Presbyopic Correction on the Cornea Samuel Arba Mosquera1 and Jorge L Alió2,3*
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Hyperopia Hyperopia
Hyperopia Hyperopia hyperopia hyperopia • Farsightedness, or hyperopia, • Farsightedness occurs if your eyeball is too as it is medically termed, is a short or the cornea has too little curvature, so vision condition in which distant objects are usually light entering your eye is not focused correctly. seen clearly, but close ones do • Its effect varies greatly, depending on the not come into proper focus. magnitude of hyperopia, the age of the individual, • Approximately 25% of the the status of the accommodative and general population is hyperopic (a person having hyperopia). convergence system, and the demands placed on the visual system. By Judith Lee and Gretchyn Bailey; reviewed by Dr. Vance Thompson; Flash illustration by Stephen Bagi 1. Cornea is too flap. hyperopia • In theory, hyperopia is the inability to focus and see the close objects clearly, but in practice many young hyperopics can compensate the weakness of their focusing ability by excessive use of the accommodation functions of their eyes. Hyperopia is a refractive error in • But older hyperopics are not as lucky as them. By which parallel rays of light aging, accommodation range diminishes and for 2. Axial is too short. entering the eye reach a focal older hyperopics seeing close objects becomes point behind the plane of the retina, while accommodation an impossible mission. is maintained in a state of relaxation. 1 Amplitude of Accommodation hyperopia Maximum Amplitude= 25-0.4(age) • An emmetropic eye for reading and other near Probable Amplitude= 18.5-.3(age) work, at distance of 16 in (40cm), the required amount of acc. -

Defining Emmetropia and Ametropia As a Function of Ocular Biometry II
SyntEyes: a Higher Order Statistical Eye Model for Healthy Eyes Jos J. Rozema,*† MSc PhD, Pablo Rodriguez,‡ MSc PhD, Rafael Navarro,‡ MSc PhD, Marie-José Tassignon*†, MD PhD *Dept. of Ophthalmology, Antwerp University Hospital, Edegem, Belgium † Dept. of Medicine and Health Sciences, Antwerp University, Wilrijk, Belgium ‡ICMA, Consejo Superior de Investigaciones Científicas-Universidad de Zaragoza, Facultad de Ciencias, Zaragoza, Spain Abstract Purpose: To present a stochastic eye model that simulates the higher order shape parameters of the eye, as well as their variability and mutual correlations. Methods: The biometry of 312 right eyes of 312 subjects were measured with an autorefractometer, a Scheimpflug camera, an optical biometer and a ray tracing aberrometer. The corneal shape parameters were exported as Zernike coefficients, which were converted into eigenvectors in order to reduce the dimensionality of the model. These remaining 18 parameters were modeled by fitting a sum of two multivariate Gaussians. Based on this fit an unlimited number of synthetic data sets (‘SyntEyes’) can be generated with the same distribution as the original data. After converting the eigenvectors back to the Zernike coefficients, the data may be introduced into ray tracing software. Results: The mean values of nearly all SyntEyes parameters was statistically equal to those of the original data (two one-side t test). The variability of the SyntEyes parameters was the same as for the original data for the most important shape parameters and intraocular distances, but showed significantly lower variability for the higher order shape parameters (F test) due to the eigenvector compression. The same was seen for the correlations between higher order shape parameters. -

