Current Topics in Behavioral Neurosciences
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Medical Management of Depression
The new england journal of medicine review article drug therapy The Medical Management of Depression J. John Mann, M.D. ecurrent episodes of major depression, which is a common From the Department of Neuroscience, and serious illness, are called major depressive disorder; depressive episodes New York State Psychiatric Institute– r Columbia University College of Physicians that occur in conjunction with manic episodes are called bipolar disorder. and Surgeons, New York. Address reprint Major depressive disorder accounts for 4.4 percent of the total overall global disease requests to Dr. Mann at the Department of burden, a contribution similar to that of ischemic heart disease or diarrheal diseases.1 Neuroscience, New York State Psychiatric 2 Institute, 1051 Riverside Dr., Box 42, New The prevalence of major depressive disorder in the United States is 5.4 to 8.9 percent York, NY 10032, or at [email protected]. and of bipolar disorder, 1.7 to 3.7 percent.3 Major depression affects 5 to 13 percent of medical outpatients,4 yet is often undiagnosed and untreated.5,6 Moreover, it is often N Engl J Med 2005;353:1819-34. undertreated when correctly diagnosed.6 Copyright © 2005 Massachusetts Medical Society. The demographics of depression are impressive. Among persons both with major depressive disorder and bipolar disorder, 75 to 85 percent have recurrent episodes.7,8 In addition, 10 to 30 percent of persons with a major depressive episode recover incom- pletely and have persistent, residual depressive symptoms, or dysthymia, a disorder with symptoms -

Polymorphic Regions of the Estrogen Receptor, Androgen Receptor and Serotonin Transporter Genes and Their Association with Mood Variability in Young Women
Lakehead University Knowledge Commons,http://knowledgecommons.lakeheadu.ca Electronic Theses and Dissertations Retrospective theses 2006 Polymorphic regions of the estrogen receptor, androgen receptor and serotonin transporter genes and their association with mood variability in young women Richards, Meghan A. http://knowledgecommons.lakeheadu.ca/handle/2453/3361 Downloaded from Lakehead University, KnowledgeCommons Polymorphic Regions 1 Ruimmg head: GENETIC POLYMORPHISMS AND MOOD Polymorphic Regions of the Estrogen Receptor, Androgen Receptor and Serotonin Transporter Genes and their Association with Mood Variability in Young Women Meghan A. Richards M.A. Thesis Lakehead University Supervisor: Dr. Kirsten Oinonen copyright © Meghan Richards, 2006 Reproduced with permission of the copyright owner. Further reproduction prohibited without permission. Library and Bibliothèque et 1^1 Archives Canada Archives Canada Published Heritage Direction du Branch Patrimoine de l'édition 395 Wellington Street 395, rue Wellington Ottawa ON K1A 0N4 Ottawa ON K1A 0N4 Canada Canada Your file Votre référence ISBN: 978-0-494-21539-5 Our file Notre référence ISBN: 978-0-494-21539-5 NOTICE: AVIS: The author has granted a non L'auteur a accordé une licence non exclusive exclusive license allowing Library permettant à la Bibliothèque et Archives and Archives Canada to reproduce,Canada de reproduire, publier, archiver, publish, archive, preserve, conserve,sauvegarder, conserver, transmettre au public communicate to the public by par télécommunication ou par l'Internet, prêter, telecommunication or on the Internet,distribuer et vendre des thèses partout dans loan, distribute and sell theses le monde, à des fins commerciales ou autres, worldwide, for commercial or non sur support microforme, papier, électronique commercial purposes, in microform,et/ou autres formats. -

