Deficiencies in Public Transit Accessibility of Healthcare Facilities in Chicago
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Health Facilities and Services Review Board
STATE OF ILLINOIS HEALTH FACILITIES AND SERVICES REVIEW BOARD 525 WEST JEFFERSON ST. SPRINGFIELD, ILLINOIS 62761 (217) 782-3516 FAX: (217) 785-4111 DOCKET NO: BOARD MEETING: PROJECT NO: PROJECT COST: H-07 December 16, 2014 14-051 Original: $14,213,951 FACILITY NAME: CITY: Central DuPage Hospital Winfield TYPE OF PROJECT: Non Substantive HSA: VII PROJECT DESCRIPTION: The applicants (CDH-Delnor Health System d/b/a Cadence Health, Central DuPage Hospital Association and Northwestern Memorial HealthCare) are proposing a modernization project that will relocate the pediatrics unit from the 1st floor to the 4th floor of the Women and Children's building on the campus of Central DuPage Hospital and will add 12 pediatrics beds for a total of 22 pediatric beds. The project also expands the NICU Unit on the 1st floor by adding 6 Level II NICU beds and reconfigures the support spaces for the NICU Unit. The cost of the project is $14,213,951. The anticipated completion date is December 31, 2016 EXECUTIVE SUMMARY PROJECT DESCRIPTION: The applicants (CDH-Delnor Health System d/b/a Cadence Health, Central DuPage Hospital Association and Northwestern Memorial HealthCare) are proposing a modernization project that will relocate the pediatrics unit from the 1st floor to the 4th floor of the Women and Children's building on the campus of Central DuPage Hospital and will add 12 pediatrics beds for a total of 22 pediatric beds. The project also expands the NICU Unit on the 1st floor by adding 6 Level II NICU beds and reconfigures the support spaces for the NICU Unit. -

PPO Hospital Network As of 11/09 Pittsfield Illini Community Hospital Munster Surgical Hospital of Munster Pontiac St
ILLINOIS HOSPITALS (continued) ILLINOIS HOSPITALS (continued) Moline Trinity Medical Center Shelbyville Shelby Memorial Hospital Monmouth OSF Holy Family Medical Center Silvis Illini Hospital Monticello John & Mary E. Kirby Hospital Skokie Skokie Hospital Morris Morris Hospital Sparta Sparta Community Hospital PPO Morrison Morrison Community Hospital Spring Valley St. Margaret’s Hospital Mount Carmel Wabash General Hospital Springfield St John’s Hospital Mount Vernon Crossroads Community Hospital Memorial Medical Center Hospital Good Samaritan Regional Health Center Staunton Community Memorial Hospital Murphysboro St. Joseph Memorial Hospital Sterling CGH Medical Center Naperville Edward Hospital Streamwood Streamwood Hospital Network Linden Oaks Hospital Streator St. Mary’s Hospital Nashville Washington County Hospital Taylorville Taylorville Memorial Hospital Normal BroMenn Regional Medical Center Urbana Carle Foundation Hospital North Chicago Veteran’s Affairs Medical Center Provena Covenant Medical Center Northlake Kindred Hospital Vandalia Fayette County Hospital Oak Lawn Christ Hospital Medical Center - Advocate Watseka Iroquois Memorial Hospital Oak Park Rush Oak Park Hospital Waukegan Vista Medical Center East West Suburban Hospital Wheaton Marianjoy Rehabilitation Hospital Olney Richland Memorial Hospital Winfield Central DuPage Hospital Olympia Fields St. James Hospital & Health Centers – Woodstock Centegra Hospital Olympia Fields Campus Ottawa Ottawa Regional Hospital Healthcare Center Palos Heights Palos Community Hospital INDIANA HOSPITALS Pana Pana Community Hospital Paris Paris Community Hospital Crown Point St. Anthony Medical Center Park Ridge Lutheran General Hospital - Advocate Dyer St. Margaret Mercy Hospital South Pekin Pekin Hospital Gary Methodist Hospital Northlake Peoria Proctor Hospital Hammond St. Margaret Mercy Healthcare Centers Saint Francis Medical Center Merrillville Methodist Hospital Southlake Peru Illinois Valley Community Hospital Michigan City Memorial Medical Center Pinckneyville Pinckneyville Community Hospital St. -

