RISPERDAL-Pi.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

From the Academy
FROM THE ACADEMY Joint American Academy of DermatologyeNational Psoriasis Foundation guidelines of care for the management and treatment of psoriasis with phototherapy Craig A. Elmets, MD (Co-Chair),a HenryW.Lim,MD,b Benjamin Stoff, MD, MA,c Cody Connor, MD,a Kelly M. Cordoro, MD,d Mark Lebwohl, MD,e AprilW.Armstrong,MD,MPH,f Dawn M. R. Davis, MD,g Boni E. Elewski, MD,a Joel M. Gelfand, MD, MSCE,h Kenneth B. Gordon, MD,i AliceB.Gottlieb,MD,PhD,j Daniel H. Kaplan, MD, PhD,k Arthur Kavanaugh, MD,l Matthew Kiselica, BA/BS,m Dario Kivelevitch, MD,n Neil J. Korman, MD, PhD,o Daniela Kroshinsky, MD, MPH,p Craig L. Leonardi, MD,q Jason Lichten, MD,m NehalN.Mehta,MD,MSCE,r Amy S. Paller, MD,s Sylvia L. Parra, MD,t Arun L. Pathy, MD,u Elizabeth A. Farley Prater, MD,v Reena N. Rupani, MD,e Michael Siegel, PhD,m BruceE.Strober,MD,PhD,w,x Emily B. Wong, MD,y Jashin J. Wu, MD,z Vidhya Hariharan, PhD,aa and Alan Menter, MD (Co-Chair)n Birmingham, Alabama; Detroit, Michigan; Atlanta, Georgia; San Francisco, Los Angeles, San Diego, and Irvine, California; New York, New York; Rochester, Minnesota; Philadelphia and Pittsburgh, Pennsylva- nia; Milwaukee, Wisconsin; Portland, Oregon; Dallas and San Antonio, Texas; Cleveland, Ohio; Boston, Massachusetts; St. Louis, Missouri; Bethesda, Maryland; Chicago and Rosemont, Illinois; Sumter, South Carolina; Centennial, Colorado; Oklahoma City, Oklahoma; Farmington, Connecticut; and Waterloo, Ontario, Canada Psoriasis is a chronic inflammatory disease involving multiple organ systems and affecting approximately 3.2% of the world’s population. -

Medication Conversion Chart
Fluphenazine FREQUENCY CONVERSION RATIO ROUTE USUAL DOSE (Range) (Range) OTHER INFORMATION KINETICS Prolixin® PO to IM Oral PO 2.5-20 mg/dy QD - QID NA ↑ dose by 2.5mg/dy Q week. After symptoms controlled, slowly ↓ dose to 1-5mg/dy (dosed QD) Onset: ≤ 1hr 1mg (2-60 mg/dy) Caution for doses > 20mg/dy (↑ risk EPS) Cmax: 0.5hr 2.5mg Elderly: Initial dose = 1 - 2.5mg/dy t½: 14.7-15.3hr 5mg Oral Soln: Dilute in 2oz water, tomato or fruit juice, milk, or uncaffeinated carbonated drinks Duration of Action: 6-8hr 10mg Avoid caffeinated drinks (coffee, cola), tannics (tea), or pectinates (apple juice) 2° possible incompatibilityElimination: Hepatic to inactive metabolites 5mg/ml soln Hemodialysis: Not dialyzable HCl IM 2.5-10 mg/dy Q6-8 hr 1/3-1/2 po dose = IM dose Initial dose (usual): 1.25mg Onset: ≤ 1hr Immediate Caution for doses > 10mg/dy Cmax: 1.5-2hr Release t½: 14.7-15.3hr 2.5mg/ml Duration Action: 6-8hr Elimination: Hepatic to inactive metabolites Hemodialysis: Not dialyzable Decanoate IM 12.5-50mg Q2-3 wks 10mg po = 12.5mg IM CONVERTING FROM PO TO LONG-ACTING DECANOATE: Onset: 24-72hr (4-72hr) Long-Acting SC (12.5-100mg) (1-4 wks) Round to nearest 12.5mg Method 1: 1.25 X po daily dose = equiv decanoate dose; admin Q2-3wks. Cont ½ po daily dose X 1st few mths Cmax: 48-96hr 25mg/ml Method 2: ↑ decanoate dose over 4wks & ↓ po dose over 4-8wks as follows (accelerate taper for sx of EPS): t½: 6.8-9.6dy (single dose) ORAL DECANOATE (Administer Q 2 weeks) 15dy (14-100dy chronic administration) ORAL DOSE (mg/dy) ↓ DOSE OVER (wks) INITIAL DOSE (mg) TARGET DOSE (mg) DOSE OVER (wks) Steady State: 2mth (1.5-3mth) 5 4 6.25 6.25 0 Duration Action: 2wk (1-6wk) Elimination: Hepatic to inactive metabolites 10 4 6.25 12.5 4 Hemodialysis: Not dialyzable 20 8 6.25 12.5 4 30 8 6.25 25 4 40 8 6.25 25 4 Method 3: Admin equivalent decanoate dose Q2-3wks. -

