Your Information. Your Rights. Our Responsibilities
Total Page:16
File Type:pdf, Size:1020Kb

Load more
Recommended publications
-

Urban Planning Approaches in Divided Cities
ITU A|Z • Vol 13 No 1 • March 2016 • 139-156 Urban planning approaches in divided cities Gizem CANER1, Fulin BÖLEN2 1 [email protected] • Department of Urban and Regional Planning, Graduate School of Science, Engineering and Technology, Istanbul Technical University, Istanbul, Turkey 2 [email protected] • Department of Urban and Regional Planning, Faculty of Architecture, Istanbul Technical University, Istanbul, Turkey Received: April 2014 • Final Acceptance: December 2015 Abstract This paper provides a comparative analysis of planning approaches in divided cities in order to investigate the role of planning in alleviating or exacerbating urban division in these societies. It analyses four urban areas—Berlin, Beirut, Belfast, Jerusalem—either of which has experienced or still experiences extreme divisions related to nationality, ethnicity, religion, and/or culture. Each case study is investigated in terms of planning approaches before division and after reunifi- cation (if applicable). The relation between division and planning is reciprocal: planning effects, and is effected by urban division. Therefore, it is generally assumed that traditional planning approaches are insufficient and that the recognized engagement meth- ods of planners in the planning process are ineffective to overcome the problems posed by divided cities. Theoretically, a variety of urban scholars have proposed different perspectives on this challenge. In analysing the role of planning in di- vided cities, both the role of planners, and planning interventions are evaluated within the light of related literature. The case studies indicate that even though different planning approaches have different consequences on the ground, there is a universal trend in harmony with the rest of the world in reshaping these cities. -