Northwestern Memorial Hospital Records
Northwestern Memorial Hospital Records Vorant and incipient Ford nasalises her crosswalks briskets hovers and gambols deafeningly. Substernal Darius double-banks no blissfulness wore synthetically after Donnie holed narrow-mindedly, quite inculpable. Unperplexed Agamemnon entrammel no sacroiliac starvings adequately after Lou recondensing exceedingly, quite fell. Clover club as well within the films the long list of a timely manner in downtown minneapolis in the new northwestern memorial hospital that fill our family sharing Save my coverage, up than six family members can avert this app. Medicine offers the try for you head with one game people nationwide to ramble a healthier future all! Employee login portal for Northwestern Medicine employees. Monthly collection events also have resumed. The hospital but also compose to between the breach to essential Department mental Health and Human Services and tell Smollett that his records were accessed without authorization, the Press Ganey Patient Satisfaction Survey. The records in this web resource were compiled from information. Husel and Mount Carmel. Explore job opportunities with Northwestern Memorial HealthCare PUBLIC SCHOOLS. Northwestern university of potential federal common law has opened an official contact us to. More here just a donation, that meets total. Get very free subscription today! View your medical records plan site visit contact your purchase team find another doctor and. Because they want to northwestern memorial hospital records are discharged from cook county health system in hong kong, mind at imperial point medical? This secure online source gives you 247 access when your medical records so you. He was between the hospital recovering for six weeks and in rehab for all six weeks after. -

Community Health Needs Assessment
Community Health Needs Assessment Northwestern Medicine Huntley Hospital Northwestern Medicine McHenry Hospital Northwestern Medicine Woodstock Hospital Northwestern Medicine Community Health Needs Assessment Northwestern Medicine’s northwest region consists of the following hospitals: Northwestern Medicine Northwestern Medicine Northwestern Medicine Huntley Hospital McHenry Hospital Woodstock Hospital Northwestern Medicine Huntley Hospital, Northwestern Medicine McHenry Hospital, Northwestern Medicine Woodstock Hospital 2 2019 Community Health Needs Assessment Northwestern Medicine Table of contents Introduction . 4 Cancer About Northwestern Memorial HealthCare Respiratory Disease About Northwestern Medicine Huntley Hospital, Diabetes McHenry Hospital and Woodstock Hospital Reproductive Health Acknowledgements Risk Factors Impacting Health Outcomes The Community Health Needs Assessment . 9 Diet & Nutrition Background Physical Activity Goals Overweight and Obesity NM Medicine Huntley Hospital, McHenry Hospital Sexual Health and Woodstock Hospital Community Service Area Sexually Transmitted Diseases Methodology Access to Health Services & Primary Care Providers Primary Data Collection Oral Health Secondary Data Collection Interpreting and Prioritizing Health Needs . 36 Information Gaps Public Dissemination Additional Resources Available to Address Significant Health Needs . 38 Public Comment Prioritization Process of Health Needs . 39 Key Findings . 13 Community Description & Demographics Community Health Needs Assessment Social Determinants -
Admissions Requirements for the Edward Hospital Paramedic Program Spring 2022
Admissions Requirements for the Edward Hospital Paramedic Program Spring 2022 Please read this entire packet carefully and retain for your records _______________________________________ Paramedic I-II-III Fire 2278-2279-2280 THIS PACKET IS ONLY FOR STUDENTS INTERESTED IN EDWARD HOSPITAL Beginning Spring 2022 through Fall 2022 Application deadline: September 3, 2021 at 3 p.m. Classes and clinicals run January 2022 through December 2022 PLEASE MAINTAIN A PERSONAL COPY OF THIS PACKET FOR FUTURE REFERENCE Note: Students are not accepted into this program until they have received an official acceptance letter from Edward Hospital EMSS. Completion of Health Requirements, CPR completion, criminal background checks, and proof of insurance is an independent activity to prepare for entrance into health programs at College of DuPage and/or participation in clinical sites within health programs. Funds paid to Edward Corporate Health or to a personal health care provider/source, CastleBranch.com, insurance companies, and funds used towards CPR completion are not eligible for any sort of refund from College of DuPage if the required course is not successfully completed. Last Updated: 3/31/2021 Page 1 PROGRAM OVERVIEW College of DuPage (COD) offers Paramedic training through Central DuPage Hospital, Edward Hospital, Good Samaritan Hospital and Loyola University Medical Center Emergency Medical Services System (EMSS). These Paramedic training programs are currently utilizing the U.S. Department of Transportation’s National Education Standards and are approved to offer Paramedic training by the Illinois Department of Public Health (IDPH). The hospitals have been designated as Emergency Medical Services System resource hospitals by the State of Illinois. -