Adjunctive Risperidone Treatment for Antidepressant-Resistant
Supplementary Online Content Krystal JH, Rosenheck RA, Cramer JA, et al. Adjunctive risperidone treatment for antidepressant- resistant symptoms of chronic military service–related PTSD. JAMA. 2011;306(5):493-502. eTable 1. Follow-up Drugs Started After Randomization eTable 2. Baseline Medications eTable 3. Number of Different Drugs From Each Major Class Each Patient Is Taking at Baseline eTable 4. Baseline Medication Combinations eTable 5. Adverse Events eFigure 1. Product-Limit Survival Estimates With Number of Subjects at Risk eFigure 2. Percentage of Veterans at Each CAPS Severity Level at 24 Weeks, by Treatment This supplementary material has been provided by the authors to give readers additional information about their work. © 2011 American Medical Association. All rights reserved. Downloaded From: https://jamanetwork.com/ on 09/23/2021 eTable 1. Follow-up Drugs Started After Randomization Placebo Risperidone N= 134 N= 133 Total Patients % Patients % Patients % p-value Drugs started after randomization 46 34.3 59 44.4 105 39.3 0.10 Adrenergic Drugs 4 3.0 5 3.8 9 3.4 0.75 Atenolol 0 0.0 2 1.5 2 0.7 Metoprolol 3 2.2 2 1.5 5 1.9 Propranolol 1 0.7 1 0.8 2 0.7 Opiates 22 16.4 19 14.3 41 15.4 0.73 Codeine 1 0.7 1 0.8 2 0.7 Fentanyl 3 2.2 0 0.0 3 1.1 Hydrocodone (With Or Without 13 9.7 10 7.5 23 8.6 Acetaminophen) Methadone 1 0.7 0 0.0 1 0.4 Morphine 3 2.2 2 1.5 5 1.9 Oxycodone (With Or Without 4 3.0 7 5.3 11 4.1 Acetaminophen) Tramadol 3 2.2 2 1.5 5 1.9 Psycho-Stimulants 0 0.0 2 1.5 2 0.7 0.25 Methylphenidate 0 0.0 2 1.5 2 0.7 Muscle -

Psychedelics in Psychiatry: Neuroplastic, Immunomodulatory, and Neurotransmitter Mechanismss
Supplemental Material can be found at: /content/suppl/2020/12/18/73.1.202.DC1.html 1521-0081/73/1/202–277$35.00 https://doi.org/10.1124/pharmrev.120.000056 PHARMACOLOGICAL REVIEWS Pharmacol Rev 73:202–277, January 2021 Copyright © 2020 by The Author(s) This is an open access article distributed under the CC BY-NC Attribution 4.0 International license. ASSOCIATE EDITOR: MICHAEL NADER Psychedelics in Psychiatry: Neuroplastic, Immunomodulatory, and Neurotransmitter Mechanismss Antonio Inserra, Danilo De Gregorio, and Gabriella Gobbi Neurobiological Psychiatry Unit, Department of Psychiatry, McGill University, Montreal, Quebec, Canada Abstract ...................................................................................205 Significance Statement. ..................................................................205 I. Introduction . ..............................................................................205 A. Review Outline ........................................................................205 B. Psychiatric Disorders and the Need for Novel Pharmacotherapies .......................206 C. Psychedelic Compounds as Novel Therapeutics in Psychiatry: Overview and Comparison with Current Available Treatments . .....................................206 D. Classical or Serotonergic Psychedelics versus Nonclassical Psychedelics: Definition ......208 Downloaded from E. Dissociative Anesthetics................................................................209 F. Empathogens-Entactogens . ............................................................209 -

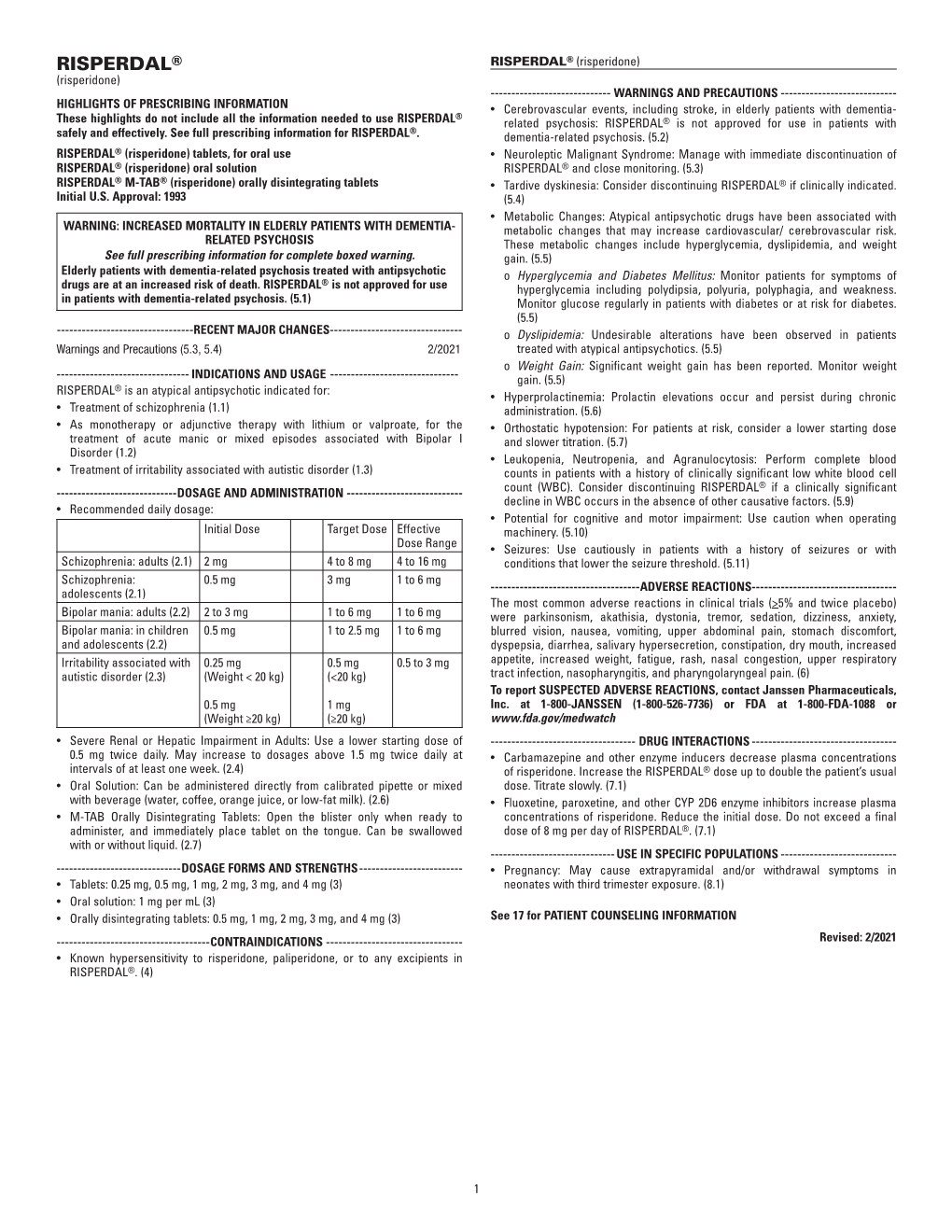
INVEGA SUSTENNA® (Paliperidone Palmitate)