PRESBYOND Laser Blended Vision Practical Guide
PRESBYOND Laser Blended Vision Practical Guide Disclaimer: This practical guide was produced independently by Dan Z Reinstein, MD MA(Cantab) FRCSC DABO FRCOphth FEBO1, 2, 3, 4 Glenn I Carp, MBBCh, FC Ophth (SA)1 Timothy J Archer, MA(Oxon), DipCompSci(Cantab)1, 4 Sharon Ritchie, BSc (Hons), MCOptom1 1 London Vision Clinic, London, UK 2 Department of Ophthalmology, Columbia University Medical Center, NY, USA 3 Centre Hospitalier National d’Ophtalmologie, Paris, France 4 Biomedical Science Research Institute, University of Ulster, Coleraine, Northern Ireland Financial Disclosure: Dr Reinstein is a consultant for Carl Zeiss Meditec (Carl Zeiss Meditec AG, Jena, Germany) and has a proprietary interest in the Artemis technology (ArcScan Inc, Golden, Colorado) through patents administered by the Center for Technology Licensing at Cornell University (CTL), Ithaca, New York. Dr Carp receives travel expenses from Carl Zeiss Meditec. The remaining authors have no proprietary or financial interest in the materials presented herein. Preoperative 1. Pre-operative testing protocol 2. Manifest refraction 3. Dominance testing 4. Laser Blended Vision tolerance assessment 5. What myopic target to expect 6. Laser Blended Vision explanation and patient counselling Postoperative 7. Postoperative evaluation 8. Postoperative visual course 9. Cross-blur management at final outcome 10. Appendix A – Preoperative tolerance test examples 11. Appendix B – Postoperative cross-blur and enhancement examples 2 1. Pre-operative testing protocol Highlighted topics are particularly relevant for PRESBYOND • History. Motivation for surgery, previous ocular • Cirrus OCT corneal and epithelial pachymetry. history (including detailed history of contact lens wear, • Undilated WASCA aberrometry. period of wear, type of lens, wear modality, last worn, • Ocular Response Analyser. -

Posterior Vitreous Detachment As Observed by Wide-Angle OCT Imaging
Posterior Vitreous Detachment as Observed by Wide-Angle OCT Imaging Mayuka Tsukahara, OD,1,* Keiko Mori, MD,1 Peter L. Gehlbach, MD, PhD,2 Keisuke Mori, MD, PhD1,3,4,* Purpose: Posterior vitreous detachment (PVD) plays an important role in vitreoretinal interface disorders. Historically, observations of PVD using OCT have been limited to the macular region. The purpose of this study is to image the wide-angle vitreoretinal interface after PVD in normal subjects using montaged OCT images. Design: An observational cross-sectional study. Participants: A total of 144 healthy eyes of 98 normal subjects aged 21 to 95 years (51.4Æ22.0 [mean Æ standard deviation]). Methods: Montaged images of horizontal and vertical OCT scans through the fovea were obtained in each subject. Main Outcome Measures: Montaged OCT images. Results: By using wide-angle OCT, we imaged the vitreoretinal interface from the macula to the periphery. PVD was classified into 5 stages: stage 0, no PVD (2 eyes, both aged 21 years); stage 1, peripheral PVD limited to paramacular to peripheral zones (88 eyes, mean age 38.9Æ16.2 years, mean Æ standard deviation); stage 2, perifoveal PVD extending to the periphery (12 eyes, mean age 67.9Æ8.4 years); stage 3, peripapillary PVD with persistent vitreopapillary adhesion alone (7 eyes, mean age 70.9Æ11.9 years); stage 4, complete PVD (35 eyes, mean age 75.1Æ10.1 years). All stage 1 PVDs (100%) were observed in the paramacular to peripheral region where the vitreous gel adheres directly to the cortical vitreous and retinal surface. After progression to stage 2 PVD, the area of PVD extends posteriorly to the perifovea and anteriorly to the periphery. -
Age-Optimized Vision Correction Laser Blended Vision Modulates Spherical Aberration with Corneal Ablation
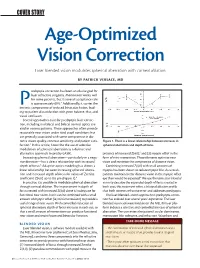
COVER STORY Age-Optimized Vision Correction Laser blended vision modulates spherical aberration with corneal ablation. BY PATRICK VERSACE, MD resbyopia correction has been an elusive goal for laser refractive surgeons. Monovision works well for some patients, but its overall acceptance rate P is approximately 60%.1 Additionally, it carries the intrinsic compromise of reduced binocular fusion, lead- ing to patient dissatisfaction with poor balance, blur, and visual confusion. Several approaches exist for presbyopic laser correc- tion, including multifocal and bifocal corneal optics cre- ated in various patterns. These approaches often provide reasonable near vision under ideal pupil conditions but are generally associated with some compromise in dis- tance vision quality, contrast sensitivity, and patient satis- Figure 1. There is a linear relationship between increases in faction.2 In this article, I describe the use of selective spherical aberration and depth of focus. modulation of spherical aberration as a distinct and alternative approach to presby-LASIK. presence of increased Z(4,0),5 and (3) myopic offset in the Increasing spherical aberration—particularly in a nega- form of mini-monovision. These elements optimize near tive direction—has a direct relationship with increased vision and minimize the compromise of distance vision. depth of focus.3 Adaptive optics modeling has shown a Combining increased Z(4,0) with small amounts of linear relationship between increasing spherical aberra- myopia has been shown to reduce myopic blur. As a result, tion and increased depth of focus for values of Zernike patients maintain better distance vision in the myopic offset coefficient Z(4,0) up to 0.6 µm (Figure 1).4 eye than would be expected.6 We use the term laser blended In practice, it is possible to modulate spherical aberration vision to describe the expanded depth of focus created in through corneal ablation. -