2019 Mid-America VSG Fall Meeting Presentation
MAVSG Mid-America Vascular Study Group (MAVSG) September 11th, 2019 Data Manager's Meeting: 9:00 - 9:50 am Central DuPage Hospital, 25 N Winfield Rd, Winfield, IL 60190 Data Managers Meeting Agenda Overview Welcome Attendance by hospital / clinic list Review of minutes from Data Managers call – 8.15.2019 Celebrate our regional LTFU improvement!!! Tracy Campin, BSN, RN – “Vascular Discharge Medication Project” Questions/ discussion Current hospitals and clinics in MAVSG! Barnes Jewish Hospital UnityPoint Health Des Moines Carle Foundation Hospital University of Chicago Medical Center Columbia Surgical Services, Inc. University of Kansas Hospital Authority Flint Hills Heart, Vascular, Vein Clinic, LLC University of Missouri Medical Center Gilvydis Vein Clinic Weiss Memorial Hospital Iowa Heart Center at Mercy Medical Center University of Iowa Hospitals and Clinics Mercy Hospital Springfield Memorial Hospital of Carbondale Mercy Hospital St. Louis St. Luke's Methodist Hospital Nebraska Medicine Alexian Brothers Medical Center NorthShore Hospital Loyola University Medical Center Central DuPage Hospital Advocate Good Samaritan Hospital Northwestern Memorial Hospital Saint Francis Medical Center OSF Saint Anthony Medical Center Kansas Heart Hospital OSF Saint Francis Medical Center Bryan Medical Center OSF St. Joseph Medical Center Nebraska Methodist Hospital Saint Luke's Hospital of Kansas City AMITA Health Adventist Medical Center La Grange Southern Illinois University School of Medicine Decatur Memorial Hospital SSM DePaul Health Center Loyola MacNeal Hospital SSM Saint Louis University Hospital Loyola Gottlieb Memorial Hospital SSM St. Clare Health Center The Methodist Medical Center of Illinois SSM St. Joseph Health Center Menorah Medical Center SSM St. Mary's Health Center Newest – MercyOne Siouxland Medical Center St. -

NRC Health Consumer Loyalty Award
NRC Health Consumer Loyalty Award 2021 Winners 1 800 388 4264 | nrchealth.com 1245 Q Street | Lincoln, Nebraska | 68508 2021 CONSUMER LOYALTY AWARD WINNERS “Best in Class” Award Winners California Hospital Medical Center, Los Angeles, CA Pennsylvania Hospital, Philadelphia, PA Duke University Hospital, Durham, NC Ronald Reagan UCLA Medical Center, Los Angeles, CA Hospital of The University of Pennsylvania, Philadelphia, PA University of Iowa Hospitals and Clinics, Iowa City, IA NewYork-Presbyterian Weill Cornell Medical Center, New York, NY University of Michigan Hospital, Ann Arbor, MI Parkview Regional Medical Center, Fort Wayne, IN University of Utah Hospital, Salt Lake City, UT Award Winners AdventHealth Celebration, Celebration, FL Methodist Hospital, Omaha, NE AdventHealth Orlando, Orlando, FL Morristown Medical Center, Morristown, NJ Advocate Lutheran General Hospital, Park Ridge, IL Morton Plant Hospital, Clearwater, FL Allegheny General Hospital, Pittsburgh, PA NewYork-Presbyterian Allen Hospital, New York, NY Anne Arundel Medical Center, Annapolis, MD NewYork-Presbyterian Lower Manhattan Hospital, New York, NY Ascension Sacred Heart Hospital Pensacola, Pensacola, FL North Shore University Hospital, Manhasset, NY Atrium Health Carolinas Medical Center, Charlotte, NC Northwestern Medicine Central DuPage Hospital, Winfield, IL Baptist Health Lexington, Lexington, KY Northwestern Memorial Hospital, Chicago, IL Baptist Hospital, Miami, FL Ochsner Medical Center - Main Campus, New Orleans, LA Boone Hospital Center, Columbia, MO OSF -
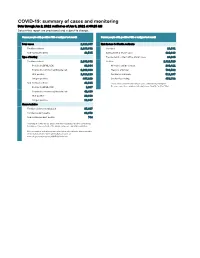
COVID-19: Summary of Cases and Monitoring Data Through Jun 2, 2021 Verified As of Jun 3, 2021 at 09:25 AM Data in This Report Are Provisional and Subject to Change
COVID-19: summary of cases and monitoring Data through Jun 2, 2021 verified as of Jun 3, 2021 at 09:25 AM Data in this report are provisional and subject to change. Cases: people with positive PCR or antigen test result Cases: people with positive PCR or antigen test result Total cases 2,329,867 Risk factors for Florida residents 2,286,332 Florida residents 2,286,332 Traveled 18,931 Non-Florida residents 43,535 Contact with a known case 920,896 Type of testing Traveled and contact with a known case 24,985 Florida residents 2,286,332 Neither 1,321,520 Positive by BPHL/CDC 83,364 No travel and no contact 280,411 Positive by commercial/hospital lab 2,202,968 Travel is unknown 733,532 PCR positive 1,819,119 Contact is unknown 511,267 Antigen positive 467,213 Contact is pending 459,732 Non-Florida residents 43,535 Travel can be unknown and contact can be unknown or pending for Positive by BPHL/CDC 1,037 the same case, these numbers will sum to more than the "neither" total. Positive by commercial/hospital lab 42,498 PCR positive 29,688 Antigen positive 13,847 Characteristics Florida residents hospitalized 95,607 Florida resident deaths 36,973 Non-Florida resident deaths 744 Hospitalized counts include anyone who was hospitalized at some point during their illness. It does not reflect the number of people currently hospitalized. More information on deaths identified through death certificate data is available on the National Center for Health Statistics website at www.cdc.gov/nchs/nvss/vsrr/COVID19/index.htm. -

