Geographic Patterns of Hepatocellular Carcinoma Mortality with Exposure
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Assessment of Coastal Protection Based on Risk Maps
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 19 June 2018 doi:10.20944/preprints201806.0291.v1 Peer-reviewed version available at Water 2018, 10, 988; doi:10.3390/w10080988 1 Article 2 Assessment of Coastal Protection Based on Risk 3 Maps: A Case Study on Yunlin Coast, Taiwan 4 Wei-Po Huang 1,*, Jui-Chan Hsu 2 , Chun-Shen Chen 3 and Chun-Jhen Ye 4 5 1,* Department of Harbor and River Engineering, National Taiwan Ocean University, Keelung, Taiwan, 6 [email protected] 7 2 Department of Harbor and River Engineering, National Taiwan Ocean University, Keelung, Taiwan 8 [email protected] 9 3 Water Resources Planning Institute, Water Resources Agency, Ministry of Economic Affairs, Taiwan, 10 Taichung, Taiwan; [email protected] 11 4 Department of Harbor and River Engineering, National Taiwan Ocean University, Keelung, Taiwan, 12 [email protected] 13 * Correspondence: [email protected]; Tel.: +886-2-2462-2192 ext.6157 14 15 Abstract: In this study, we used the natural and anthropogenic characteristics of a coastal region to 16 generate risk maps showing vulnerability and potential hazards, and proposed design criteria for 17 coastal defense and land use for the various kinds of risks faced. The Yunlin coast: a first-level 18 protection area in mid-west Taiwan, was then used as an example to illustrate the proposed design 19 criteria. The safety of the present coastal defenses and land use of the Yunlin coastal area was 20 assessed, and coastal protection measures for hazard prevention were proposed based on the 21 generated risk map. -

Taipei Biennial 2020 2020.11.21–2021.3.14
YOU AND I DON’T LIVE ON THE SAME PLANET Taipei Biennial 2020 2020.11.21–2021.3.14 Curators: Bruno Latour & Martin Guinard with Eva Lin (public programs) Planet Globalization Planet Escape Gaia Planet Security Encounter-Zone Planet Encounter-Zone Terrestrial Critical Zone Alternative Alternative Gravity Contents Floor Plan p.6 Preface p.14 Introduction p.16 Prelude p.18 Planet Globalization p.22 Planet Security p.44 Planet Escape p.52 Planet Terrestrial p.56 Approaching the Terrestrial: Critical Zone p.58 Approaching the Terrestrial: Gaia p.84 New Diplomatic Encounters p.108 Public Programs p.110 Planet with Alternative Gravity p.118 Moving Earths p.130 Shoreline Movements p.136 Symposium p.144 Mobile App Guide | TFAM APP Taipei Biennial 2020 References p.146 www.taipeibiennial.org/2020 Acknowledgements p.149 F1 Hall Prelude p.20 1 Fernando PALMA RODRÍGUEZ 9 Second Floor 6 10 8 Planet Globalization 5 7 11 12 p.24 2 Mika ROTTENBERG 4 p.26 3 Jean KATAMBAYI MUKENDI 3 13 p.28 4 HUANG Hai-Hsin p.30 5 Franck LEIBOVICI & Julien SEROUSSI 2 p.32 6 Marianne MORILD 14 p.34 7 MILLIØNS (Zeina KOREITEM & John MAY) with Kiel MOE and 15 Peter OSBORNE p.36 8 Femke HERREGRAVEN p.38 9 Antonio VEGA MACOTELA 1 p.40 10 Hicham BERRADA p.42 11 CUI Jie Planet Security p.46 12 CHIN Cheng-Te, LEE Chia-Hung, LIN Chuan-Kai, and CHEN Yi-Chun p.48 13 Jonas STAAL p.50 14 James T. HONG Planet Escape p.54 15 Femke HERREGRAVEN First Floor Wang Da Hong 46 House Theater Planet Terrestrial Approaching the Terrestrial: Critical Zone South Entrance p.60 16a, b CHANG Yung-Ta 45 -

List of Insured Financial Institutions (PDF)