The Functions of a Capital City: Williamsburg and Its "Public Times," 1699-1765
W&M ScholarWorks Dissertations, Theses, and Masters Projects Theses, Dissertations, & Master Projects 1980 The functions of a capital city: Williamsburg and its "Public Times," 1699-1765 Mary S. Hoffschwelle College of William & Mary - Arts & Sciences Follow this and additional works at: https://scholarworks.wm.edu/etd Part of the United States History Commons Recommended Citation Hoffschwelle, Mary S., "The functions of a capital city: Williamsburg and its "Public Times," 1699-1765" (1980). Dissertations, Theses, and Masters Projects. Paper 1539625107. https://dx.doi.org/doi:10.21220/s2-ja0j-0893 This Thesis is brought to you for free and open access by the Theses, Dissertations, & Master Projects at W&M ScholarWorks. It has been accepted for inclusion in Dissertations, Theses, and Masters Projects by an authorized administrator of W&M ScholarWorks. For more information, please contact [email protected]. THE FUNCTIONS OF A CAPITAL CITY: »» WILLIAMSBURG AND ITS "PUBLICK T I M E S 1699-1765 A Thesis Presented to The Faculty of the Department of History The College of William and Mary in Virginia In Partial Fulfillment Of the Requirements for the Degree of Master of Arts by Mary S„ Hoffschwelle 1980 APPROVAL SHEET This thesis is submitted in partial fulfillment of the requirements for the degree of Master of Arts Mary S. Hoffschwelle Approved, August 1980 i / S A /] KdJL, C.£PC„ Kevin Kelly Q TABLE OF CONTENTS Page ABSTRACT ........................... ................... iv CHAPTER I. THEORETICAL BACKGROUND ........................... 2 CHAPTER II. THE URBAN IMPULSE IN COLONIAL VIRGINIA AND ITS IMPLEMENTATION ........................... 14 CHAPTER III. THE CAPITAL ACQUIRES A LIFE OF ITS OWN: PUBLIC TIMES ................... -
FC-Micronesia.Pdf
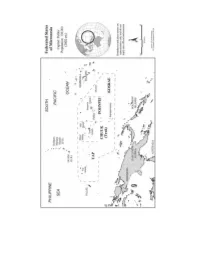
The Federated States of Micronesia DIRK ANTHONY BALLENDORF 1 history and development of federalism Micronesia is a collection of island groups in the Pacific Ocean comprised of four major clusters: the Marianas, Carolines, Marshalls, and Gilberts (now known as Kiribati). The Federated States of Micronesia (fsm) is part of the Caroline island archipelago. The fsm consists of the island groups of Chuuk (formerly Truk), Yap, Pohnpei (formerly Ponape) and Kosrae – it is thus a subset of Micronesia writ large. The total land area of the fsm is approximately 700 km, but the islands are spread over 2.5 million km. It has a population of approximately 108,000 people. The history of Micronesia is one of almost continuous exploitation since Ferdinand Magellan first landed briefly in Guam in 1521. Four successive colonial administrations – Spanish, 1521 to 1898; German, 1899 to 1914; Japanese, 1914 to 1944; and American, 1944 to indepen- dence in 1986 – have controlled the many small islands of Micronesia. In 1947, the United States was assigned administration of Microne- sia under a United Nations Trusteeship Agreement. Like previous co- lonial administrations, the American administration was centralized, with Saipan in the northern Marianas as the capital. The Micronesian peoples were divided into six separate administrative districts: Mari- anas, Yap, Palau, Truk (now Chuuk), Ponape (now Pohnpei), and the Marshalls, and they remained largely self-sufficient and isolated from the rest of the world. In 1977, a seventh district, Kosrae, was created from a division of the Ponape district. 217 Federated States of Micronesia Minimal attention was paid by both the United States and the United Nations to US obligations under the un Charter until a un mission to the area during the Kennedy administration drew attention to an extensive list of local complaints. -
Geographical Characteristics of the State
Geographical Characteristics of the State The Cultural Mosaic Fellman, and Notes from D.J. Zeigler of Old Dominion Vocab Review • State • Sovereignty • Nation • Nation-state • Binational or Multinational • Stateless Nation • Nationalism Territoriality • The modern state is an example of a common human tendency: the need to belong to a larger group that controls its own piece of the earth, its own territory. • This is called territoriality: a cultural strategy that uses power to control area and communicate that control, subjugating inhabitants and acquiring resources. Shapes of States • Compact States – Efficient – Theoretically round – Capital in center – Shortest possible boundaries to defend – Improved communications – Ex. Burundi, Kenya, Rwanda, Uganda, Poland, Uraguay Shapes of States • Prorupted States – w./large projecting extension – Sometimes natural – Sometimes to gain a resource or advantage, such as to reach water, create a buffer zone – Ex. Thailand, Myanmar, Namibia, Mozambique, Cameroon, Congo Shapes of States • Elongated States – States that are long and narrow – Suffer from poor internal communication – Capital may be isolated – Ex. Chile, Norway, Vietnam, Italy, Gambia Shapes of States • Fragmented States – Several discontinuous pieces of territory – Technically, all states w/off shore islands – Two kinds: separated by water & separated by an intervening state – Exclave – – Ex. Indonesia, USA, Russia, Philippines Shapes of States • Perforated States – A country that completely surrounds another state – Enclave – the surrounded territory – Ex. Lesotho/South Africa, San Marino & Vatican City/Italy Enclaves and exclaves • An enclave is an area surrounded by a country but not ruled by it. – It can be self-governing or an exclave of another country. Example-- Lesotho – Can be problematic for the surrounding country. -
The Laws on the Ethnic Minority Autonomous Regions in China: Legal Norms and Practices Haiting Zhang
Loyola University Chicago International Law Review Volume 9 Article 3 Issue 2 Spring/Summer 2012 2012 The Laws on the Ethnic Minority Autonomous Regions in China: Legal Norms and Practices Haiting Zhang Follow this and additional works at: http://lawecommons.luc.edu/lucilr Part of the International Law Commons Recommended Citation Haiting Zhang The Laws on the Ethnic Minority Autonomous Regions in China: Legal Norms and Practices, 9 Loy. U. Chi. Int'l L. Rev. 249 (2012). Available at: http://lawecommons.luc.edu/lucilr/vol9/iss2/3 This Feature Article is brought to you for free and open access by LAW eCommons. It has been accepted for inclusion in Loyola University Chicago International Law Review by an authorized administrator of LAW eCommons. For more information, please contact [email protected]. THE LAWS ON THE ETHNIC MINORITY AUTONOMous REGIONS IN CHINA: LEGAL NoRMS AND PRACTICES Haiting Zhang t I. Introduction... ............................ 249 II. Regulated Autonomous Powers of the Ethnic Minority Autonomous Regions.................................. 251 A. Autonomous Legislation Powers ....................... 252 B. Special Personnel Arrangements ....................... 252 C. Other Autonomous Powers .......................... 253 III. Problems in the Operation of the Regional Ethnic Autonomous System: The Gap Between Law and Practice ................. 254 A. Local Governmental Nature of the Autonomous Agencies ... 254 B. The Tale of Regional Autonomy Regulations: Insufficient Exercise of the Autonomous Legislation Power ............ 255 C. Behind the Personnel Arrangement: Party Politics and the Ethnic Minority Regional Autonomy ................... 257 D. The Vulnerable Autonomy............................ 259 E. The Economic Gap and the Natural Resource Exploitation Issue .......................................... 260 IV. Seeking Legal Guarantees: Improving the Exercise of the Autonomous Powers.......................................... -