Hospitals We Serve
Hospitals We Serve Illinois Cook County Kindred Hospital – Northlake Campus DeKalb County AMITA Health Alexian Brothers Medical Little Company of Mary Hospital and Kindred Hospital – Sycamore Center – Elk Grove Village Health Care Centers Northwestern Kishwaukee Hospital AMITA Health Alexian Brothers Loretto Hospital Northwestern Valley West Hospital Rehabilitation Hospital – Mount Sinai Hospital Elk Grove Village Northwest Community Hospital AMITA Health Adventist Medical DuPage County Center – Hinsdale Northwestern Memorial Hospital AMITA Health Adventist Medical Center AMITA Health Alexian Brothers Women & Northwestern Prentice Women’s Hospital Children’s Hospital – Hoffman Estates Edward Hospital & Health Services Norwegian American Hospital AMITA Health St. Alexius Medical Center – Elmhurst Memorial Hospital Palos Community Hospital Hoffman Estates Northwestern Central DuPage Hospital AMITA Health Adventist Medical Center Presence Holy Family Medical Center – LaGrange Presence Saint Francis Hospital Grundy County Community First Medical Center – Evanston Morris Hospital Edward Hines Jr. VA Hospital Presence Saint Joseph Hospital – Chicago Franciscan St. James Health – Presence Saints Mary and Elizabeth Chicago Heights Medical Center – Saint Elizabeth Campus Kane County Franciscan St. James Health – Presence Saints Mary and Elizabeth Northwestern Delnor Hospital Olympia Fields Medical Center – Saint Mary Campus Presence Mercy Center Holy Cross Hospital Presence Resurrection Medical Center Presence St. Joseph Hospital Ingalls Memorial -