401 INSURED FINANCIAL INSTITUTIONS 2021/5/31 39 Insured Domestic Banks 5 Sanchong City Farmers' Association of New Taipei City 62 Hengshan District Farmers' Association of Hsinchu County 1 Bank of Taiwan 13 BNP Paribas 6 Banciao City Farmers' Association of New Taipei City 63 Sinfong Township Farmers' Association of Hsinchu County 2 Land Bank of Taiwan 14 Standard Chartered Bank 7 Danshuei Township Farmers' Association of New Taipei City 64 Miaoli City Farmers' Association of Miaoli County 3 Taiwan Cooperative Bank 15 Oversea-Chinese Banking Corporation 8 Shulin City Farmers' Association of New Taipei City 65 Jhunan Township Farmers' Association of Miaoli County 4 First Commercial Bank 16 Credit Agricole Corporate and Investment Bank 9 Yingge Township Farmers' Association of New Taipei City 66 Tongsiao Township Farmers' Association of Miaoli County 5 Hua Nan Commercial Bank 17 UBS AG 10 Sansia Township Farmers' Association of New Taipei City 67 Yuanli Township Farmers' Association of Miaoli County 6 Chang Hwa Commercial Bank 18 ING BANK, N. V. 11 Sinjhuang City Farmers' Association of New Taipei City 68 Houlong Township Farmers' Association of Miaoli County 7 Citibank Taiwan 19 Australia and New Zealand Bank 12 Sijhih City Farmers' Association of New Taipei City 69 Jhuolan Township Farmers' Association of Miaoli County 8 The Shanghai Commercial & Savings Bank 20 Wells Fargo Bank 13 Tucheng City Farmers' Association of New Taipei City 70 Sihu Township Farmers' Association of Miaoli County 9 Taipei Fubon Commercial Bank 21 MUFG Bank 14 -

Evaluation of Liquefaction Potential and Post-Liquefaction Settlement of Tzuoswei River Alluvial Plain in Western Taiwan
Missouri University of Science and Technology Scholars' Mine International Conference on Case Histories in (2008) - Sixth International Conference on Case Geotechnical Engineering Histories in Geotechnical Engineering 16 Aug 2008, 8:45am - 12:30pm Evaluation of Liquefaction Potential and Post-Liquefaction Settlement of Tzuoswei River Alluvial Plain in Western Taiwan C. P. Kuo National Taiwan University of Science & Technology, Taipei, Taiwan, China M. Chang National Yunlin University of Science & Technology, Yunlin, Taiwan, China R. E. Hsu National Yunlin University of Science & Technology, Yunlin, Taiwan, China S. H. Shau National Yunlin University of Science & Technology, Yunlin, Taiwan, China T. M. Lin National Yunlin University of Science & Technology, Yunlin, Taiwan, China Follow this and additional works at: https://scholarsmine.mst.edu/icchge Part of the Geotechnical Engineering Commons Recommended Citation Kuo, C. P.; Chang, M.; Hsu, R. E.; Shau, S. H.; and Lin, T. M., "Evaluation of Liquefaction Potential and Post- Liquefaction Settlement of Tzuoswei River Alluvial Plain in Western Taiwan" (2008). International Conference on Case Histories in Geotechnical Engineering. 8. https://scholarsmine.mst.edu/icchge/6icchge/session03/8 This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 4.0 License. This Article - Conference proceedings is brought to you for free and open access by Scholars' Mine. It has been accepted for inclusion in International Conference on Case Histories in Geotechnical Engineering by an authorized administrator of Scholars' Mine. This work is protected by U. S. Copyright Law. Unauthorized use including reproduction for redistribution requires the permission of the copyright holder. For more information, please contact [email protected]. -

Formosa Plastics Corporation Corporate Social Responsibility Report Contents
