Loyola OB/GYN Clerkship Student Guide
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Caesarean Section Or Vaginal Delivery in the 21St Century
CAESAREAN SECTION OR VAGINAL DELIVERY IN THE 21ST CENTURY ntil the 20th Century, caesarean fluid embolism. The absolute risk of trans-placentally to the foetus, prepar- section (C/S) was a feared op- death with C/S in high and middle- ing the foetus to adopt its mother’s Ueration. The ubiquitous classical resource settings is between 1/2000 and microbiome. C/S interferes with neonatal uterine incision meant high maternal 1/4000 (2, 3). In subsequent pregnancies, exposure to maternal vaginal and skin mortality from bleeding and future the risk of placenta previa, placenta flora, leading to colonization with other uterine rupture. Even with aseptic surgi- accreta and uterine rupture is increased. environmental microbes and an altered cal technique, sepsis was common and These conditions increase maternal microbiome. Routine antibiotic exposure lethal without antibiotics. The operation mortality and severe maternal morbid- with C/S likely alters this further. was used almost solely to save the life of ity cumulatively with each subsequent Microbial exposure and the stress of a mother in whom vaginal delivery was C/S. This is of particular importance to labour also lead to marked activation extremely dangerous, such as one with women having large families. of immune system markers in the cord placenta previa. Foetal death and the use blood of neonates born vaginally or by of intrauterine foetal destructive proce- Maternal Benefits C/S after labour. These changes are absent dures, which carry their own morbidity, C/S has a modest protective effect against in the cord blood of neonates born by were often preferable to C/S. -

Postpartum Care of Taiwanese and Chinese Immigrant Women
City University of New York (CUNY) CUNY Academic Works All Dissertations, Theses, and Capstone Projects Dissertations, Theses, and Capstone Projects 2-2017 Retelling an Old Wife’s Tale: Postpartum Care of Taiwanese and Chinese Immigrant Women Kuan-Yi Chen The Graduate Center, City University of New York How does access to this work benefit ou?y Let us know! More information about this work at: https://academicworks.cuny.edu/gc_etds/1872 Discover additional works at: https://academicworks.cuny.edu This work is made publicly available by the City University of New York (CUNY). Contact: [email protected] RETELLING AN OLD WIFE’S TALE: POSTPARTUM CARE OF TAIWANESE AND CHINESE IMMIGRANT WOMEN by KUAN-YI CHEN A dissertation submitted to the Graduate Faculty in Sociology in partial fulfillment of the requirements for the degree of Doctor of Philosophy, The City University of New York 2017 © 2017 Kuan-Yi Chen All Rights Reserved ii Retelling an old wife’s tale: Postpartum care of Taiwanese and Chinese immigrant women by Kuan-Yi Chen This manuscript has been read and accepted for the Graduate Faculty in Sociology in satisfaction of the dissertation requirement for the degree of Doctor of Philosophy ______________________ _____________________________________ Date Barbara Katz Rothman Chair of Examining Committee ______________________ _____________________________________ Date Philip Kasinitz Executive Officer Supervisory Committee: Barbara Katz Rothman Margaret M. Chin Robert Courtney Smith THE CITY UNIVERSITY OF NEW YORK iii ABSTRACT Retelling an old wife’s tale: Postpartum care of Taiwanese and Chinese immigrant women by Kuan-Yi Chen Advisor: Barbara Katz Rothman The focus of this dissertation is the Chinese postpartum tradition zuoyuezi, often translated into English as doing-the-month. -