(19) United States (12) Patent Application Publication (10) Pub
US 20130289061A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2013/0289061 A1 Bhide et al. (43) Pub. Date: Oct. 31, 2013 (54) METHODS AND COMPOSITIONS TO Publication Classi?cation PREVENT ADDICTION (51) Int. Cl. (71) Applicant: The General Hospital Corporation, A61K 31/485 (2006-01) Boston’ MA (Us) A61K 31/4458 (2006.01) (52) U.S. Cl. (72) Inventors: Pradeep G. Bhide; Peabody, MA (US); CPC """"" " A61K31/485 (201301); ‘4161223011? Jmm‘“ Zhu’ Ansm’ MA. (Us); USPC ......... .. 514/282; 514/317; 514/654; 514/618; Thomas J. Spencer; Carhsle; MA (US); 514/279 Joseph Biederman; Brookline; MA (Us) (57) ABSTRACT Disclosed herein is a method of reducing or preventing the development of aversion to a CNS stimulant in a subject (21) App1_ NO_; 13/924,815 comprising; administering a therapeutic amount of the neu rological stimulant and administering an antagonist of the kappa opioid receptor; to thereby reduce or prevent the devel - . opment of aversion to the CNS stimulant in the subject. Also (22) Flled' Jun‘ 24’ 2013 disclosed is a method of reducing or preventing the develop ment of addiction to a CNS stimulant in a subj ect; comprising; _ _ administering the CNS stimulant and administering a mu Related U‘s‘ Apphcatlon Data opioid receptor antagonist to thereby reduce or prevent the (63) Continuation of application NO 13/389,959, ?led on development of addiction to the CNS stimulant in the subject. Apt 27’ 2012’ ?led as application NO_ PCT/US2010/ Also disclosed are pharmaceutical compositions comprising 045486 on Aug' 13 2010' a central nervous system stimulant and an opioid receptor ’ antagonist. -

YTN Ci Y COOCH3 --Al-E- F 7.1% F 5 6
USOO5853696A United States Patent (19) 11 Patent Number: 5,853,696 Elmaleh et al. (45) Date of Patent: Dec. 29, 1998 54 SUBSTITUTED 2-CARBOXYALKYL-3 Carroll et al., “Synthesis, Ligand Binding, QSAR, and (FLUOROPHENYL)-8-(3-HALOPROPEN-2- CoMFA Study . , Journal of Medicinal Chemistry YL) NORTROPANES AND THEIR USE AS 34:2719-2725, 1991. IMAGING AGENTS FOR Madras et al., “N-Modified Fluorophenyltropane Analogs. NEURODEGENERATIVE DISORDERS ... ", Pharmcology, Biochemistry & Behavior 35:949–953, 1990. 75 Inventors: David R. Elmaleh; Bertha K. Madras, Milius et al., “Synthesis and Receptor Binding of N-Sub both of Newton; Peter Meltzer, stituted Tropane Derivatives . , Journal of Medicinal Lexington; Robert N. Hanson, Newton, Chemistry 34:1728-1731, 1991. all of Mass. Boja et al. “New, Potent Cocaine Analogs: Ligand Binding 73 Assignees: Organix, Inc., Woburn; The General and Transport Studies in Rat Striatum' European J. of Hospital Corporation, Boston; The Pharmacology, 184:329–332 (1990). President and Fellows of Harvard Brownell et al. *Use of C-11 College, Cambridge; Northeastern 2B-Carbomethoxy-3B-4-Fluorophenyl Tropane (C-11 University, Boston, all of Mass. CFT) in Studying Dopamine Fiber Loss in a Primate Model of Parkinsonism” J. Nuclear Med. Abs., 33:946 (1992). 21 Appl. No.: 605,332 Canfield et al. “Autoradiographic Localization of Cocaine Binding Sites by HICFT (I HIWIN 35,428) in the 22 Filed: Feb. 20, 1996 Monkey Brain” Synapse, 6:189-195 (1990). Carroll et al. “Probes for the Cocaine Receptor. Potentially Related U.S. Application Data Irreversible Ligands for the Dopamine Transporter” J. Med. 62 Division of Ser. No. 142.584, Oct. -

Human 5-HT Transporter Availability Predicts Amygdala Reactivityin Vivo