INVEGA SUSTENNA® INVEGA SUSTENNA® (paliperidone palmitate) extended-release injectable suspension, for intramuscular use (paliperidone palmitate) extended-release injectable suspension, for intramuscular use --------------------------- DOSAGE FORMS AND STRENGTHS --------------------------- HIGHLIGHTS OF PRESCRIBING INFORMATION Extended-release injectable suspension: 39 mg/0.25 mL, 78 mg/0.5 mL, 117 mg/0.75 mL, These highlights do not include all the information needed to use 156 mg/mL, or 234 mg/1.5 mL (3) INVEGA SUSTENNA® safely and effectively. See full prescribing information for INVEGA SUSTENNA®. ----------------------------------- CONTRAINDICATIONS ----------------------------------- INVEGA SUSTENNA® (paliperidone palmitate) extended-release injectable Known hypersensitivity to paliperidone, risperidone, or to any excipients in suspension, for intramuscular use INVEGA SUSTENNA®. (4) Initial U.S. Approval: 2006 -----------------------------WARNINGS AND PRECAUTIONS ----------------------------- WARNING: INCREASED MORTALITY IN ELDERLY PATIENTS • Cerebrovascular Adverse Reactions, Including Stroke, in Elderly Patients with WITH DEMENTIA-RELATED PSYCHOSIS Dementia-Related Psychosis: Increased incidence of cerebrovascular adverse See full prescribing information for complete boxed warning. reactions (e.g. stroke, transient ischemic attack). (5.2) • Neuroleptic Malignant Syndrome: Manage with immediate discontinuation of Elderly patients with dementia-related psychosis treated with antipsychotic drug and close monitoring. (5.3) drugs are -

Treatment of Adult Major Depressive Disorder (MDD) Tool
Section: A B C D E F G Resources References Treatment of Adult Major Depressive Disorder (MDD) Tool This tool is designed to support primary care providers in the treatment of adult patients (≥ 18 years) who have major depressive disorder (MDD). MDD is the most prevalent depressive disorder, and approximately 7% of Canadians meet the diagnostic criteria every year.1,2 The treatment of MDD involves psychotherapy and/or pharmacotherapy. Providers should work with patients to create a treatment plan together using providers’ clinical expertise and keeping in mind the patient’s preferences, as well as the practicality, feasibility, availability and affordability of treatment. TABLE OF CONTENTS pg. 1 Section A: Overview of MDD pathway pg. 6 Section E: Complementary and alternative medicine pg. 2 Section B: Assessing suicidality and managing pg. 7 Section F: Follow-up and monitoring suicide-related behaviour pg. 9 Section G: Special patient populations pg. 3 Section C: Psychotherapy options pg. 10 Resources pg.3 Section D: Pharmacotherapy management SECTION A: Overview of MDD pathway Patient has suspected depression Talking Points It is important to provide your patient with non-judgmental care (e.g. “Being Consider unexpected life events (e.g. death in the family, diagnosed with depression is nothing to be ashamed of, it is very common and change in family status, financial crisis). Consider special many adults are diagnosed with it every year”) patient populations. • Don’t use clinical/psychiatric language (e.g. “mental health,” “psychiatric,” and/or “maladaptive”) unless the patient uses these terms first • Use understandable language for cognitive distortions (e.g. -

Annual Report
