PED-1407 – Pediatric Mental Health
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Neurotransmitter Resource Guide
NEUROTRANSMITTER RESOURCE GUIDE Science + Insight doctorsdata.com Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE Table of Contents Sample Report Sample Report ........................................................................................................................................................................... 1 Analyte Considerations Phenylethylamine (B-phenylethylamine or PEA) ................................................................................................. 1 Tyrosine .......................................................................................................................................................................................... 3 Tyramine ........................................................................................................................................................................................4 Dopamine .....................................................................................................................................................................................6 3, 4-Dihydroxyphenylacetic Acid (DOPAC) ............................................................................................................... 7 3-Methoxytyramine (3-MT) ............................................................................................................................................... 9 Norepinephrine ........................................................................................................................................................................ -

Methylphenidate Hydrochloride
Application for Inclusion to the 22nd Expert Committee on the Selection and Use of Essential Medicines: METHYLPHENIDATE HYDROCHLORIDE December 7, 2018 Submitted by: Patricia Moscibrodzki, M.P.H., and Craig L. Katz, M.D. The Icahn School of Medicine at Mount Sinai Graduate Program in Public Health New York NY, United States Contact: [email protected] TABLE OF CONTENTS Page 3 Summary Statement Page 4 Focal Point Person in WHO Page 5 Name of Organizations Consulted Page 6 International Nonproprietary Name Page 7 Formulations Proposed for Inclusion Page 8 International Availability Page 10 Listing Requested Page 11 Public Health Relevance Page 13 Treatment Details Page 19 Comparative Effectiveness Page 29 Comparative Safety Page 41 Comparative Cost and Cost-Effectiveness Page 45 Regulatory Status Page 48 Pharmacoepial Standards Page 49 Text for the WHO Model Formulary Page 52 References Page 61 Appendix – Letters of Support 2 1. Summary Statement of the Proposal for Inclusion of Methylphenidate Methylphenidate (MPH), a central nervous system (CNS) stimulant, of the phenethylamine class, is proposed for inclusion in the WHO Model List of Essential Medications (EML) & the Model List of Essential Medications for Children (EMLc) for treatment of Attention-Deficit/Hyperactivity Disorder (ADHD) under ICD-11, 6C9Z mental, behavioral or neurodevelopmental disorder, disruptive behavior or dissocial disorders. To date, the list of essential medications does not include stimulants, which play a critical role in the treatment of psychotic disorders. Methylphenidate is proposed for inclusion on the complimentary list for both children and adults. This application provides a systematic review of the use, efficacy, safety, availability, and cost-effectiveness of methylphenidate compared with other stimulant (first-line) and non-stimulant (second-line) medications. -

Free PDF Download
European Review for Medical and Pharmacological Sciences 2019; 23: 3-15 Use of cognitive enhancers: methylphenidate and analogs J. CARLIER1, R. GIORGETTI2, M.R. VARÌ3, F. PIRANI2, G. RICCI4, F.P. BUSARDÒ2 1Unit of Forensic Toxicology, Sapienza University of Rome, Rome, Italy 2Section of Legal Medicine, Universita Politecnica delle Marche, Ancona, Italy 3National Centre on Addiction and Doping, Istituto Superiore di Sanità, Rome, Italy 4School of Law, University of Camerino, Camerino, Italy Abstract. – OBJECTIVE: In the last decades, phenidate analogs should be undertaken to re- several cognitive-enhancing drugs have been duce the uprising threat, and education efforts sold onto the drug market. Methylphenidate and should be made among high-risk populations. analogs represent a sub-class of these new psy- choactive substances (NPS). We aimed to re- Key Words: view the use and misuse of methylphenidate and Cognitive enhancers, Methylphenidate, Ritalin, Eth- analogs, and the risk associated. Moreover, we ylphenidate, Methylphenidate analogs, New psycho- exhaustively reviewed the scientific data on the active substances. most recent methylphenidate analogs (methyl- phenidate and ethylphenidate excluded). MATERIALS AND METHODS: Literature Introduction search was performed on methylphenidate and analogs, using specialized search engines ac- cessing scientific databases. Additional reports Consumption of various pharmaceutical drugs were retrieved from international agencies, in- by healthy individuals in an attempt to improve stitutional websites, and drug user forums. cognitive faculties is on the rise, whether for aca- RESULTS: Methylphenidate/Ritalin has been demic or recreational purposes1. These substances used for decades to treat attention deficit disor- are stimulants that preferentially target the cate- ders and narcolepsy. More recently, it has been used as a cognitive enhancer and a recreation- cholamines of the prefrontal cortex of the brain to al drug. -