The Journal of Neuroscience, August 22, 2007 • 27(34):9233–9237 • 9233 Brief Communications Human 5-HT Transporter Availability Predicts Amygdala Reactivity In Vivo Rebecca A. Rhodes,1 Naga Venkatesha Murthy,1,3 M. Alex Dresner,2 Sudhakar Selvaraj,1,4 Nikolaos Stavrakakis,1 Syed Babar,5 Philip J. Cowen,4 and Paul M. Grasby1 1Psychiatry Group, 2Imaging Sciences Department, Medical Research Council (MRC) Clinical Sciences Centre, and 3Experimental Medicine, Psychiatry Clinical Pharmaceology Discovery Medicine, GlaxoSmithKline Clinical Imaging Centre, Imperial College London, London W12 0NN, United Kingdom, 4Department of Psychiatry, University of Oxford, Oxford OX3 7JX, United Kingdom, and 5Radiology Department, Hammersmith Hospital, London W12 0HS, United Kingdom The amygdala plays a central role in fear conditioning, emotional processing, and memory modulation. A postulated key component of the neurochemical regulation of amygdala function is the neurotransmitter 5-hydroxytryptamine (5-HT), and synaptic levels of 5-HT in the amygdala and elsewhere are critically regulated by the 5-HT transporter (5-HTT). The aim of this study was to directly examine the relationship between 5-HTT availability and amygdala activity using multimodal [positron emission tomography (PET) and functional magnetic resonance imaging (fMRI)] imaging measures in the same individuals. Healthy male volunteers who had previously undergone an[ 11C]-3-amino-4-(2-dimethylaminomethylphenylsulfanyl)-benzonitrile([ 11C]-DASB)PETscantodetermine5-HTTavailabilitycom- pleted an fMRI emotion recognition task. [ 11C]-DASB binding potential values were calculated for the amygdala using arterial input function and linear graphical (Logan) analysis. fMRI was performed on a 3T Philips Intera scanner, and data were analyzed using SPM2 (Wellcome Department Imaging Neuroscience, University College London). -

Contents I. Central Nervous System Diseases Ii
CONTENTS CONTRIBUTORS xi PREFACE xiii CORRIGENDUM xv I. CENTRAL NERVOUS SYSTEM DISEASES Section Editor: David Wustrow, Pfizer Global Research & Development, Ann Arbor, Michigan 1. Neuronal Nicotinic Acetylcholine Receptor Modulators: Recent Advances and Therapeutic Potential 3 Scott R. Breining, Anatoly A. Mazurov and Craig H. Miller, Targacept, Inc., 200 East First Street, Suite 300, Winston-Salem, NC 27101 2. Recent Advances in Selective Serotonergic Agents 17 Wayne E. Childers, Jr. and Albert J. Robichaud, Chemical & Screening Sciences, Wyeth Research, CN 8000, Princeton, NJ 08543 3. BACE Inhibitors for the Treatment of Alzheimer’s Disease 35 Ellen W. Baxter and Allen B. Reitz, Johnson & Johnson Pharmaceutical Research and Development LLC, Spring House, PA 19477-0776 4. Positron Emission Tomography Agents for Central Nervous System Drug Development Applications 49 N. Scott Masona and Chester A. Mathisa,b,c, aDepartments of Radiology, bPharmacology and cPharmaceutical Sciences, University of Pittsburgh, Pittsburgh, PA, 15213, USA II. CARDIOVASCULAR AND METABOLIC DISEASES Section Editor: Andrew Stamford, Schering-Plough Research Institute, 2015 Galloping Hill Road, Kenilworth, New Jersey 5. Emerging Topics in Atherosclerosis: HDL Raising Therapies 71 Peter J. Sinclair, Merck Research Laboratories, Rahway, NJ 07065, USA v vi Contents 6. Small Molecule Anticoagulant/Antithrombotic Agents 85 Robert M. Scarborough, Anjali Pandey and Xiaoming Zhang, Portola Pharmaceuticals, Inc., 270 East Grand Ave., Suite 22, South San Francisco, CA 94080, USA 7. CB1 Cannabinoid Receptor Antagonists 103 Francis Barth, Sanofi-aventis, 371 rue du Professeur Blayac 34184 Montpellier Cedex 04, France 8. Melanin-Concentrating Hormone as a Therapeutic Target 119 Mark D. McBriar and Timothy J. Kowalski, Schering-Plough Research Institute, 2015 Galloping Hill Road, Kenilworth, NJ 07033 9. -