PRESBYOND Laser Blended Vision from ZEISS
CASE STUDIES CASE OF THE MONTH Treatment of presbyopia with Laser Blended Vision to provide a continuous range of station. The procedure compensates for presbyopia by 95% of emmetropes.1-3 Patient satisfaction rates are also combining micro-monovision with a non-linear aspheric high, although if a patient is unhappy for any reason, the ablation profile that induces spherical aberration to in- treatment can be reversed with spectacle wear or even quality vision crease depth of field, and it has many advantages compa- with another laser procedure. Future enhancement is also Liliana Bányai, Dr. medic, Bányai Laser Centre Leonberg, Germany. red with other surgical approaches for reducing spectacle possible to adjust for progressive presbyopia. dependence in presbyopic patients. CONCLUSION PRESBYOND Laser Blended Vision is more attractive I have been using PRESBYOND Laser Blended Vision than clear lens exchange for many patients because it is successfully in my practice to treat presbyopia in pati- CASE HISTORY ness of 110 µm OU in both eyes were created using the less invasive and avoids the risks of intraocular surgery. ents without cataract for 1.5 years, and it is a good choice A 53-year-old male engineer presented requesting a VisuMax® femtosecond laser (Carl Zeiss Meditec AG, Unlike corneal inlay procedures, PRESBYOND Laser for refractive surgeons who are already performing Fem- solution that would give him spectacle independence Jena, Germany). The ablation was performed using the Blended Vision is suitable for patients with a broad to-LASIK because it requires no new skills. As with any for all of his vision needs. -

Distance Vision, Near Vision and Quality of Life Between Preferred Emmetropia and Residual Myopia in Monofocal Intraocular Lens Implantation - a Comparative Study
10-Comparative00212_3-PRIMARY.qxd 5/13/21 10:29 PM Page 340 ORIGINAL ARTICLE Distance vision, near vision and quality of life between preferred emmetropia and residual myopia in monofocal intraocular lens implantation - A Comparative study Jaafar Juanarita, MMed 1,2,3 , Abdul Rahman Siti-Khadijah, MBBS 1,2 , Bakiah Shaharuddin, PhD 4, Yaakub Azhany, MMed 1,2 1Department of Ophthalmology and Visual Sciences, School of Medical Sciences, Universiti Sains Malaysia, Kubang Kerian, Kelantan, Malaysia, 2Ophthalmology Clinic, Hospital Universiti Sains Malaysia, Kubang Kerian, Kelantan, Malaysia, 3Hospital Sultanah Bahiyah, Alor Setar, Alor Setar, Kedah, 4Advanced Medical and Dental Institute, Universiti Sains Malaysia, Kepala Batas, Penang, Malaysia unoperated cataracts. 2 Currently, there is no effective ABSTRACT prevention for cataracts, and the only treatment is to remove Introduction: This study was done to evaluate the visual the cloudy lens. 3 acuity and quality of life in predicted emmetropia (EM) and predicted residual myopia (RM) patients following Intraocular lens (IOL) implantation is the commonest phacoemulsification with monofocal intraocular lens practice of visual rehabilitation after cataract surgery. implantation. Monofocal or fixed focal IOLs have only one focus at distance; thus, the placement of a monofocal IOL requires Materials and Methods: This prospective comparative study corrective lenses (spectacles) after surgery for near vision- was conducted in the ophthalmology clinic of the Universiti related tasks. Although no statistical difference was found Sains Malaysia Hospital, Kelantan, Malaysia. Overall, 139 between multifocal (MFIOL) and monofocal IOL with respect patients with senile cataract were randomised into EM and to achieving a post-operative best-corrected visual acuity RM groups. At three months post-operatively, patients were (BCVA) of 6/6, near vision was often found to be better with assessed for distance and near vision, as well as quality of MFIOL. -
Chapter 14 Presbyopia Correction
Chapter 14 Presbyopia Correction Introduction ....................................................................................208 Nonsurgical Methods for Correction of Presbyopia............209 Surgical Methods for Correction of Presbyopia ...................210 Laser Assisted Presbyopia Corrections25,26 ........................................................216 Conclusion .......................................................................................217 14. Presbyopia Correction Pulak Agarwal, Chirakshi Dhull, Yogita Gupta, and Sudarshan Khokhar Introduction (AP). Thus, it proposes loss of lens capsule elasticity as the main cause of loss of accommodation. Loss of accommodative amplitude due to aging is known as presbyopia. Symptoms include diminution of vision for near Schachar Theory3 sight, headache, asthenopia, and eye strain. Many plausible mechanisms in the form of theories have It proposes that during ciliary contraction, the tension in been proposed for accommodation (Fig. 14.1), equatorial zonular fibers increases, which leads to steepen- ing of anterior lens capsule. With aging, the distance between Helmholtz Theory1,2 ciliary body and the equatorial lens capsule decreases, which causes ineffective tension generation. Most of the scleral- It proposes that when the ciliary body is relaxed, the based interventions are based on this theory. zonules are stretched, which lead to flattening of anterior lens capsule and decrease in the diameter (AP) of the lens. Catenary Theory As opposed to when the ciliary body contracts, -