FSI-D-16-00226R1 Title
Elsevier Editorial System(tm) for Forensic Science International Manuscript Draft Manuscript Number: FSI-D-16-00226R1 Title: An overview of Emerging and New Psychoactive Substances in the United Kingdom Article Type: Review Article Keywords: New Psychoactive Substances Psychostimulants Lefetamine Hallucinogens LSD Derivatives Benzodiazepines Corresponding Author: Prof. Simon Gibbons, Corresponding Author's Institution: UCL School of Pharmacy First Author: Simon Gibbons Order of Authors: Simon Gibbons; Shruti Beharry Abstract: The purpose of this review is to identify emerging or new psychoactive substances (NPS) by undertaking an online survey of the UK NPS market and to gather any data from online drug fora and published literature. Drugs from four main classes of NPS were identified: psychostimulants, dissociative anaesthetics, hallucinogens (phenylalkylamine-based and lysergamide-based materials) and finally benzodiazepines. For inclusion in the review the 'user reviews' on drugs fora were selected based on whether or not the particular NPS of interest was used alone or in combination. NPS that were use alone were considered. Each of the classes contained drugs that are modelled on existing illegal materials and are now covered by the UK New Psychoactive Substances Bill in 2016. Suggested Reviewers: Title Page (with authors and addresses) An overview of Emerging and New Psychoactive Substances in the United Kingdom Shruti Beharry and Simon Gibbons1 Research Department of Pharmaceutical and Biological Chemistry UCL School of Pharmacy -

(Ssris) SEROTONIN and NOREPHINEPHRINE REUPTAKE INHIBITORS DOPAMINE and NOREPINEPHRINE RE
VA / DOD DEPRESSION PRACTICE GUIDELINE PROVIDER CARE CARD ANTIDEPRESSANT MEDICATION TABLE CARD 7 Refer to pharmaceutical manufacturer’s literature for full prescribing information SEROTONIN SELECTIVE REUPTAKE INHIBITORS (SSRIs) GENERIC BRAND NAME ADULT STARTING DOSE MAX EXCEPTION SAFETY MARGIN TOLERABILITY EFFICACY SIMPLICITY Citalopram Celexa 20 mg 60 mg Reduce dose Nausea, insomnia, Fluoxetine Prozac 20 mg 80 mg for the elderly & No serious systemic sedation, those with renal toxicity even after headache, fatigue Paroxetine Paxil 20 mg 50 mg or hepatic substantial overdose. dizziness, sexual AM daily dosing. failure Drug interactions may dysfunction Response rate = Can be started at Sertraline Zoloft 50 mg 200 mg include tricyclic anorexia, weight 2 - 4 wks an effective dose First Line Antidepressant Medication antidepressants, loss, sweating, GI immediately. Drugs of this class differ substantially in safety, tolerability and simplicity when used in patients carbamazepine & distress, tremor, warfarin. restlessness, on other medications. Can work in TCA (tricyclic antidepressant) nonresponders. Useful in agitation, anxiety. several anxiety disorders. Taper gradually when discontinuing these medications. SEROTONIN and NOREPHINEPHRINE REUPTAKE INHIBITORS GENERIC BRAND NAME ADULT STARTING DOSE MAX EXCEPTION SAFETY MARGIN TOLERABILITY EFFICACY SIMPLICITY Reduce dose Take with food. Venlafaxine IR Effexor IR 75 mg 375 mg Comparable to BID or TID for the elderly & No serious systemic SSRIs at low dose. dosing with IR. those with renal toxicity. Nausea, dry mouth, Response rate = Daily dosing or hepatic Downtaper slowly to Venlafaxine XR Effexor XR 75 mg 375 mg insomnia, anxiety, 2 - 4 wks with XR. failure prevent clinically somnolence, head- (4 - 7 days at Can be started at significant withdrawal ache, dizziness, ~300 mg/day) an effective dose Dual action drug that predominantly acts like a Serotonin Selective Reuptake inhibitor at low syndrome. -

