SENEGAL Mid-Term Assessment Global Fund Breaking Down Barriers Initiative
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Mozambique Zambia South Africa Zimbabwe Tanzania
UNITED NATIONS MOZAMBIQUE Geospatial 30°E 35°E 40°E L a k UNITED REPUBLIC OF 10°S e 10°S Chinsali M a l a w TANZANIA Palma i Mocimboa da Praia R ovuma Mueda ^! Lua Mecula pu la ZAMBIA L a Quissanga k e NIASSA N Metangula y CABO DELGADO a Chiconono DEM. REP. OF s a Ancuabe Pemba THE CONGO Lichinga Montepuez Marrupa Chipata MALAWI Maúa Lilongwe Namuno Namapa a ^! gw n Mandimba Memba a io u Vila úr L L Mecubúri Nacala Kabwe Gamito Cuamba Vila Ribáué MecontaMonapo Mossuril Fingoè FurancungoCoutinho ^! Nampula 15°S Vila ^! 15°S Lago de NAMPULA TETE Junqueiro ^! Lusaka ZumboCahora Bassa Murrupula Mogincual K Nametil o afu ezi Namarrói Erego e b Mágoè Tete GiléL am i Z Moatize Milange g Angoche Lugela o Z n l a h m a bez e i ZAMBEZIA Vila n azoe Changara da Moma n M a Lake Chemba Morrumbala Maganja Bindura Guro h Kariba Pebane C Namacurra e Chinhoyi Harare Vila Quelimane u ^! Fontes iq Marondera Mopeia Marromeu b am Inhaminga Velha oz P M úngu Chinde Be ni n è SOFALA t of ManicaChimoio o o o o o o o o o o o o o o o gh ZIMBABWE o Bi Mutare Sussundenga Dondo Gweru Masvingo Beira I NDI A N Bulawayo Chibabava 20°S 20°S Espungabera Nova OCE A N Mambone Gwanda MANICA e Sav Inhassôro Vilanculos Chicualacuala Mabote Mapai INHAMBANE Lim Massinga p o p GAZA o Morrumbene Homoíne Massingir Panda ^! National capital SOUTH Inhambane Administrative capital Polokwane Guijá Inharrime Town, village o Chibuto Major airport Magude MaciaManjacazeQuissico International boundary AFRICA Administrative boundary MAPUTO Xai-Xai 25°S Nelspruit Main road 25°S Moamba Manhiça Railway Pretoria MatolaMaputo ^! ^! 0 100 200km Mbabane^!Namaacha Boane 0 50 100mi !\ Bela Johannesburg Lobamba Vista ESWATINI Map No. -

East and Central Africa 19
Most countries have based their long-term planning (‘vision’) documents on harnessing science, technology and innovation to development. Kevin Urama, Mammo Muchie and Remy Twingiyimana A schoolboy studies at home using a book illuminated by a single electric LED lightbulb in July 2015. Customers pay for the solar panel that powers their LED lighting through regular instalments to M-Kopa, a Nairobi-based provider of solar-lighting systems. Payment is made using a mobile-phone money-transfer service. Photo: © Waldo Swiegers/Bloomberg via Getty Images 498 East and Central Africa 19 . East and Central Africa Burundi, Cameroon, Central African Republic, Chad, Comoros, Congo (Republic of), Djibouti, Equatorial Guinea, Eritrea, Ethiopia, Gabon, Kenya, Rwanda, Somalia, South Sudan, Uganda Kevin Urama, Mammo Muchie and Remy Twiringiyimana Chapter 19 INTRODUCTION which invest in these technologies to take a growing share of the global oil market. This highlights the need for oil-producing Mixed economic fortunes African countries to invest in science and technology (S&T) to Most of the 16 East and Central African countries covered maintain their own competitiveness in the global market. in the present chapter are classified by the World Bank as being low-income economies. The exceptions are Half the region is ‘fragile and conflict-affected’ Cameroon, the Republic of Congo, Djibouti and the newest Other development challenges for the region include civil strife, member, South Sudan, which joined its three neighbours religious militancy and the persistence of killer diseases such in the lower middle-income category after being promoted as malaria and HIV, which sorely tax national health systems from low-income status in 2014. -