Previsit Counseling Is Telling BALAMURALI K
GLOBAL PRACTICE PATTERNS s STRATEGIES FOR CORRECTING PRESBYOPIA | Surgeons share their preferences. Previsit Counseling Is Telling BALAMURALI K. AMBATI, ncreasing maturity (ie, age) comes happens before and after surgery. with reduced focusing adjustment Previsit counseling using Surgiorithm’s MD, PHD, MBA, AND NORALIZ (ie, accommodation). In patients with system has increased the percentage GARCÍA-O’FARRILL, MD cataracts, the restoration of excellent of our patients who elect to undergo visual function can be achieved astigmatic and presbyopia correction Eugene, Oregon Ithrough cataract extraction coupled at the time of cataract surgery from with presbyopia technology. 43% to 53%. This system synergizes educational videos, a lifestyle PREFERENCES AND PROCESSES questionnaire, and information on In the surgical suite. Table 1 shows our available options. preferences for correcting presbyopia. During the preoperative visit, patients preoperative measurements in these Although most presbyopia-correcting learn that they may see rings after eyes and the higher touch-up rate as IOLs can correct only 2.57 D of surgery because of lens-edge effects, will a result. No matter the patient, it is astigmatism, that is not an upper likely have dry eyes for a few months essential to optimize the corneal surface limit because lens technology can be postoperatively, will likely need laser before planning presbyopic cataract combined with intrastromal corneal treatment for scar tissue behind the surgery (Table 2). ring segments, laser arcuate incisions, lens implant in 4 to 12 months after Younger patients without cataracts and limbal relaxing incisions to allow surgery, and may need a free touch-up are offered refractive lens exchange presbyopia correction even in patients for residual astigmatism or refractive (RLE), especially if they have high with 6.00 or 7.00 D of preoperative error. -