2015 Formosa Plastics Corporation Corporate Social Responsibility Report Contents 01 A Message from the Management Team 1. About the Report 3. Transparent and Honest Corporate Governance 05 1.1 Overview 37 3.1 Shareholders: A Trustworthy Corporation 05 1.2 Report Guidelines for Investors 06 1.3 Report Compilation Process 45 3.2 Customers: A Corporation that Grows with Its Customers 07 1.4 Stakeholder Identication and Communication 47 3.3 Suppliers and Contractors: Creating a Business Relationship based on Mutual 09 1.5 Identication of Critical Issues Trust and Interests 13 1.6 Risk Management 14 1.7 Corporate Social Responsibility Objectives 15 1.8 CSR Achievements at a Glance 2. Company Overview 23 2.1 Company Prole 4. A Happy and Healthy Work Environment 25 2.2 Management Philosophy 26 2.3 Main Products and Market Share 53 4.1 Protection of Human Rights and Recruitment 34 2.4 Participation in External Associations 56 4.2 Rights and Welfare of Employees 34 2.5 Economic Performance 62 4.3 Human Capital Cultivation 64 4.4 A Safe and Healthy Work Environment 5. Environment Sustainability 7. Social Welfare 71 5.1 Commitment to Environmental 119 7.1 Charitable Donations Protection 121 7.2Promotion of Medical Services and Education 74 5.2 Environmental Accounting 126 7.3 Social Assistance 75 5.3 Water and Energy Conservation and Greenhouse Gas Reduction 82 5.4 Energy Conservation in the Ofce 82 5.5 Environmental Protection at the Plant 90 5.6 Product Safety and Health Responsibility Appendix 135 1. Global Reporting Initiative 146 2. -
Non Binding Translation for Convenience Only
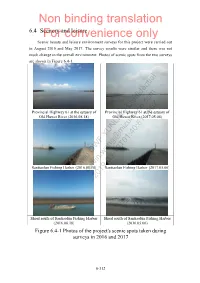
Non binding translation 6.4 SceneryFor and convenience leisure only Scenic beauty and leisure environment surveys for this project were carried out in August 2016 and May 2017. The survey results were similar and there was not much change in the overall environment. Photos of scenic spots from the two surveys are shown in Figure 6.4-1. Provincial Highway 61 at the estuary of Provincial Highway 61 at the estuary of Old Huwei River (2016.08.18) Old Huwei River (2017.05.06) Santiaolun Fishing Harbor (2016.08.18) Santiaolun Fishing Harbor (2017.05.06) Shoal south of Santiaolun Fishing Harbor Shoal south of Santiaolun Fishing Harbor (2016.08.18) (2016.05.06) Figure 6.4-1 Photos of the project's scenic spots taken during surveys in 2016 and 2017 6-312 Non binding translation For convenience only Observation platform on the western Observation platform on the western embankment of Gangxi Village embankment of Gangxi Village (2016.08.18) (2017.05.06) On the Aogu Wetland embankment On the Aogu Wetland embankment (2016.08.18) (2017.05.06) Dongshih Fisherman's Wharf (2016.08.18) Dongshih Fisherman's Wharf (2017.05.06) Figure 6.4-1 Photos of the project's scenic spots taken during surveys in 2016 and 2017 (continued) 6.4.1 Environmental scenic beauty I. Survey and analysis of the current development site scenic beauty status The wind farm is located off the coasts of Sihu Township and Kouhu Township, Yunlin County. Provincial Highways 17 and 61 (Western Coast Expressway) and County Roadways 155, 160, 164, and 166 are the main traffic access ways along the coast of Yunlin and Chiayi. -

Evaluation of the Preservation Value and Location of Farm Ponds in Yunlin County, Taiwan