CONDOMINIUM HOUSING in ETHIOPIA: the Integrated Housing Development Programme
SUMMARY Since 2005 Ethiopia has been implementing an ambitious government-led low- and middle- income housing programme: The Integrated Housing Development Programme (IHDP) which aims to construct 400,000 housing units, create 200,000 jobs, promote the development of 10,000 micro- and small- enterprises, and enhance the capacity of the construction sector. This authoritative book documents the genesis of the programme and the country’s experience since its inception. As it is intended for policy makers, public sector officials, and urban and housing practitioners, it logically outlines the design of this programme and its effect on the multiple dimensions of housing. Through documenting the Ethiopian experience other developing countries with housing shortages and who face rapid urbanization and population growth can adapt and apply this logic to their own housing systems. In light of Ethiopia’s previously uncoordinated and inefficient housing sector, the Integrated Housing Development Programme has proved to be a highly successful tool for affordable housing delivery at a large scale. Importantly, the programme is not only a housing programme but a wealth generation programme for low-income households. Its success lies in its integrated nature - understanding housing as part of an integrated social, economic, and political system - which has the opportunity to greatly improve the living conditions and economic capacity of all sectors of society. CONDOMINIUM HOUSING IN ETHIOPIA: The Integrated Housing Development Programme United Nations Human Settlements Programme (UN-HABITAT) P.O. Box 30030, Nairobi 00100, KENYA Tel: +254 20 762 3120 European Commission Website: www.unhabitat.org Series Summary: Housing Practices: country experiences of designing and implementing affordable housing programmes Housing Practices is an ongoing series that documents the experiences of countries who are implementing large-scale affordable housing programmes. -

52:9Q-12. Capital City Redevelopment Corporation A
52:9Q-12. Capital City Redevelopment Corporation a. There is established in the Executive Branch of the State Government a public body corporate and politic, with corporate succession, to be known as the Capital City Redevelopment Corporation. For the purpose of complying with the provisions of Article V, Section IV, paragraph 1 of the New Jersey Constitution, the corporation is allocated within the Department of the Treasury, but, notwithstanding that allocation the corporation shall be independent of any supervision or control by the department or by the State Treasurer or any officer or employee thereof. The corporation is constituted as an instrumentality of the State exercising public and essential governmental functions, and the exercise by the corporation of the powers conferred by this or any other act shall be deemed to be an essential governmental function of the State. b. The board of directors of the corporation shall consist of the following: a member of the Executive Branch to be appointed by the Governor, and the State Treasurer who shall both serve ex officio and may each designate, by written notification to the board, an alternate who shall act in their place with the authority to attend, vote and perform any duty or function assigned to them in their absence; one other high-ranking State officer designated by the Governor; the mayor of the city of Trenton, ex officio; and five public members appointed by the Governor with the advice and consent of the Senate, one of whom shall be a public employee of the State or city, one of whom shall have the city of Trenton as his principal place of business, and at least one of whom shall have the county of Mercer as his principal place of business. -