Methylphenidate Amplifies the Potency and Reinforcing Effects Of
ARTICLE Received 1 Aug 2013 | Accepted 7 Oct 2013 | Published 5 Nov 2013 DOI: 10.1038/ncomms3720 Methylphenidate amplifies the potency and reinforcing effects of amphetamines by increasing dopamine transporter expression Erin S. Calipari1, Mark J. Ferris1, Ali Salahpour2, Marc G. Caron3 & Sara R. Jones1 Methylphenidate (MPH) is commonly diverted for recreational use, but the neurobiological consequences of exposure to MPH at high, abused doses are not well defined. Here we show that MPH self-administration in rats increases dopamine transporter (DAT) levels and enhances the potency of MPH and amphetamine on dopamine responses and drug-seeking behaviours, without altering cocaine effects. Genetic overexpression of the DAT in mice mimics these effects, confirming that MPH self-administration-induced increases in DAT levels are sufficient to induce the changes. Further, this work outlines a basic mechanism by which increases in DAT levels, regardless of how they occur, are capable of increasing the rewarding and reinforcing effects of select psychostimulant drugs, and suggests that indivi- duals with elevated DAT levels, such as ADHD sufferers, may be more susceptible to the addictive effects of amphetamine-like drugs. 1 Department of Physiology and Pharmacology, Wake Forest University School of Medicine, Winston-Salem, North Carolina 27157, USA. 2 Department of Pharmacology and Toxicology, University of Toronto, Toronto, Ontario, Canada M5S1A8. 3 Department of Cell Biology, Medicine and Neurobiology, Duke University Medical Center, Durham, North Carolina 27710, USA. Correspondence and requests for materials should be addressed to S.R.J. (email: [email protected]). NATURE COMMUNICATIONS | 4:2720 | DOI: 10.1038/ncomms3720 | www.nature.com/naturecommunications 1 & 2013 Macmillan Publishers Limited. -

Clomipramine | Memorial Sloan Kettering Cancer Center
PATIENT & CAREGIVER EDUCATION Clomipramine This information from Lexicomp® explains what you need to know about this medication, including what it’s used for, how to take it, its side effects, and when to call your healthcare provider. Brand Names: US Anafranil Brand Names: Canada Anafranil; MED ClomiPRAMINE; TARO-Clomipramine Warning Drugs like this one have raised the chance of suicidal thoughts or actions in children and young adults. The risk may be greater in people who have had these thoughts or actions in the past. All people who take this drug need to be watched closely. Call the doctor right away if signs like low mood (depression), nervousness, restlessness, grouchiness, panic attacks, or changes in mood or actions are new or worse. Call the doctor right away if any thoughts or actions of suicide occur. This drug is not approved for use in all children. Talk with the doctor to be sure that this drug is right for your child. What is this drug used for? It is used to treat obsessive-compulsive problems. It may be given to you for other reasons. Talk with the doctor. Clomipramine 1/8 What do I need to tell my doctor BEFORE I take this drug? If you have an allergy to clomipramine or any other part of this drug. If you are allergic to this drug; any part of this drug; or any other drugs, foods, or substances. Tell your doctor about the allergy and what signs you had. If you have had a recent heart attack. If you are taking any of these drugs: Linezolid or methylene blue. -

(19) United States (12) Patent Application Publication (10) Pub
US 20130289061A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2013/0289061 A1 Bhide et al. (43) Pub. Date: Oct. 31, 2013 (54) METHODS AND COMPOSITIONS TO Publication Classi?cation PREVENT ADDICTION (51) Int. Cl. (71) Applicant: The General Hospital Corporation, A61K 31/485 (2006-01) Boston’ MA (Us) A61K 31/4458 (2006.01) (52) U.S. Cl. (72) Inventors: Pradeep G. Bhide; Peabody, MA (US); CPC """"" " A61K31/485 (201301); ‘4161223011? Jmm‘“ Zhu’ Ansm’ MA. (Us); USPC ......... .. 514/282; 514/317; 514/654; 514/618; Thomas J. Spencer; Carhsle; MA (US); 514/279 Joseph Biederman; Brookline; MA (Us) (57) ABSTRACT Disclosed herein is a method of reducing or preventing the development of aversion to a CNS stimulant in a subject (21) App1_ NO_; 13/924,815 comprising; administering a therapeutic amount of the neu rological stimulant and administering an antagonist of the kappa opioid receptor; to thereby reduce or prevent the devel - . opment of aversion to the CNS stimulant in the subject. Also (22) Flled' Jun‘ 24’ 2013 disclosed is a method of reducing or preventing the develop ment of addiction to a CNS stimulant in a subj ect; comprising; _ _ administering the CNS stimulant and administering a mu Related U‘s‘ Apphcatlon Data opioid receptor antagonist to thereby reduce or prevent the (63) Continuation of application NO 13/389,959, ?led on development of addiction to the CNS stimulant in the subject. Apt 27’ 2012’ ?led as application NO_ PCT/US2010/ Also disclosed are pharmaceutical compositions comprising 045486 on Aug' 13 2010' a central nervous system stimulant and an opioid receptor ’ antagonist. -