Int. J. Environ. Res. Public Health 2014, 11, 548-572; doi:10.3390/ijerph110100548 OPEN ACCESS International Journal of Environmental Research and Public Health ISSN 1660-4601 www.mdpi.com/journal/ijerph Article Evaluation of the Preservation Value and Location of Farm Ponds in Yunlin County, Taiwan Wen-Wen Chou 1, Soen-Han Lee 1 and Chen-Fa Wu 2,* 1 Department of Architecture, National Cheng Kung University, Tainan City 701, Taiwan; E-Mails: [email protected] (W.-W.C.); [email protected] (S.-H.L.) 2 Department of Horticulture, National Chung Hsing University, Taichung City 402, Taiwan * Author to whom correspondence should be addressed; E-Mail: [email protected]; Tel./Fax: +886-422-859-125. Received: 7 October 2013; in revised form: 3 December 2013 / Accepted: 13 December 2013 / Published: 31 December 2013 Abstract: Farm ponds in Yunlin County first appeared in 1,622 and have played roles in habitation, production, the ecology, culture, and disaster reduction. Farm ponds largely disappeared with the development of urban areas and the industrial sector; thus, effective preservation of the remaining ponds is critical. The criteria to evaluate the preservation value of farm ponds is established by expert questionnaires which follow the Fuzzy Delphi Method (FDM) and Fuzzy Analytic Hierarchy Process (FAHP), and GIS, which are integrated into a spatial analysis of the remaining 481 farm ponds in Yunlin County. The results show that 28 ponds should be preserved to continue the cultural interaction between farm ponds and settlements; 36 ponds should preserved to connect coasts and streams, which are important habitats for birds; 30 ponds should be preserved to increase storage capacity, recharge groundwater, and reduce land subsidence; four ponds should be preserved as Feng-Shui ponds in front of temples in settlements or as recreation areas for local citizens; and four farms should be preserved (high priority) in agricultural production areas to support irrigation. -

Sustainability & Financial Report 2019
SUSTAINABILITY & FINANCIAL REPORT 2019 WELCOME FROM OUR CEO 2019 has been a year As Chief Executive Officer of Vena Energy Collaborations with our host and Chairperson of our Sustainability communities are stronger than ever, to remember for Committee, I am very pleased to welcome with new initiatives being carried out on Vena Energy, marking you to Vena Energy’s 2019 Sustainability healthcare, infrastructure, education, Report. and the environment across Australia, another consecutive Indonesia, India, Japan, Philippines, 2019 has been a year to remember Singapore, South Korea, Taiwan, and year of double-digit for Vena Energy, marking another Thailand. The cooperation and guidance growth in operating consecutive year of double-digit growth from our local stakeholders were essential in operating capacity, development for the success and effectiveness of our capacity, development project conversions, geographical corporate social responsibility initiatives. project conversions, expansion, functional integration, social For example, in 2019 we successfully initiatives, financial performance and completed our wildlife and natural habitat geographical expansion, talent onboarding in our ever more preservation project at our 70 MW Mingus functional integration, diversified regional team. I wish to Solar Farm in Taiwan. A large number of extend my gratitude to all our internal local and migratory wild birds have made social initiatives, and external stakeholders for their a permanent home within our 241,000m2 financial performance invaluable contributions, which enabled Ecological Conservation Area, including us to achieve such remarkable results. the endangered Black-Faced Spoonbill and talent onboarding in This success makes us even prouder as which migrates to our site during the our ever more diversified it comes from activities entirely aligned winter months. -