Enhanced Reporting
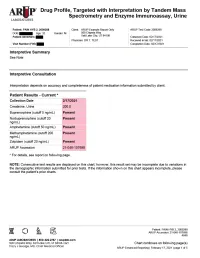
Drug Profile, Targeted with Interpretation by Tandem Mass Spectrometry and Enzyme Immunoassay, Urine Patient: PAIN HYB 2, 2009288 | Date of Birth: | Gender: M | Physician: DR T. TEST Patient Identifiers: | Visit Number (FIN): Drug Analyte Result Cutoff Notes Meperidine metabolite Not Detected 50 ng/mL normeperidine Tapentadol Not Detected 100 ng/mL --Tapentadol-o-sulfate Not Detected 200 ng/mL tapentadol metabolite AMPHETAMINE-LIKE, MASS SPEC Amphetamine Present 50 ng/mL eg, Vyvanse; also a metabolite of methamphetamine Methamphetamine Present 200 ng/mL d- and l- isomers are not distinguished by this test; may reflect Vicks inhaler, Desoxyn, Selegiline, or illicit source MDMA - Ecstasy Not Detected 200 ng/mL MDA Not Detected 200 ng/mL also a metabolite of MDMA and MDEA MDEA - Eve Not Detected 200 ng/mL Phentermine Not Detected 100 ng/mL Methylphenidate Not Detected 100 ng/mL eg, Ritalin, Dexmethylphenidate, Focalin, Concerta BENZODIAZEPINE-LIKE, MASS SPEC Alprazolam Not Detected 40 ng/mL eg, Xanax --Alpha-hydroxyalprazolam Not Detected 20 ng/mL alprazolam metabolite Clonazepam Not Detected 20 ng/mL eg, Klonopin --7-aminoclonazepam Not Detected 40 ng/mL clonazepam metabolite Diazepam Not Detected 50 ng/mL eg, Valium Nordiazepam Not Detected 50 ng/mL metabolite of chlordiazepoxide (Librium), clorazepate (Tranxene), diazepam, halazepam (Alapryl), prazepam (Centrax) and others Oxazepam Not Detected 50 ng/mL eg, Serax; also metabolite of nordiazepam and temazepam Temazepam Not Detected 50 ng/mL eg, Restoril; also a metabolite of diazepam Lorazepam Not Detected 60 ng/mL eg, Ativan Midazolam Not Detected 20 ng/mL eg, Versed Zolpidem Present 20 ng/mL eg, Ambien Reference interval Creatinine value (mg/dL) 200.0 20.0 - 400.0 mg/dL Patient: PAIN HYB 2, 2009288 ARUP Accession: 21-048-107698 4848 Chart continues on following page(s) ARUP Enhanced Reporting | February 17, 2021 | page 4 of 5 Drug Profile, Targeted with Interpretation by Tandem Mass Spectrometry and Enzyme Immunoassay, Urine Patient: PAIN HYB 2, 2009288 | Date of Birth | Gender: M | Physician: DR T. -

Pharmacological Characterizations of H05, a Novel Potent Serotonin And
JPET/2018/248351 Title: Pharmacological characterization of (3-(benzo[d][1,3] dioxol-4-yloxy) -3-(4-fluorophenyl)-N, N-dimethylpropan-1-amine (H05), a novel serotonin and noradrenaline reuptake inhibitor with moderate 5-HT2A antagonist activity for the treatment of depression Authors: Xiangqing Xu, Yaqin Wei, Qiang Guo, Song Zhao, Zhiqiang Liu, Ting Xiao, Yani Liu, Yinli Qiu, Yuanyuan Hou, Guisen Zhang and KeWei Wang Affiliations: Department of Molecular and Cellular Pharmacology, State Key Laboratory of Natural and Biomimetic Drugs, School of Pharmaceutical Sciences, Peking University , Beijing, China (X.X., T.X., K.W.W.); School of pharmacy, Xuzhou Medical University, Xuzhou, Jiangsu, China (Y.W.); Institute of pharmaceutical research, Jiangsu Nhwa Pharmaceutical Co., Ltd., Xuzhou, Jiangsu, China (Q.G., S.Z., Z.L., Y.Q., Y.H., G.Z.); Department of Pharmacology, School of Pharmacy, Qingdao University, Qingdao, Shandong, China (Y.L., K.W.W.) 1 Running title page Running title: A novel SNRI with 5-HT2A antagonist activity for treatment of depression Corresponding author: KeWei Wang Address: No. 38 Xueyuan Road, Haidian District, Beijing, 100191, China. Tel: 86•10•82805605; E•mail: [email protected] or [email protected] Number of text pages: 57 Number of tables: 3 Number of figures: 7 Number of references: 71 Words in Abstract: 248 Words in Introduction: 712 Words in Discussion:1357 Abbreviations: ADs: antidepressants; SSRIs: selective serotonin reuptake inhibitors; NRIs: norepinephrine reuptake inhibitors; SNRIs: serotonin and norepinephrine -

