20) sent a valuable addition to our refractive practice and and 0.8 (20/25) for the non-dominant eye. Overall, I feel serve to promote the reputation of our hospital nationally very satisfied with the outcome. If, however, I was to and internationally. By Jiang Haixiang MD highlight one area that could be improved upon, it would probably be my near vision in dim light conditions. My requirements for sharp near vision are probably slight- THE SURGEON’S VIEWPOINT ly higher than most people, while the quality of my far Dr Xingtao Zhou, M.D., Ph.D CASE HISTORY with that modality. With PRESBYOND, I felt confident vision seems to exceed my requirements at present. As As an ophthalmologist with low-grade myopia, I am one that I could achieve even better outcomes: the sophisti- with any refractive procedure, there is always a degree I have been performing procedures with of those eye surgeons who continued to wear glasses cated wavefront laser profile expands the depth of focus of compromise to be found for the range of vision ob- PRESBYOND for over two years now even though other viable treatment options were avail- for each eye while reducing dependence on the patient’s tained at near, far and intermediate distance points. -

Restoring Near and Intermediate Vision with Corneal Excimer Laser
CASE STUDIES CASE OF THE MONTH Restoring near and intermediate vision PRESBYOND LBV, however, accounts for approxi- for as much myopia as possible up to -1.5 D. In my mately one-third of my corneal refractive surgeries and experience, about 95% of patients are able to tolerate with corneal excimer laser surgery about 40% of all of my presbyopic patients. an interocular difference of 0.75 D whereas only about 30% of patients tolerate 1.5 D of anisometropia. Compared with its alternatives, which include refrac- By Pait Teesalu, MD, Tartu, Estonia tive lens exchange with implantation of a presby- CONCLUSION opia-correcting IOL, LASIK monovision, or Presby- We all try to do our best for our patients and that in- LASIK that creates a multifocal cornea, PRESBYOND cludes providing them with accurate information that LBV has several advantages that made it appealing to can help them make an informed decision. Because of me and that are attractive and important for many pa- my experience, I can say with assurance that PRES- CASE HISTORY newsprint at 20 cm. Today, at 12 years after surgery, tients. Patients are already familiar with corneal laser BYOND LBV surgery is a safe and effective way to Twelve years ago when I was 42 years old and tired of my refraction is 0.00 -0.5 X 132° OD and 0.00 -0.5 X surgery because it has been widely marketed to the pub- help appropriately selected non-cataract presbyopic the inconvenience and bother of wearing glasses, I de- 65° OS, and my distance UCVA is still 20/12.5 in each lic, and they tend to be less afraid of it than lens surgery and pre-presbyopic patients who do not want to rely on cided that I wanted to have refractive surgery to correct eye. -
What You Should Know About Laser Blended Vision?
Patient information Patient What you should know about Laser Blended Vision A personalized treatment for patients with presbyopia 2 Optimized visual acuity at all distances for patients with presbyopia Laser Blended Vision Our eyesight is the most valuable of all our senses. We take in the world around us primarily with our eyes. Seeing provides us with information, puts things into perspective and forms our views. As we grow older, bodily functions like our eyesight start to decline. Presbyopia is a common eye condition that affects many people over the age of 40. Thereby, the eye starts to lose its ability to shift focus, causing difficulty when focusing on close objects and blurriness when reading. However, thanks to pioneering medical and technological research in recent years, correction options are available. One of these options is Laser Blended Vision, an advanced Laser Vision Correction procedure for compensating some of the symptoms of presbyopia. It offers several advantages over conventional methods, particularly with respect to the customization of treatment, sharply focused vision at all distances and the immediate impact it provides. Whether Laser Vision Correction is right for you depends on a variety of factors. Your eye doctor will be happy to assist you in finding the best option for your vision needs. 3 Bringing it into focus Understanding presbyopia Presbyopia is the natural regression of vision with age that at different distances. As we age, the lens becomes less usually begins at the age of 40 and older. Similar to a cam- flexible and starts losing its ability to change shape and era lens, the cornea and lens of the human eye bundle the to adjust its focus.