Taiwan Power Company Sustainability Report
Taiwan Power Company Sustainability Report 2014 Installed Capacity (40.79 GW) Purchased 9,386 MW 23% Corporate Pumped 2,602 MW 6% storage hydro IPP - Gas 4,610 MW 11% Highlights Oil 3,325 MW 8% IPP - Coal 3,097 MW 8% Coal 7,600 MW 19% Purchased Renewable 1,679 MW 4% Gas 10,635 MW 26% energy Nuclear 5,144 MW 13% Renewable 2,094 MW 5% energy Power Generation (219,224 GWh) Purchased 50,166 GWh 23% Pumped 3,108 GWh 1% storage hydro IPP - Gas 17,181 GWh 8% Oil 6,259 GWh 3% IPP - Coal 21,524 GWh 10% Coal 60,825 GWh 28% Purchased Renewable 4,457 GWh 2% Gas 53,734 GWh 24% energy Nuclear 40,801 GWh 19% Cogeneration 7,004 GWh 3% Renewable 4,331 GWh 2% energy Customers (13,389 thousand) Sales (205,956 GWh) Residential 11,975 89.4% Residential 42,506 20.6% Industrial 210 1.6% Industrial 113,939 55.3% Commercial 1,008 7.5% Commercial 32,064 15.6% Others 196 1.5% Others 17,447 8.5% 2009-2014 Power Outage Duration and Frequency 2009-2014 Line Loss 6% 19.246 19.050 4.86% 4.66% 4.76% 18.224 5% 17.663 18.086 4.42% 4.25% 17.496 4.09% 4% 0.298 0.264 0.264 2.65% 2.65% 0.238 3% 2.53% 2.37% 2.25% 2.12% 0.196 0.204 2% 2.21% 2.13% 2.11% 2.05% 2.00% 1.97% 1% 2009 2010 2011 2012 2013 2014 2009 2010 2011 2012 2013 2014 Duration of power outage per household (min/household x year) Total system Transmission Distribution Frequency of power outage per household (times/household x year) system system Total Assets (TWD million) Note Operating Revenue (TWD million) Note 2,000,000 1,893,952 1,926,503 800,000 592,732 642,747 523,722 547,698 1,800,000 600,000 511,171 1,608,656 1,629,499 1,628,947 400,000 1,600,000 200,000 1,400,000 0 2010 2011 2012 2013 2014 2010 2011 2012 2013 2014 Stockholders' Equity (TWD million) Note Gain/Loss before Income Tax (TWD million) Note 500,000 20,000 -18,106 -43,286 -61,606 -17,789 404,973 0 400,000 362,030 14,147 -20,000 300,000 283,106 180,481 194,609 -40,000 200,000 -60,000 100,000 -80,000 2010 2011 2012 2013 2014 2010 2011 2012 2013 2014 Note: Figures above have been audited by accountants using the ROC GAAP established in 2012 and the IFRS established in 2013. -

Non-Anopheline Mosquitoes of Taiwan: Annotated Catalog and Bibliography1
Pacific Insects 4 (3) : 615-649 October 10, 1962 NON-ANOPHELINE MOSQUITOES OF TAIWAN: ANNOTATED CATALOG AND BIBLIOGRAPHY1 By J. C. Lien TAIWAN PROVINCIAL MALARIA RESEARCH INSTITUTE2 INTRODUCTION The studies of the mosquitoes of Taiwan were initiated as early as 1901 or even earlier by several pioneer workers, i. e. K. Kinoshita, J. Hatori, F. V. Theobald, J. Tsuzuki and so on, and have subsequently been carried out by them and many other workers. Most of the workers laid much more emphasis on anopheline than on non-anopheline mosquitoes, because the former had direct bearing on the transmission of the most dreaded disease, malaria, in Taiwan. Owing to their efforts, the taxonomic problems of the Anopheles mos quitoes of Taiwan are now well settled, and their local distribution and some aspects of their habits well understood. However, there still remains much work to be done on the non-anopheline mosquitoes of Taiwan. Nowadays, malaria is being so successfully brought down to near-eradication in Taiwan that public health workers as well as the general pub lic are starting to give their attention to the control of other mosquito-borne diseases such as filariasis and Japanese B encephalitis, and the elimination of mosquito nuisance. Ac cordingly extensive studies of the non-anopheline mosquitoes of Taiwan now become very necessary and important. Morishita and Okada (1955) published a reference catalogue of the local non-anophe line mosquitoes. However the catalog compiled by them in 1955 was based on informa tion obtained before 1945. They listed 34 species, but now it becomes clear that 4 of them are respectively synonyms of 4 species among the remaining 30. -