Selective Serotonin Reuptake Inhibitors, Fluoxetine and Paroxetine, Attenuate the Expression of the Established Behavioral Sensitization Induced by Methamphetamine
Neuropsychopharmacology (2007) 32, 658–664 & 2007 Nature Publishing Group All rights reserved 0893-133X/07 $30.00 www.neuropsychopharmacology.org Selective Serotonin Reuptake Inhibitors, Fluoxetine and Paroxetine, Attenuate the Expression of the Established Behavioral Sensitization Induced by Methamphetamine 1 1 1 1 1 ,1 Yujiro Kaneko , Atsushi Kashiwa , Takashi Ito , Sumikazu Ishii , Asami Umino and Toru Nishikawa* 1 Section of Psychiatry and Behavioral Sciences, Tokyo Medical and Dental University Graduate School, Yushima, Bunkyo-ku, Tokyo, Japan To obtain an insight into the development of a new pharmacotherapy that prevents the treatment-resistant relapse of psychostimulant- induced psychosis and schizophrenia, we have investigated in the mouse the effects of selective serotonin reuptake inhibitors (SSRI), fluoxetine (FLX) and paroxetine (PRX), on the established sensitization induced by methamphetamine (MAP), a model of the relapse of these psychoses, because the modifications of the brain serotonergic transmission have been reported to antagonize the sensitization phenomenon. In agreement with previous reports, repeated MAP treatment (1.0 mg/kg a day, subcutaneously (s.c.)) for 10 days induced a long-lasting enhancement of the increasing effects of a challenge dose of MAP (0.24 mg/kg, s.c.) on motor activity on day 12 or 29 of withdrawal. The daily injection of FLX (10 mg/kg, s.c.) or PRX (8 mg/kg, s.c.) from 12 to 16 days of withdrawal of repeated MAP administration markedly attenuated the ability of the MAP pretreatment to augment the motor responses to the challenge dose of the stimulant 13 days after the SSRI injection. The repeated treatment with FLX or PRX alone failed to affect the motor stimulation following the challenge of saline and MAP 13 days later. -