African Dialects
African Dialects • Adangme (Ghana ) • Afrikaans (Southern Africa ) • Akan: Asante (Ashanti) dialect (Ghana ) • Akan: Fante dialect (Ghana ) • Akan: Twi (Akwapem) dialect (Ghana ) • Amharic (Amarigna; Amarinya) (Ethiopia ) • Awing (Cameroon ) • Bakuba (Busoong, Kuba, Bushong) (Congo ) • Bambara (Mali; Senegal; Burkina ) • Bamoun (Cameroons ) • Bargu (Bariba) (Benin; Nigeria; Togo ) • Bassa (Gbasa) (Liberia ) • ici-Bemba (Wemba) (Congo; Zambia ) • Berba (Benin ) • Bihari: Mauritian Bhojpuri dialect - Latin Script (Mauritius ) • Bobo (Bwamou) (Burkina ) • Bulu (Boulou) (Cameroons ) • Chirpon-Lete-Anum (Cherepong; Guan) (Ghana ) • Ciokwe (Chokwe) (Angola; Congo ) • Creole, Indian Ocean: Mauritian dialect (Mauritius ) • Creole, Indian Ocean: Seychelles dialect (Kreol) (Seychelles ) • Dagbani (Dagbane; Dagomba) (Ghana; Togo ) • Diola (Jola) (Upper West Africa ) • Diola (Jola): Fogny (Jóola Fóoñi) dialect (The Gambia; Guinea; Senegal ) • Duala (Douala) (Cameroons ) • Dyula (Jula) (Burkina ) • Efik (Nigeria ) • Ekoi: Ejagham dialect (Cameroons; Nigeria ) • Ewe (Benin; Ghana; Togo ) • Ewe: Ge (Mina) dialect (Benin; Togo ) • Ewe: Watyi (Ouatchi, Waci) dialect (Benin; Togo ) • Ewondo (Cameroons ) • Fang (Equitorial Guinea ) • Fõ (Fon; Dahoméen) (Benin ) • Frafra (Ghana ) • Ful (Fula; Fulani; Fulfulde; Peul; Toucouleur) (West Africa ) • Ful: Torado dialect (Senegal ) • Gã: Accra dialect (Ghana; Togo ) • Gambai (Ngambai; Ngambaye) (Chad ) • olu-Ganda (Luganda) (Uganda ) • Gbaya (Baya) (Central African Republic; Cameroons; Congo ) • Gben (Ben) (Togo -
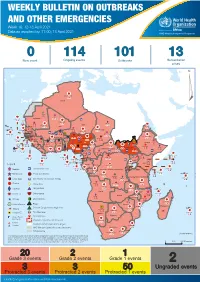
Week 16: 12-18 April 2021
WEEKLY BULLETIN ON OUTBREAKS AND OTHER EMERGENCIES Week 16: 12-18 April 2021 Data as reported by: 17:00; 18 April 2021 REGIONAL OFFICE FOR Africa WHO Health Emergencies Programme 0 114 101 13 New event Ongoing events Outbreaks Humanitarian crises 119 642 3 155 Algeria ¤ 36 13 110 0 5 694 170 Mauritania 7 2 13 070 433 110 0 7 0 Niger 17 129 453 Mali 3 491 10 567 0 6 0 2 079 4 4 706 169 Eritrea Cape Verde 39 782 1 091 Chad Senegal 5 074 189 61 0 Gambia 27 0 3 0 20 466 191 973 5 Guinea-Bissau 847 17 7 0 Burkina Faso 236 49 242 028 3 370 0 164 233 2 061 Guinea 13 129 154 12 38 397 1 3 712 66 1 1 23 12 Benin 30 0 Nigeria 1 873 72 0 Ethiopia 540 2 481 5 6 188 15 Sierra Leone Togo 3 473 296 61 731 919 52 14 Ghana 5 787 75 Côte d'Ivoire 10 473 114 14 484 479 63 0 40 0 Liberia 17 0 South Sudan Central African Republic 916 2 45 0 97 17 25 0 21 612 260 45 560 274 91 709 771 Cameroon 7 0 28 676 137 5 330 13 151 653 2 481 655 2 43 0 119 12 6 1 488 6 4 028 79 12 533 7 259 106 Equatorial Guinea Uganda 542 8 Sao Tome and Principe 32 11 2 066 85 41 378 338 Kenya Legend 7 611 95 Gabon Congo 2 012 73 Rwanda Humanitarian crisis 2 275 35 23 888 325 Measles 21 858 133 Democratic Republic of the Congo 10 084 137 Burundi 3 612 6 Monkeypox Ebola virus disease Seychelles 28 956 745 235 0 420 29 United Republic of Tanzania Lassa fever Skin disease of unknown etiology 190 0 4875 25 509 21 Cholera Yellow fever 1 349 5 6 257 229 24 389 561 cVDPV2 Dengue fever 90 918 1 235 Comoros Angola Malawi COVID-19 Chikungunya 33 941 1 138 862 0 3 815 146 Zambia 133 0 Mozambique -