Local Level Public Officials Election - Taiwan ,2018)
Election Result By Parties & Seats For Township Magistrates Councillors Elections (Local Level Public Officials Election - Taiwan ,2018) Parties & Seats Democratic Progressive Nonpartisan & Non-Party Locality Chungkuo Kuomintang Free Taiwan Party Pan Union Party(PEUP) Youth sunshine party Party nominated candidates Elected seats candidates Elected seats candidates Elected seats candidates Elected seats candidates Elected seats candidates Elected seats Total 135 80 95 40 1 0 1 0 1 0 290 78 Fujian 14 7 0 0 0 0 0 0 1 0 10 3 Province. Lienchiang 5 4 0 0 0 0 0 0 0 0 0 0 County Kinmen 9 3 0 0 0 0 0 0 1 0 10 3 County Taiwan 121 73 95 40 1 0 1 0 0 0 280 75 Province Yilan 11 8 10 3 0 0 0 0 0 0 11 1 County Hsinchu 14 10 1 0 0 0 0 0 0 0 22 3 County Miaoli 13 10 2 0 0 0 0 0 0 0 29 8 County Changhua 19 9 19 7 0 0 0 0 0 0 44 10 County Nantou 13 4 6 2 0 0 0 0 0 0 19 7 County Yunlin 6 1 17 9 0 0 0 0 0 0 31 10 County Chiayi 2 0 14 11 0 0 0 0 0 0 19 7 County Pingtung 10 8 18 7 1 0 1 0 0 0 59 18 County Taitung 13 9 4 1 0 0 0 0 0 0 26 6 County Hualien 17 12 2 0 0 0 0 0 0 0 13 1 County Penghu 3 2 2 0 0 0 0 0 0 0 7 4 County Source:Central Election Commission in The Republic of China (Taiwan) Election Date:2018-11-24 Edit: Election Study Center, National Chengchi University Election Result By Parties & Seats For Hsinchu County Councillors Elections (Local Level Public Officials Election - Taiwan ,2018) Parties & Seats Nonpartisan & Non-Party Locality Chungkuo Kuomintang Democratic Progressive Party nominated candidates Elected seats candidates Elected seats -

Pagina 1 Di 4 19/01/2015
Pagina 1 di 4 Print Highly pathogenic avian influenza, Chinese Taipei Close Information received on 16/01/2015 from Dr Ping-Cheng Yang, Vice President, Agriculture Technology Research Institute, Council of Agriculture, Hsinchu City, Chinese Taipei Summary Report type Follow-up report No. 3 Date of start of the event 07/01/2015 Date of pre-confirmation of the 11/01/2015 event Report date 16/01/2015 Date submitted to OIE 16/01/2015 Reason for notification Reoccurrence of a listed disease Date of previous occurrence 23/07/2014 Manifestation of disease Clinical disease Causal agent Highly pathogenic avian influenza virus Serotype H5N2 Nature of diagnosis Clinical, Laboratory (advanced) This event pertains to a defined zone within the country Immediate notification (12/01/2015) Follow-up report No. 1 (13/01/2015) Related reports Follow-up report No. 2 (15/01/2015) Follow-up report No. 3 (16/01/2015) New outbreaks (17) Outbreak 1 Kouhu Township, YUNLIN COUNTY Date of start of the outbreak 11/01/2015 Outbreak status Continuing (or date resolved not provided) Epidemiological unit Farm Species Susceptible Cases Deaths Destroyed Slaughtered Affected animals Birds 2200 897 897 1303 0 Affected population Breeding geese Outbreak 2 Budai Township, CHIAYI COUNTY Date of start of the outbreak 11/01/2015 Outbreak status Continuing (or date resolved not provided) Epidemiological unit Farm Species Susceptible Cases Deaths Destroyed Slaughtered Affected animals Birds 3600 1825 1825 1775 0 Affected population Geese Outbreak 3 Wandan Township, PINGTUNG COUNTY