The Unique Case of Winnipeg
Prairie Perspectives 47 Provincial dominance: the unique case of Winnipeg William R. Horne, Brandon University Abstract: This paper identifies Winnipeg as a unique city within the Canadian urban system. While it is not among the largest cities in Canada, it dominates the province of Manitoba in a way that other capital cities and large cities do not. Statistical evidence for this domination is presented followed by historical reasons for its development. The economic and political effects on Manitoba are discussed. The city should not be discounted because of its decline in position at the national scale. Introduction When one thinks of the most powerful cities in Canada, Toronto, Montreal, Calgary and Vancouver quickly come to mind (McCann and Gunn 1998). At the provincial scale however, there is another city that appears to have more influence over its province than any other Canadian city. That city is Winnipeg. This paper will present evidence from the 2001 Census to support this claim. Four historical explanations for this situation will be argued. A review of provincial-municipal relationships across Canada will demonstrate the unique position of Winnipeg within Manitoba. The political structure of the province will further explain a number of actions taken by the provincial government to increase the economic and social importance of Winnipeg. Collectively, these factors give Winnipeg a unique position among Canadian cities. Much has been written about urban systems and the development of urban hierarchies. Stutz and Warf (2005) review two theories about the development of urban hierarchies. The central place model proposes that urban growth is related to the provision of services to a surrounding urban region. -

Administrative Divisions
INFORMATION PAPER Indonesia: Administrative Divisions Indonesia is the world's largest archipelagic state, stretching across both sides of the equator from the city of Banda Aceh at 05° 33' 28" N, 095° 19' 20" E in the west, to the city of Jayapura at 02° 31' 36" S, 140° 42' 51" E in the east. It is made up of over 17,500 islands (of which around 1,000 are permanently settled) strategically located along major sea lanes between the Pacific and Indian Oceans. The capital, Jakarta, is located near the northwestern coast of Jawa (Java). Its islands can be grouped into the Kepulauan Sunda Besar (Greater Sunda Islands) of Sumatera (Sumatra), Jawa, Sulawesi and the southern part of Kalimantan1; the Nusa Tenggara (Lesser Sunda) islands of Bali and a chain of islands that runs eastward through the island of Timor2; the Maluku (Moluccas) islands; and the western part of the island of New Guinea3. Indonesia Languages Indonesian (Bahasa Indonesia)4 is the official and most commonly spoken language in Indonesia, and is a modified version of Malay. It is the official language of the government and education. Over 700 local dialects of Indonesian are spoken, the most common of which is Javanese. English is also widely spoken in Indonesia. Administrative Divisions In May 1999, Indonesia embarked on a reform of regional governance5, decentralizing most functions of the government to the rural districts and municipalities and increasing local participation in politics and the economy. The Regional Autonomy Law6 gave authority to two levels of regional government, provinces (provinsi) at the first‐order administrative level (ADM1), and regencies (kabupaten) and 1 Kalimantan is the Indonesian name for the island of Borneo. -