Mozambique Country Profile
MOZAMBIQUE COUNTRY PROFILE Following a long civil war, Mozambique has transitioned to peace, stability, and economic growth. It now provides an essential link between landlocked neighbors and the global marketplace. Mozambique's ties to South Africa’s industrial heartland underscore the fact that the country’s economic, political, and social progress is vital to the interests of the region. Mozambique's recent economic downturn has exacerbated the high prevalence of HIV/AIDS, malaria and high infant mortality, and resulted in a distressingly low life expectancy of just 50 years. USAID’s programs in economic growth, health and education address these challenges and open new opportunities. OUR WORK AGRICULTURE AND FOOD SECURITY USAID / Agriculture continues to be the mainstay of the economy, but has declined to less than a quarter of GDP and accounts for more than 70% of employment of the economically active population. USAID is working to improve the overall performance of the agricultural sector, with the goal of increasing productivity, improving resilience, and generating higher incomes for farmers and their families to reduce hunger, poverty, and under-nutrition. ALEX LARRIEUX DEMOCRACY, HUMAN RIGHTS AND GOVERNANCE Good governance has emerged as one of Mozambique's greatest challenges. The lack of transparency and effective accountability is central to the ongoing fiscal crisis, and has contributed to the reemergence of armed conflict, most recently in the north of Cabo Delgado Province. USAID works to strengthen and promote democracy and good governance in Mozambique through activities that advance local media independence and sustainability, strengthen the rule of law, promote free and fair elections, and empower civil society. -
Mapping of Child Protection Accountability Mechanisms in Armed Conflict in Africa
1 LIST OF ACRONYMS Save the Children Somalia MAPPING OF CHILD PROTECTION ACCOUNTABILITY MECHANISMS IN ARMED CONFLICT IN AFRICA SAVE THE CHILDREN 1 MAPPING OF CHILD PROTECTION ACCOUNTABILITY MECHANISMS IN ARMED CONFLICT IN AFRICA ARMED CONFLICT IN MECHANISMS IN ACCOUNTABILITY MAPPING OF CHILD PROTECTION Save the Children Somalia 2 SAVE THE CHILDREN Save the Children is the world’s leading independent organisation for children. Save the Children works in more than 120 countries. We save children’s lives. We fight for their rights. We help them fulfil their potential. 1 LIST OF ACRONYMS Our vision A world in which every child attains the right to survival, protection, development and participation. Our mission To inspire breakthroughs in the way the world treats children and to achieve immediate and lasting change in their lives. We will stay true to our values of accountability, ambition, collaboration, creativity and integrity. Published by: Save the Children International East and Southern Africa Regional Office Regional Programming Unit Protecting Children in Conflict P.O. Box 19423-00202 Nairobi, Kenya Cellphone: +254 711 090 000 [email protected] www.savethechildren.net Save the Children East & Southern Africa Region SaveTheChildren E&SA @ESASavechildren https://www.youtube.com/channel/ UCYafJ7mw4EutPvYSkpnaruQ Project Lead: Anthony Njoroge Technical Lead: Fiona Otieno Reviewers: Simon Kadima, Joram Kibigo, Maryline Njoroge, Alexandra Chege, Mory Camara, Måns Welander, Anta Fall, Liliane Coulibaly, and Rita Kirema. © Save the Children International August 2019 Photos: Save the Children SAVE THE CHILDREN 3 Save the Children is the world’s leading independent organisation for children. Save the Children works in more than 120 countries. -