Methamphetamine (Canadian Drug Summary)
www.ccsa.ca • www.ccdus.ca March 2020 Canadian Drug Summary Methamphetamine Key Points • The prevalence of methamphetamine use in the Canadian population is low (~0.2%). • Several jurisdictions report at least a three-fold increase in the use of methamphetamine over the past five years among individuals accessing treatment or harm reduction services. • Notable increases for rates of criminal violations involving methamphetamine have been observed in the last five years (2013–2018). Introduction Methamphetamine is a synthetic drug classified as a central nervous system (CNS) stimulant or psychostimulant. CNS stimulants cover a wide range of substances that act on the body by increasing the level of activity of the CNS and include caffeine, nicotine, amphetamine (e.g., Adderall®), methylphenidate (e.g., Ritalin®), MDMA (“ecstasy”), cocaine (including crack cocaine) and methamphetamine (including crystal meth).1,2 While both methamphetamine and amphetamine are psychostimulants and often grouped together, they are different drugs. A slight chemical modification of amphetamine produces methamphetamine, which has a different pharmacological profile that results in a larger release of certain neurochemicals in the brain and a stronger and more rapid physiological response. Some amphetamines are prescribed in Canada for attention-deficit hyperactivity disorder (ADHD) and narcolepsy (e.g., Adderall and Vyvanse®), but methamphetamine use is currently illegal. Methamphetamine is often made in illegal, clandestine laboratories with commonly available, inexpensive chemicals, such as ephedrine and pseudoephedrine, found in medications, among other sources. The use of these medications as precursor chemicals for methamphetamine led to stricter regulations introduced in Canada in 2006, limiting access to them by requiring they be kept behind the counter of pharmacies.3 Illegal production can be dangerous due to the toxicity of the chemicals used and the high risk of explosions. -
Enhanced Reporting
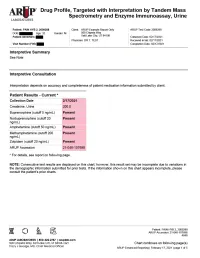
Drug Profile, Targeted with Interpretation by Tandem Mass Spectrometry and Enzyme Immunoassay, Urine Patient: PAIN HYB 2, 2009288 | Date of Birth: | Gender: M | Physician: DR T. TEST Patient Identifiers: | Visit Number (FIN): Drug Analyte Result Cutoff Notes Meperidine metabolite Not Detected 50 ng/mL normeperidine Tapentadol Not Detected 100 ng/mL --Tapentadol-o-sulfate Not Detected 200 ng/mL tapentadol metabolite AMPHETAMINE-LIKE, MASS SPEC Amphetamine Present 50 ng/mL eg, Vyvanse; also a metabolite of methamphetamine Methamphetamine Present 200 ng/mL d- and l- isomers are not distinguished by this test; may reflect Vicks inhaler, Desoxyn, Selegiline, or illicit source MDMA - Ecstasy Not Detected 200 ng/mL MDA Not Detected 200 ng/mL also a metabolite of MDMA and MDEA MDEA - Eve Not Detected 200 ng/mL Phentermine Not Detected 100 ng/mL Methylphenidate Not Detected 100 ng/mL eg, Ritalin, Dexmethylphenidate, Focalin, Concerta BENZODIAZEPINE-LIKE, MASS SPEC Alprazolam Not Detected 40 ng/mL eg, Xanax --Alpha-hydroxyalprazolam Not Detected 20 ng/mL alprazolam metabolite Clonazepam Not Detected 20 ng/mL eg, Klonopin --7-aminoclonazepam Not Detected 40 ng/mL clonazepam metabolite Diazepam Not Detected 50 ng/mL eg, Valium Nordiazepam Not Detected 50 ng/mL metabolite of chlordiazepoxide (Librium), clorazepate (Tranxene), diazepam, halazepam (Alapryl), prazepam (Centrax) and others Oxazepam Not Detected 50 ng/mL eg, Serax; also metabolite of nordiazepam and temazepam Temazepam Not Detected 50 ng/mL eg, Restoril; also a metabolite of diazepam Lorazepam Not Detected 60 ng/mL eg, Ativan Midazolam Not Detected 20 ng/mL eg, Versed Zolpidem Present 20 ng/mL eg, Ambien Reference interval Creatinine value (mg/dL) 200.0 20.0 - 400.0 mg/dL Patient: PAIN HYB 2, 2009288 ARUP Accession: 21-048-107698 4848 Chart continues on following page(s) ARUP Enhanced Reporting | February 17, 2021 | page 4 of 5 Drug Profile, Targeted with Interpretation by Tandem Mass Spectrometry and Enzyme Immunoassay, Urine Patient: PAIN HYB 2, 2009288 | Date of Birth | Gender: M | Physician: DR T. -

The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines
The ICD-10 Classification of Mental and Behavioural Disorders: Clinical descriptions and diagnostic guidelines World Health Organization F10 - F19 Mental and behavioural disorders due to psychoactive substance use Overview of this block F10. – Mental and behavioural disorders due to use of alcohol F11. – Mental and behavioural disorders due to use of opioids F12. – Mental and behavioural disorders due to use of cannabinoids F13. – Mental and behavioural disorders due to use of sedative hypnotics F14. – Mental and behavioural disorders due to use of cocaine F15. – Mental and behavioural disorders due to use of other stimulants, including caffeine F16. – Mental and behavioural disorders due to use of hallucinogens F17. – Mental and behavioural disorders due to use of tobacco F18. – Mental and behavioural disorders due to use of volatile solvents F19. – Mental and behavioural disorders due to multiple drug use and use of other psychoactive substances Four- and five-character codes may be used to specify the clinical conditions, as follows: F1x.0 Acute intoxication .00 Uncomplicated .01 With trauma or other bodily injury .02 With other medical complications .03 With delirium .04 With perceptual distortions .05 With coma .06 With convulsions .07 Pathological intoxication F1x.1 Harmful use F1x.2 Dependence syndrome .20 Currently abstinent .21 Currently abstinent, but in a protected environment .22 Currently on a clinically supervised maintenance or replacement regime [controlled dependence] .23 Currently abstinent, but receiving treatment with