ANNUAL REPORT 2019 MARCH 2020 To Our Shareholders Alex Gorsky Chairman and Chief Executive Officer By just about every measure, Johnson & These are some of the many financial and Johnson’s 133rd year was extraordinary. strategic achievements that were made possible by the commitment of our more than • We delivered strong operational revenue and 132,000 Johnson & Johnson colleagues, who adjusted operational earnings growth* that passionately lead the way in improving the health exceeded the financial performance goals we and well-being of people around the world. set for the Company at the start of 2019. • We again made record investments in research and development (R&D)—more than $11 billion across our Pharmaceutical, Medical Devices Propelled by our people, products, and and Consumer businesses—as we maintained a purpose, we look forward to the future relentless pursuit of innovation to develop vital with great confidence and optimism scientific breakthroughs. as we remain committed to leading • We proudly launched new transformational across the spectrum of healthcare. medicines for untreated and treatment-resistant diseases, while gaining approvals for new uses of many of our medicines already in the market. Through proactive leadership across our enterprise, we navigated a constant surge • We deployed approximately $7 billion, of unique and complex challenges, spanning primarily in transactions that fortify our dynamic global issues, shifting political commitment to digital surgery for a more climates, industry and competitive headwinds, personalized and elevated standard of and an ongoing litigious environment. healthcare, and that enhance our position in consumer skin health. As we have experienced for 133 years, we • And our teams around the world continued can be sure that 2020 will present a new set of working to address pressing public health opportunities and challenges. -
JJPAF PAH Brochure
We help financially eligible patients receive prescription medications donated by Johnson & Johnson operating companies. Visit www.JJPAF.org to learn more or call 833-919-3510 (toll free) 308-920-4358 (direct dial) If you don’t have prescription coverage and can’t get access to Johnson & Johnson operating companies’ medications, we may be able to help. The Patient Assistance Program Our free prescription program is available to anyone who meets the requirements listed below: • You have been prescribed a Johnson & Johnson donated medication • You meet the eligibility income requirements for the product(s) • You don’t have any insurance or your medication is not covered – Some patients with Medicare Prescription Drug Coverage (Part D) who cannot afford their medications and who meet certain financial criteria may also be eligible for assistance • You live in the United States or a U.S. territory • You are being treated by a U.S. licensed doctor as an outpatient How the program works About the Foundation Visit us online • The Patient Assistance Program covers five The Johnson & Johnson Patient Assistance Foundation, We invite you to navigate and explore pulmonary arterial hypertension (PAH) Inc. (JJPAF) is an independent, non-profit organization www.JJPAF.org on your computer, tablet, prescription products as well as over that is committed to helping eligible patients without or smart phone. Website features include: 35 other prescription medications insurance coverage receive prescription products • User-friendly navigation donated by Johnson & Johnson operating companies. – The list of currently available PAH • Medication search functionality medications can be found at www.JJPAF.org Last year, we distributed over 580,000 units of • Step-by-step interactive process to check medication, helping more than 95,000 people receive • Once you meet program requirements and are patient eligibility approved, you’ll receive your medications for the medications they need. -