Country Codes ISO 3166
COUNTRY CODES - ISO 3166-1 ISO 3166-1 encoding list of the countries which are assigned official codes It is listed in alphabetical order by the country's English short name used by the ISO 3166/MA. Numeric English short name Alpha-2 code Alpha-3 code code Afghanistan AF AFG 4 Åland Islands AX ALA 248 Albania AL ALB 8 Algeria DZ DZA 12 American Samoa AS ASM 16 Andorra AD AND 20 Angola AO AGO 24 Anguilla AI AIA 660 Antarctica AQ ATA 10 Antigua and Barbuda AG ATG 28 Argentina AR ARG 32 Armenia AM ARM 51 Aruba AW ABW 533 Australia AU AUS 36 Austria AT AUT 40 Azerbaijan AZ AZE 31 Bahamas BS BHS 44 Bahrain BH BHR 48 Bangladesh BD BGD 50 Barbados BB BRB 52 Belarus BY BLR 112 Belgium BE BEL 56 Belize BZ BLZ 84 Benin BJ BEN 204 Bermuda BM BMU 60 Bhutan BT BTN 64 Bolivia (Plurinational State of) BO BOL 68 Bonaire, Sint Eustatius and Saba BQ BES 535 Bosnia and Herzegovina BA BIH 70 Botswana BW BWA 72 Bouvet Island BV BVT 74 Brazil BR BRA 76 British Indian Ocean Territory IO IOT 86 Brunei Darussalam BN BRN 96 Bulgaria BG BGR 100 Burkina Faso BF BFA 854 Burundi BI BDI 108 Cabo Verde CV CPV 132 Cambodia KH KHM 116 Cameroon CM CMR 120 Canada CA CAN 124 1500 Don Mills Road, Suite 800 Toronto, Ontario M3B 3K4 Telephone: 416 510 8039 Toll Free: 1 800 567 7084 www.gs1ca.org Numeric English short name Alpha-2 code Alpha-3 code code Cayman Islands KY CYM 136 Central African Republic CF CAF 140 Chad TD TCD 148 Chile CL CHL 152 China CN CHN 156 Christmas Island CX CXR 162 Cocos (Keeling) Islands CC CCK 166 Colombia CO COL 170 Comoros KM COM 174 Congo CG COG -
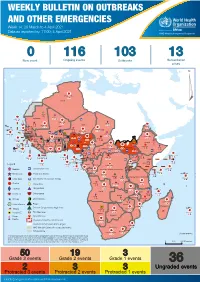
Weekly Bulletin on Outbreaks
WEEKLY BULLETIN ON OUTBREAKS AND OTHER EMERGENCIES Week 14: 29 March to 4 April 2021 Data as reported by: 17:00; 4 April 2021 REGIONAL OFFICE FOR Africa WHO Health Emergencies Programme 0 116 103 13 New event Ongoing events Outbreaks Humanitarian crises 117 622 3 105 Algeria ¤ 36 13 110 0 5 420 164 Mauritania 7 2 10 501 392 110 0 7 0 Niger 17 927 449 Mali 3 334 10 567 0 6 0 2 079 4 4 595 165 Eritrea Cape Verde 38 520 1 037 Chad Senegal 4 918 185 59 0 Gambia 27 0 3 0 17 125 159 9 761 45 Guinea-Bissau 796 17 7 0 Burkina Faso 225 46 215 189 2 963 0 162 593 2 048 Guinea 12 817 150 12 38 397 1 3 662 66 1 1 23 12 Benin 30 0 Nigeria 1 873 71 0 Ethiopia 420 14 481 5 6 188 15 Sierra Leone Togo 3 473 296 53 920 779 52 14 Ghana 5 245 72 Côte d'Ivoire 10 098 108 14 484 479 63 0 40 0 Liberia 17 0 South Sudan Central African Republic 916 2 45 0 25 0 19 670 120 43 180 237 90 287 740 Cameroon 7 0 28 676 137 5 330 13 138 988 2 224 1 952 87 655 2 51 22 43 0 112 12 6 1 488 6 3 988 79 11 187 6 902 102 Equatorial Guinea Uganda 542 8 Sao Tome and Principe 32 11 2 042 85 41 016 335 Kenya Legend 7 100 90 Gabon Congo 18 504 301 Rwanda Humanitarian crisis 2 212 34 22 482 311 Measles 18 777 111 Democratic Republic of the Congo 9 681 135 Burundi 2 964 6 Monkeypox Ebola virus disease Seychelles 27 930 739 1 525 0 420 29 United Republic of Tanzania Lassa fever Skin disease of unknown etiology 189 0 4 084 20 509 21 Cholera Yellow fever 1 349 5 6 257 229 22 631 542 cVDPV2 Dengue fever 88 930 1 220 Comoros Angola Malawi COVID-19 Chikungunya 33 661 1 123 862 0 3 719 146 -