Amphetamine/Dextroamphetamine IR Generic
GEORGIA MEDICAID FEE-FOR-SERVICE STIMULANT AND RELATED AGENTS PA SUMMARY Preferred Non-Preferred Amphetamine/dextroamphetamine IR generic Adzenys ER (amphetamine ER oral suspension) Armodafinil generic Adzenys XR (amphetamine ER dispersible tab) Atomoxetine generic Amphetamine/dextroamphetamine ER (generic Concerta (methylphenidate ER/SA) Adderall XR) Dextroamphetamine IR tablets generic Aptensio XR (methylphenidate ER) Focalin (dexmethylphenidate) Clonidine ER generic Focalin XR (dexmethylphenidate ER) Cotempla XR (methylphenidate ER disintegrating Guanfacine ER generic tablet) Methylin oral solution (methylphenidate) Daytrana (methylphenidate TD patch) Methylphenidate CD/CR/ER generic by Lannett Desoxyn (methamphetamine) [NDCs 00527-####-##] and Kremers Urban [NDCs Dexmethylphenidate IR generic 62175-####-##] (generic Metadate CD) Dexmethylphenidate ER generic Methylphenidate IR generic Dextroamphetamine ER capsules generic Modafinil generic Dextroamphetamine oral solution generic Quillichew ER (methylphenidate ER chew tabs) Dyanavel XR (amphetamine ER oral suspension) Quillivant XR (methylphenidate ER oral suspension) Evekeo (amphetamine tablets) Vyvanse (lisdexamfetamine) Methamphetamine generic Zenzedi 5 mg, 10 mg IR tablets (dextroamphetamine) Methylphenidate IR chewable tablets generic Methylphenidate ER/SA (generic Concerta) Methylphenidate ER/LA/SR (generic Ritalin LA, Ritalin SR, Metadate ER) Methylphenidate ER/SA 72 mg generic Methylphenidate oral solution generic Mydayis (amphetamine/dextroamphetamine ER) Ritalin LA 10 mg -

Compositions and Methods for Selective Delivery of Oligonucleotide Molecules to Specific Neuron Types
(19) TZZ ¥Z_T (11) EP 2 380 595 A1 (12) EUROPEAN PATENT APPLICATION (43) Date of publication: (51) Int Cl.: 26.10.2011 Bulletin 2011/43 A61K 47/48 (2006.01) C12N 15/11 (2006.01) A61P 25/00 (2006.01) A61K 49/00 (2006.01) (2006.01) (21) Application number: 10382087.4 A61K 51/00 (22) Date of filing: 19.04.2010 (84) Designated Contracting States: • Alvarado Urbina, Gabriel AT BE BG CH CY CZ DE DK EE ES FI FR GB GR Nepean Ontario K2G 4Z1 (CA) HR HU IE IS IT LI LT LU LV MC MK MT NL NO PL • Bortolozzi Biassoni, Analia Alejandra PT RO SE SI SK SM TR E-08036, Barcelona (ES) Designated Extension States: • Artigas Perez, Francesc AL BA ME RS E-08036, Barcelona (ES) • Vila Bover, Miquel (71) Applicant: Nlife Therapeutics S.L. 15006 La Coruna (ES) E-08035, Barcelona (ES) (72) Inventors: (74) Representative: ABG Patentes, S.L. • Montefeltro, Andrés Pablo Avenida de Burgos 16D E-08014, Barcelon (ES) Edificio Euromor 28036 Madrid (ES) (54) Compositions and methods for selective delivery of oligonucleotide molecules to specific neuron types (57) The invention provides a conjugate comprising nucleuc acid toi cell of interests and thus, for the treat- (i) a nucleic acid which is complementary to a target nu- ment of diseases which require a down-regulation of the cleic acid sequence and which expression prevents or protein encoded by the target nucleic acid as well as for reduces expression of the target nucleic acid and (ii) a the delivery of contrast agents to the cells for diagnostic selectivity agent which is capable of binding with high purposes. -

Synthesis of Novel 6-Nitroquipazine Analogs for Imaging the Serotonin Transporter by Positron Emission Tomography