Immersion A-Scan Compared with Partial Coherence Interferometry Outcomes Analysis
Immersion A-scan compared with partial coherence interferometry Outcomes analysis Mark Packer, MD, I. Howard Fine, MD, Richard S. Hoffman, MD, Peggy G. Coffman, COT, Laurie K. Brown, COMT, COE ABSTRACT Purpose: To compare 2 methods of axial length measurement, immersion ultrasonogra- phy and partial coherence interferometry, and to elucidate surgical outcomes based on immersion measurements. Setting: Oregon Eye Institute, Eugene, Oregon, USA. Methods: Axial length measurements in 50 cataractous eyes were obtained by optical biometry (IOLMasterா, Zeiss Humphrey Systems) and immersion ultrasound (Axis II, Quantel Medical), and the results were compared. Intraocular lens (IOL) power calcu- lations in the same eyes after cataract extraction and posterior chamber IOL implanta- tion were evaluated retrospectively based on the postoperative spherical equivalent prediction error. Results: Immersion ultrasonography and partial coherence interferometry measurements correlated in a highly positive manner (correlation coefficient ϭ 0.996). Outcomes analysis demonstrated 92.0% of eyes were within Ϯ0.5 diopter of emmetropia based on immersion axial length measurements. Conclusion: Immersion ultrasonography provided highly accurate axial length measure- ments and permitted highly accurate IOL power calculations. J Cataract Refract Surg 2002; 28:239–242 © 2002 ASCRS and ESCRS xial length measurement remains an indispensable mersion technique.2 Reportedly “user-friendly” and less A technique for intraocular lens (IOL) power calcu- dependent on technician expertise than ultrasound lation. Recently, partial coherence interferometry has methods, noncontact optical biometry is, however, lim- emerged as a new modality for biometry.1 Postoperative ited by dense media, eg, posterior subcapsular cataract. results achieved with this modality have been considered A second limitation of the optical method is the lack of “analogous” to those achieved with the ultrasound im- a lens thickness measurement, a required variable in the Holladay 2 IOL power calculation software, version 2.30.9705. -

Training Eye Instructions
Training Eye Instructions Using the Direct Ophthalmoscope with the Model Eye The Model Eye uses a single plastic lens in place of the cornea and crystalline lens of the real eye (Fig. 20). The lens is mounted at one end of an open plastic tube into which another tube holding the “retina” is inserted. The model eye also has two different pupil sizes (2, and 4 mm in diameter) that are selected by moving the plastic pupil strip left or right. Taking the pupil strip out completely provides a pupil diameter of 8 mm. pupil strip outside tube convex lens velcro "retina" inside sliding tube Fig. 20. Cross-section of the Model Eye. Assembling the Model Eye Each Model Eye kit contains: Stand Outer tube that mounts on the stand Inner tube that slides into the outer tube Pupil strip 6 black plastic disks 5 images of retinas and 1 mm grid with double-stick tape on back 1 cross hair focus disk Attach the large, outer tube to the stand by pressing the black V-shaped plastic attached to the tube over the clear plastic ball on the stand. Next, insert the smaller-diameter inner tube into the Model Eye. EXPERIMENT 1: Emmetropia In a normal, emmetropic eye, parallel rays of light from a distant object come to focus on the retina (Fig. 21A). Light rays are “reversible”, that is they travel the same path whether going into or out of an optical system. Consequently, if the retina of an emmetropic eye could “light up”, light rays from a point on the retina would exit the eye as parallel rays (Fig. -

Non-Linear Aspheric Ablation Profile for Presbyopic Corneal Treatment Using the Mel80/90 and Crs Master Presbyond Module
NON-LINEAR ASPHERIC ABLATION PROFILE FOR PRESBYOPIC CORNEAL TREATMENT USING THE MEL80/90 AND CRS MASTER PRESBYOND MODULE Dan Z Reinstein, MD MA(Cantab) FRCSC DABO FRCOphth FEBO1,2,3,4 Timothy J Archer, MA(Oxon) DipCompSci(Cantab)1 Glenn I Carp, MBBCh, FC Ophth (SA)1 1 London Vision Clinic, London, UK 2 Biomedical Science Research Institute, Ulster University, Belfast, UK 3 Department of Ophthalmology, Weill Medical College of Cornell University, NY, USA 4 Centre Hospitalier National d’Ophtalmologie, Paris, France Financial disclosure: Dr Reinstein is a consultant for Carl Zeiss Meditec (Jena, Germany) and has a financial interest in ArcScan Inc (Morrison, CO).. The remaining authors have no proprietary or financial interest in the materials presented herein. Correspondence: Dan Z Reinstein, MD MA(Cantab) FRCSC DABO FRCOphth FEBO, London Vision Clinic, 138 Harley Street, London W1G 7LA, United Kingdom. Tel +44 207 224 1005, Fax +44 207 224 1055, email [email protected] Disclaimer: Not all recommendations, treatment ranges and protocols in this document are officially approved or supported by the products intended use. Where relevant, a comment will be made regarding the official intended use. Also, note that not all products, services or offers are approved or offered in every market and approved labeling and instructions may vary from one country to another. 1 Introduction There has recently been a tremendous increase in interest of surgical presbyopic correction. The effective treatment of presbyopia combined with any refractive