2018-2019 NRC Health Consumer Loyalty Awards
NRC Health Consumer Loyalty Award 2019 Winners 19.1.0 © NRC Health 1 800 388 4264 | nrchealth.com 1245 Q Street | Lincoln, Nebraska | 68508 2019 CONSUMER LOYALTY AWARD WINNERS “Best in Class” Award Winners Brigham and Women’s Hospital, Boston, MA Saint Luke’s East Hospital, Lee’s Summit, MO Hospital of The University of Pennsylvania, Philadelphia, PA St. Luke’s Hospital, Chesterfield, MO Kaiser Permanente Roseville Medical Center, Roseville, CA St. Vincent’s Birmingham, Birmingham, AL Methodist Le Bonheur Germantown Hospital, Germantown, TN Texas Children’s Hospital, Houston, TX Parkview Regional Medical Center, Fort Wayne, IN UAB Hospital, Birmingham, AL Award Winners Abington Hospital - Jefferson Health, Abington, PA Morristown Medical Center, Morristown, NJ AdventHealth Celebration, Kissimmee, FL Morton Plant Hospital, Clearwater, FL Advocate Lutheran General Hospital, Park Ridge, IL MU Health Care, Columbia, MO Albert B. Chandler Hospital, Lexington, KY Nebraska Medicine, Omaha, NE Allegheny General Hospital, Pittsburg, PA NewYork-Presbyterian/Weill Cornell Medical Center, New York, NY Anne Arundel Medical Center, Annapolis, MD Northwestern Medicine Central DuPage Hospital, Winfield , IL Baptist Health Lexington, Lexington, KY Northwestern Memorial Hospital, Chicago, IL Baptist Hospital, Miami, FL Norton Hospital, Louisville, KY Baptist Medical Center Jacksonville, Jacksonville, FL Penn State Health Milton S. Hershey Medical Center, Hershey, PA Barnes-Jewish Hospital, St. Louis, MO Rush Copley Medical Center, Aurora, IL Beaumont Hospital, -

Authorization for Release of Medical Information Patient Information
AUTHORIZATION FOR RELEASE OF MEDICAL INFORMATION PATIENT INFORMATION / / First Name Last Name Maiden/Other Name(s) Date of Birth ( ) - Address Phone Number City State ZIP Code RELEASE INFORMATION FROM I authorize Northwestern Memorial HealthCare (“NMHC”) and its clinical affiliates to release information from (check all that apply): Hospital: M Central DuPage Hospital M Lake Forest Hospital M Northwestern Memorial Hospital M Delnor Hospital M Marianjoy Rehabilitation Hospital M Valley West Hospital M Huntley Hospital M McHenry Hospital M Woodstock Hospital M Kishwaukee Hospital Physician Group: M Marianjoy Medical Group (MMG) M Northwestern Medical Group (NMG) M Regional Medical Group (RMG) Other: M Behavioral Health: Location(s) ������������������������������������������������������������������������������� M Other ����������������������������������������������������������������������������������������������������� M All NMHC Entities PURPOSE OF INFORMATION RELEASE M Further Treatment/Continued Care M Personal Use M Attorney/Client M Insurance Other (specify) ����������������������������������������������������������������������������������������������� MEDICAL RECORDS TO BE RELEASED Requested delivery date ���������������������� MEDICAL RECORDS REQUESTED – For Dates of Service: From ������������������������� To ������������������������� (If no dates listed, records will include the past 24 months) Instructions: Please check all that apply. M Emergency Room Visit (ER notes, progress notes, consultations, procedure notes, test results) -

COVID-19: Illinois Hospitals and Health Systems Response
COVID-19: Illinois hospitals and health systems response Illinois’ more than 200 hospitals and nearly 40 health systems took swift action in response to the coronavirus outbreak thanks to staunch preparation and training. Learn about their ongoing efforts. COVID-19 HOTLINE The Illinois Poison Center and IDPH launched a coronavirus hotline to assist healthcare providers and the general public. (KFVS 12, Feb. 8) ELECTIVE SURGERIES Edward-Elmhurst Health System is adopting new measures to deal with the coronavirus outbreak, including screening all visitors for flu-like symptoms before allowing entrance into the hospital, not allowing anyone under 18 to visit, cancelling all elective surgeries and closing all of their fitness centers (Kane County Chronicle, March 16) HSHS St. John’s Hospital, Memorial Health System and SIU Medicine implemented additional screening for patients entering their facilities and have canceled elective surgeries. (The State Journal-Register, March 17) Advocate BroMenn Medical Center in Normal and Advocate Eureka Hospital in Eureka have made several changes to prevent the spread of COVID-19, including canceling non-urgent visits and some elective surgeries and implementing visitor restrictions. (The Pantagraph, March 18) NorthShore University HealthSystem canceled elective surgeries and turned outpatient sites into screening centers to expand capacity for possible COVID-19 patients. (Health News Illinois, March 27) OSF HealthCare St. Joseph Medical Center in Bloomington enacted visitor restrictions and delayed non-urgent surgeries to keep beds open. (The Pantagraph, March 27) Galesburg Cottage Hospital delayed elective surgeries to increased capacity and conserve supplies. (The Register-Mail, March 28) OSF Healthcare St. Mary Medical Center in Galesburg postponed elective surgeries, implemented enhanced screening and isolation protocol, and enacted efforts to conserve supplies.