University of Montana ScholarWorks at University of Montana Graduate Student Theses, Dissertations, & Professional Papers Graduate School 2006 Synthesis of novel 6-nitroquipazine analogs for imaging the serotonin transporter by positron emission tomography David B. Bolstad The University of Montana Follow this and additional works at: https://scholarworks.umt.edu/etd Let us know how access to this document benefits ou.y Recommended Citation Bolstad, David B., "Synthesis of novel 6-nitroquipazine analogs for imaging the serotonin transporter by positron emission tomography" (2006). Graduate Student Theses, Dissertations, & Professional Papers. 9590. https://scholarworks.umt.edu/etd/9590 This Dissertation is brought to you for free and open access by the Graduate School at ScholarWorks at University of Montana. It has been accepted for inclusion in Graduate Student Theses, Dissertations, & Professional Papers by an authorized administrator of ScholarWorks at University of Montana. For more information, please contact [email protected]. Maureen and Mike MANSFIELD LIBRARY The University of Montana Permission is granted by the author to reproduce this material in its entirety, provided that this material is used for scholarly purposes and is properly cited in published works and reports. **Please check "Yes" or "No" and provide signature** Yes, I grant permission No, I do not grant permission Author's Signature: Date: C n { ( j o j 0 ^ Any copying for commercial purposes or financial gain may be undertaken only with the author's explicit consent. 8/98 Reproduced with permission of the copyright owner. Further reproduction prohibited without permission. Reproduced with permission of the copyright owner. Further reproduction prohibited without permission. -

A Brief Overview of Psychiatric Pharmacotherapy
A Brief Overview of Psychiatric Pharmacotherapy Joel V. Oberstar, M.D. Chief Executive Officer Disclosures • Some medications discussed are not approved by the FDA for use in the population discussed/described. • Some medications discussed are not approved by the FDA for use in the manner discussed/described. • Co-Owner: – PrairieCare and PrairieCare Medical Group – Catch LLC Disclaimer The contents of this handout are for informational purposes only and are not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified healthcare provider with any questions you may have regarding a medical or psychiatric condition. Never disregard professional/medical advice or delay in seeking it because of something you have read in this handout. Material in this handout may be copyrighted by the author or by third parties; reasonable efforts have been made to give attribution where appropriate. Caveat Regarding the Role of Medication… Neuroscience Overview Mind Over Matter, National Institute on Drug Abuse, National Institutes of Health. Available at: http://teens.drugabuse.gov/mom/index.asp. http://medicineworld.org/images/news-blogs/brain-700997.jpg Neuroscience Overview Mind Over Matter, National Institute on Drug Abuse, National Institutes of Health. Available at: http://teens.drugabuse.gov/mom/index.asp. Neurotransmitter Receptor Source: National Institute on Drug Abuse Common Diagnoses and Associated Medications • Psychotic Disorders – Antipsychotics • Bipolar Disorders – Mood Stabilizers, Antipsychotics, & Antidepressants • Depressive Disorders – Antidepressants • Anxiety Disorders – Antidepressants & Anxiolytics • Attention Deficit Hyperactivity Disorder – Stimulants, Antidepressants, 2-Adrenergic Agents, & Strattera Classes of Medications • Anti-depressants • Stimulants and non-stimulant alternatives • Anti-psychotics (a.k.a.