Slavery and the Slave Trade in the Indian Ocean
2 Slavery and the Slave Trade in the Indian Ocean Vijayalakshmi Teelock and Abdul Sheriff The specificities of the Indian Ocean slave trade and slavery have been highlighted in the numerous works of historians of the Indian Ocean such as Ned Alpers, Abdul Sheriff, Richard Allen and Hubert Gerbeau, and are being recognised even by scholars of the Atlantic region. Within the Indian Ocean, however, the specificities of individual countries need to be highlighted and contrasted with each other. Some Indian Ocean countries, such as Zanzibar and Madagascar, were both importers and exporters of slaves, while others without indigenous populations, like Mauritius and Reunion, were solely importers of slave labour. Before embarking on a comparative study of the transition of these slave societies to freedom, it is necessary to have an understanding of the historical context of the establishment of slavery and the peopling of the islands through the slave trade. This is the focus of this chapter. Mauritius: The Colonial Slave Trade and Slavery According to latest figures available from Richard Allen and Thomas Vernet, the numbers of slaves exported from the Indian Ocean by Europeans far exceed previous estimates. Table 2.1: Export of slaves from the Indian Ocean 1670-1769 1770-1810 1811-1848 Total Madagascar 35,314-37,931 46,203-53,427 43,808-51,365 125,325-142,723 Eastern Africa 10,677-11,468 99,614-115,189 75,767-88,835 186,058-215,492 India 14,755-15,739 4,994-5,327 6,469-21,066 SE Asia 3,804-4,759 3,804-4,759 Of the total estimated by Allen1 to date, the French slave trade is still by far the most substantial in the Indian Ocean. -
Weekly Bulletin on Outbreaks
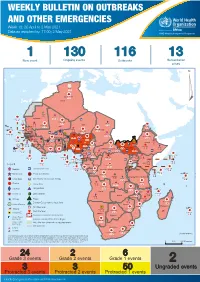
WEEKLY BULLETIN ON OUTBREAKS AND OTHER EMERGENCIES Week 18: 26 April to 2 May 2021 Data as reported by: 17:00; 2 May 2021 REGIONAL OFFICE FOR Africa WHO Health Emergencies Programme 1 130 116 13 New event Ongoing events Outbreaks Humanitarian crises 64 0 122 522 3 270 Algeria ¤ 36 13 612 0 5 901 175 Mauritania 7 2 13 915 489 110 0 7 0 Niger 18 448 455 Mali 3 671 10 567 0 6 0 2 079 4 4 828 170 Eritrea Cape Verde 40 433 1 110 Chad Senegal 5 074 189 61 0 Gambia 27 0 3 0 24 368 224 1 069 5 Guinea-Bissau 847 17 7 0 Burkina Faso 236 49 258 384 3 726 0 165 167 2 063 Guinea 13 319 157 12 3 736 67 1 1 23 12 Benin 30 0 Nigeria 1 873 72 0 Ethiopia 540 2 556 5 6 188 15 Sierra Leone Togo 3 473 296 52 14 Ghana 70 607 1 064 6 411 88 Côte d'Ivoire 10 583 115 14 484 479 65 0 40 0 Liberia 17 0 South Sudan Central African Republic 1 029 2 49 0 97 17 25 0 22 333 268 46 150 287 92 683 779 Cameroon 7 0 28 676 137 843 20 3 1 160 422 2 763 655 2 91 0 123 12 6 1 488 6 4 057 79 13 010 7 694 112 Equatorial Guinea Uganda 1 0 542 8 Sao Tome and Principe 32 11 2 066 85 41 973 342 Kenya Legend 7 821 99 Gabon Congo 2 012 73 Rwanda Humanitarian crisis 2 310 35 25 253 337 Measles 23 075 139 Democratic Republic of the Congo 11 016 147 Burundi 4 046 6 Monkeypox Ebola virus disease Seychelles 29 965 768 235 0 420 29 United Republic of Tanzania Lassa fever Skin disease of unknown etiology 191 0 5 941 26 509 21 Cholera Yellow fever 63 1 6 257 229 26 993 602 cVDPV2 Dengue fever 91 693 1 253 Comoros Angola Malawi COVID-19 Leishmaniasis 34 096 1 148 862 0 3 840 146 Zambia 133 -

Info Note OPCW Regional Meeting Gambia 2017-29.Pdf