Optimal Duration of Risperidone Or Olanzapine Adjunctive Therapy to Mood Stabilizer Following Remission of a Manic Episode: a CANMAT Randomized Double-Blind Trial
Molecular Psychiatry (2016) 21, 1050–1056 OPEN © 2016 Macmillan Publishers Limited All rights reserved 1359-4184/16 www.nature.com/mp ORIGINAL ARTICLE Optimal duration of risperidone or olanzapine adjunctive therapy to mood stabilizer following remission of a manic episode: A CANMAT randomized double-blind trial LN Yatham1, S Beaulieu2, A Schaffer3, M Kauer-Sant’Anna4, F Kapczinski4, B Lafer5, V Sharma6, SV Parikh7, A Daigneault8, H Qian9, DJ Bond1, PH Silverstone10, N Walji1, R Milev11, P Baruch12, A da Cunha13, J Quevedo14, R Dias5, M Kunz4, LT Young15, RW Lam1 and H Wong16 Atypical antipsychotic adjunctive therapy to lithium or valproate is effective in treating acute mania. Although continuation of atypical antipsychotic adjunctive therapy after mania remission reduces relapse of mood episodes, the optimal duration is unknown. As many atypical antipsychotics cause weight gain and metabolic syndrome, they should not be continued unless the benefits outweigh the risks. This 52-week double-blind placebo-controlled trial recruited patients with bipolar I disorder (n = 159) who recently remitted from a manic episode during treatment with risperidone or olanzapine adjunctive therapy to lithium or valproate. Patients were randomized to one of three conditions: discontinuation of risperidone or olanzapine and substitution with placebo at (i) entry (‘0-weeks’ group) or (ii) at 24 weeks after entry (‘24-weeks’ group) or (iii) continuation of risperidone or olanzapine for the full duration of the study (‘52-weeks’ group). The primary outcome measure was time to relapse of any mood episode. Compared with the 0-weeks group, the time to any mood episode was significantly longer in the 24-weeks group (hazard ratio (HR) 0.53; 95% confidence interval (CI): 0.33, 0.86) and nearly so in the 52-weeks group (HR: 0.63; 95% CI: 0.39, 1.02). -

Christine Feorino)
Year-End Appeal 2015 YOUR SUPPORT HELPS PUT YOUTH ON THE RIGHT PATH Somerset Home’s mission is to aunt was not the best choice. provide abused, neglected, homeless, Fortunately however, he knew and runaway youth with housing, he could call Somerset Home for a stable environment, and help. Benji started in the Pathways supportive services to help program earlier this year. Pathways them become self-sufficient. counselors helped him get a steady Self-sufficiency is a key component job, learn how to budget, and find to ensure youth are prepared to live his own place. He is now working and thrive on their own well beyond two jobs – in retail and food service - Somerset Home. Through the and has saved more than $2,000. Pathways independent-living skills program, youth receive the tools and Until last year, Pathways worked knowledge needed for success. One mostly with clients who lived at of those youth is Benji... the Somerset Home residential programs. Since then, the program Benji was a resident at Passages. branched out to serve clients His father was incarcerated and his throughout central New Jersey. mother had substance abuse issues. The expansion has resulted in a As a result, he and his siblings would steady increase in referrals. This Pathways clients receive tools and knowledge to succeed in life. go weeks being neglected until they year, Pathways has served almost were ultimately put in foster care. 60 clients - a tremendous increase After living at Passages for several from previous years. employment, pertinent documents, driver’s licenses, and more. months, he decided to leave and live “I cannot thank Pathways enough for all your services”, said Benji. -