Glossary Unit 4
01172017 Unit 04 Glossary APHUG The vocabulary list is structured according to the course outline found in the most recent AP® Human Geography Course Description published by the College Board. Term Definition the formal act of acquiring something (especially territory) by Annexation conquest or occupation an extremely cold continent at the south pole almost entirely Antarctica below the Antarctic Circle a social policy or racial segregation involving political and Apartheid economic and legal discrimination against non-whites series of anti-government protests, uprisings and armed Arab Spring rebellions that spread across the Middle East in early 2011 process by which a state breaks down through conflicts among Balkanization its ethnicities Vertical planes between states that cuts through rocks below, boundary and the airspace above the surface. Definitional- Disputes that arise from the legal language of the treaty definition of the boundary itself; one of the countries involved will usually sue another country in the International Court of Justice (World Court). Locational- Disputes that arise when the definition of the border is not questioned but the intention of the border is, as when the border has shifted (ex., a river shifts its course, changing the landscape). Operational- Disputes that arise from two abutting or adjacent countries disagreeing about a major functionality of the border, as when the United States and Mexico disagree over the issue Boundary, disputes of illegal immigration into the United States. (definitional, locational, Allocational- Disputes that usually involve conflicting claims to operational, allocational) the natural resources of a region and the drilling or mining of it. University of Texas at Austin UT High School 1 APHUG Unit 4 Vocabulary Antecedent- a boundary that existed before the cultural landscape emerged and stayed in place while people moved in to occupy the surrounding area. -

The Enduring Importance of National Capital Cities in the Global Era
URBAN AND REGIONAL University of RESEARCH Michigan COLLABORATIVE Working Paper www.caup.umich.edu/workingpapers Series URRC 03-08 The Enduring Importance of National Capital Cities in the Global Era 2003 Scott Campbell Urban and Regional Planning Program College of Architecture and Urban Planning University of Michigan 2000 Bonisteel Blvd. Ann Arbor, MI 48109-2069 [email protected] Abstract: This paper reports on the early results of a longer comparative project on capital cities. Specifically, it examines the changing role of national capital cities in this apparent global era. Globalization theory suggests that threats to the monopoly power of nation-states and the rise of a transnational network of global economic cities are challenging the traditional centrality of national capital cities. Indeed, both the changing status of nation-states and the restructuring world economy will reshuffle the current hierarchy of world cities, shift the balance of public and private power in capitals, and alter the current dominance of capitals as the commercial and governmental gateway between domestic and international spheres. However, claims in globalization theory that a new transnational system of global cities will make national boundaries, national governments and national capitals superfluous, albeit theoretically provocative, are arguably both ahistorical and improvident. Though one does see the spatial division of political and economic labor in some modern countries, especially in federations (e.g., Washington-New York; Ottawa-Toronto; Canberra-Sydney; Brasilia-Sao Paolo), the more common pattern is still the co- location of government and commerce (e.g., London, Paris, Tokyo, Seoul, Cairo). The emergence of global cities is intricately tied to the rise of nation-states -- and thus to the capital cities that govern them. -

Canada Map Assignment
Canada Map Assignment Due: _________________________________________ Name: _________________________________________ Instructions: 1. Obtain the required resources and read all the instructions before starting. 2. Colour your map after all labelling is completed. 3. Print in pencil only first, then go over the printing in black ink. 4. Work carefully and neatly. Resources Required: pencil, black pen, pencil crayons, ruler, eraser and an atlas. Part A Locate and label Canada’s three territories and ten provinces in CAPITAL letters and shade each as indicated. Alberta (yellow) British Columbia (orange) Manitoba (purple) Newfoundland and Labrador (purple) New Brunswick (red) Northwest Territories (red) Nova Scotia (pink) Nunavut (brown) Ontario (pink) Prince Edward Island (yellow) Quebec (orange) Saskatchewan (green) Yukon Territory (pink) Part B Locate and label the capital city of each province and territory and underline each city name. Part C Locate the capital city of Canada. Label this city in CAPITAL letters and underline. Part D Locate and label the following countries in CAPITAL letters and shade each as indicated. United States (grey) Greenland (green) Iceland (orange) Russia (brown) Part E Locate and label the following bodies of salt water and shade all ocean water dark blue: Pacific Ocean Arctic Ocean Atlantic Ocean Part F Locate and label the following bodies of fresh water on your map, and shade them light blue: Great Bear Lake Great Slave Lake Lake Winnipeg Lake Superior Lake Huron Lake Michigan Lake Erie Lake Ontario Part G Locate and label the following rivers and shade them light blue: Fraser River Mackenzie River St. Lawrence River Part H Complete your map with a frame, title and compass bearing.