Information Note1 Event: Fifteenth Regional Meeting of National Authorities of the Chemical Weapons Convention (CWC) States Parties in Africa Organizers: The Gambia and the Organisation for the Prohibition of Chemical Weapons (OPCW) Date and venue: 18-20 July 2017, Banjul, The Gambia Participants: Algeria, Angola, Benin, Burkina Faso, Burundi, Cameroon, Chad, Côte d’Ivoire, Democratic Republic of Congo, Ethiopia, The Gambia, Guinea Bissau, Kenya, Libya, Madagascar, Malawi, Mali, Mauritius, Mozambique, Morocco, Namibia, Nigeria, Rwanda, Sao Tome and Principe, Senegal, Sierra Leone, South Africa, Sudan, Tanzania, Togo, Tunisia, Uganda, Zambia and Zimbabwe. Background • Resolution 1540 (2004) calls on all States (operative paragraph 8) “to promote … full implementation and, where necessary, strengthening of multi-lateral treaties to which they are parties, whose main objective is to prevent the proliferation of nuclear biological or chemical weapons”. Further, the resolution calls upon States to renew and fulfil their commitment to multilateral cooperation, in particular within the framework of… and the Organisation for the Prohibition of Chemical Weapons… as an important means of achieving their common objectives in the area of non-proliferation…” • On 29 March 2017, a letter from the Director of the International Cooperation and Assistance Division, OPCW, sent to the Chair, invited a representative of the Group of Experts to participate in a panel discussion and make presentation on achievements, needs and challenges related to terrorism and non-state actors at the regional meetings being co-organised by OPCW with State Parties. The meeting was part of the events to commemorate the 20th anniversary of the entry-into-force of the Chemical Weapons Convention (CWC). -

Senegal Country Development Cooperation Strategy Original Dates: April 2, 2012 – April 2, 2017 Extended Through: April 2, 2019 Extended On: May 4, 2017
SENEGAL COUNTRY DEVELOPMENT COOPERATION STRATEGY ORIGINAL DATES: APRIL 2, 2012 – APRIL 2, 2017 EXTENDED THROUGH: APRIL 2, 2019 EXTENDED ON: MAY 4, 2017 May 2017 This publication was produced by the United States Agency for International Development. It was prepared by USAID/Senegal. SENEGAL COUNTRY DEVELOPMENT COOPERATION STRATEGY ORIGINAL DATES: APRIL 2, 2012 – APRIL 2, 2017 EXTENDED THROUGH: APRIL 2, 2019 EXTENDED ON: MAY 4, 2017 1 CONTENTS CONTENTS ................................................................................................................................................. 2 ACRONYMS ................................................................................................................................................ 3 1. DEVELOPMENT CONTEXT, CHALLENGES AND OPPORTUNITIES ....................................... 5 2. USAID/SENEGAL DEVELOPMENT OBJECTIVES ........................................................................ 10 3. MONITORING, EVALUATION AND LEARNING ........................................................................ 39 ANNEX A. M&E TABLE .......................................................................................................................... 43 2 ACRONYMS Abbreviations and acronyms have been kept to a minimum in the text of this document. Where abbreviations or acronyms have been used, they are accompanied by their full expression the first time they appear, unless they are commonly used and generally understood abbreviations such as NGO, kg., etc. However, in order to