When and How to Use Long-Acting Injectable Antipsychotics
Savvy Psychopharmacology When and how to use long-acting injectable antipsychotics William Klugh Kennedy, PharmD, BCPP, FASHP ong-acting injectable antipsychotics Understanding the similarities and dif- (LAIs) are a pharmacotherapeutic op- ferences among LAIs7 and potential inter- L tion to help clinicians individualize patient variability of each LAI allows pre- schizophrenia treatment. LAIs have been scribers to tailor the dosing regimen to the available since the 1960s, starting with flu- patient more safely and efficiently (Table, phenazine and later haloperidol; however, page 42).1,8-11 All LAI antipsychotic formu- second-generation antipsychotics were not lations rely on absorption pharmacokinet- Vicki L. Ellingrod, available in the United States until 20071,2 ics (PK) rather than elimination PK, which PharmD, BCPP, FCCP and more are in development (Box).3,4 generally is true for sustained-release oral Series Editor Up to one-half of patients with schizo- formulations as well. Absorption half-life phrenia do not adhere to their medica- duration and absorption half-life variabil- tions.5 LAI use may mitigate relapse in ity are key concepts in LAI dosing. acute schizophrenia that is caused by poor adherence to oral medications. LAIs may Clinical pearls have a lower risk of dose-related adverse Before prescribing an LAI, check that your effects because of lower peak antipsychotic patient has no known contraindications plasma levels and less variation between to the active drug or delivery method. peak and trough plasma levels. LAIs may Peak-related adverse effects typically are decrease the financial burden of schizo- not contraindications, although they may phrenia and increase individual quality prompt you to start at a lower dose. -

2016 Annual Report
ANNUAL REPORT 2016 MARCH 2017 TO OUR SHAREHOLDERS ALEX GORSKY Chairman and Chief Executive Officer I’ve worked in the health care industry for Rather, true innovations are the result of WE ARE UNITED nearly 30 years. It’s been both an honor and collaboration. And that collaboration is AND INSPIRED a privilege to work for Johnson & Johnson, driven by a diversity of ideas, individuals BY OUR CREDO, a company that touches the lives of over and disciplines – working together toward WHICH RINGS a billion people every day, around the a common goal. AS TRUE TODAY world. As I look at today’s health care AS IT DID WHEN landscape, it’s incredibly clear that the Today, more than ever, the world needs IT WAS WRITTEN pace of change has never been greater, leaders who are committed to working MORE THAN 70 or frankly, more exciting. together to help bring improved health YEARS AGO. and wellness to every person in every Today’s rapid change brings both corner of the globe. As the world’s largest opportunities and risks for any company and most broadly based health care in health care, and we are prepared company, we are uniquely positioned to help to address both. There are significant transform global health care; to shine a light challenges to overcome, but the tools, the on the most important issues we are facing; insights, the technologies, the innovations to collaborate across boundaries and – both evolutions and revolutions – all borders; to uncover scientific insights and combine to make today one of the most ideas; and to dedicate resources towards promising times for human health and for creating tomorrow’s breakthroughs.