Management of Prolonged Decelerations ▲
OBG_1106_Dildy.finalREV 10/24/06 10:05 AM Page 30 OBGMANAGEMENT Gary A. Dildy III, MD OBSTETRIC EMERGENCIES Clinical Professor, Department of Obstetrics and Gynecology, Management of Louisiana State University Health Sciences Center New Orleans prolonged decelerations Director of Site Analysis HCA Perinatal Quality Assurance Some are benign, some are pathologic but reversible, Nashville, Tenn and others are the most feared complications in obstetrics Staff Perinatologist Maternal-Fetal Medicine St. Mark’s Hospital prolonged deceleration may signal ed prolonged decelerations is based on bed- Salt Lake City, Utah danger—or reflect a perfectly nor- side clinical judgment, which inevitably will A mal fetal response to maternal sometimes be imperfect given the unpre- pelvic examination.® BecauseDowden of the Healthwide dictability Media of these decelerations.” range of possibilities, this fetal heart rate pattern justifies close attention. For exam- “Fetal bradycardia” and “prolonged ple,Copyright repetitive Forprolonged personal decelerations use may onlydeceleration” are distinct entities indicate cord compression from oligohy- In general parlance, we often use the terms dramnios. Even more troubling, a pro- “fetal bradycardia” and “prolonged decel- longed deceleration may occur for the first eration” loosely. In practice, we must dif- IN THIS ARTICLE time during the evolution of a profound ferentiate these entities because underlying catastrophe, such as amniotic fluid pathophysiologic mechanisms and clinical 3 FHR patterns: embolism or uterine rupture during vagi- management may differ substantially. What would nal birth after cesarean delivery (VBAC). The problem: Since the introduction In some circumstances, a prolonged decel- of electronic fetal monitoring (EFM) in you do? eration may be the terminus of a progres- the 1960s, numerous descriptions of FHR ❙ Complete heart sion of nonreassuring fetal heart rate patterns have been published, each slight- block (FHR) changes, and becomes the immedi- ly different from the others. -

A Guide to Obstetrical Coding Production of This Document Is Made Possible by Financial Contributions from Health Canada and Provincial and Territorial Governments
ICD-10-CA | CCI A Guide to Obstetrical Coding Production of this document is made possible by financial contributions from Health Canada and provincial and territorial governments. The views expressed herein do not necessarily represent the views of Health Canada or any provincial or territorial government. Unless otherwise indicated, this product uses data provided by Canada’s provinces and territories. All rights reserved. The contents of this publication may be reproduced unaltered, in whole or in part and by any means, solely for non-commercial purposes, provided that the Canadian Institute for Health Information is properly and fully acknowledged as the copyright owner. Any reproduction or use of this publication or its contents for any commercial purpose requires the prior written authorization of the Canadian Institute for Health Information. Reproduction or use that suggests endorsement by, or affiliation with, the Canadian Institute for Health Information is prohibited. For permission or information, please contact CIHI: Canadian Institute for Health Information 495 Richmond Road, Suite 600 Ottawa, Ontario K2A 4H6 Phone: 613-241-7860 Fax: 613-241-8120 www.cihi.ca [email protected] © 2018 Canadian Institute for Health Information Cette publication est aussi disponible en français sous le titre Guide de codification des données en obstétrique. Table of contents About CIHI ................................................................................................................................. 6 Chapter 1: Introduction .............................................................................................................. -

A Close Look at the Contraction and Relaxation of the Myometrium; the Role of Calcium Myometriyumun Kasılma Ve Gevşeme Mekanizmalarında Kalsiyumun Rolü
230 This article will be credited by TMA within the scope of CME/CPD. Review A close look at the contraction and relaxation of the myometrium; the role of calcium Myometriyumun kasılma ve gevşeme mekanizmalarında kalsiyumun rolü Bilge Pehlivanoğlu, Sibel Bayrak, Murat Doğan Department of Physiology, Hacettepe University Faculty of Medicine, Ankara, Turkey Abstract Özet The function and regulation of the myometrium, especially during Üreme fizyolojisi açısından myometriyumun işlevleri ve bu işlevle- pregnancy, labour and birth are important in reproductive physiology. rin özellikle gebelik süreci ve doğum sırasında düzenlenmeleri çok It is crucial to understand the mechanisms that generate and modu- önemlidir. Uterus kasılmalarını başlatan ve etkileyen faktörlerin anla- late uterine contractility in order to be able to prevent and/or treat the şılabilmesi myometriyumu ilgilendiren patolojik durumların engellen- problems related with the myometrium. A limited understanding of mesi ve/veya tedavi edilebilmesi için çok önemlidir. Ancak bu fizyo- the cellular and molecular events underlying these phenomena com- lojik düzenlemeyi kontrol eden hücresel ve moleküler olayların tam plicates the situation. Various agonists, hormones, transmitters and/or olarak açıklanamamış olması nedeni ile tablo hala karmaşıktır. Çok chemicals are related to the regulation of the functions of the myome- sayıda agonistin, hormonların, transmiterlerin ve kimyasal maddele- trium. Although notable advances regarding the key steps in receptor rin myometriyum işlevlerinin düzenlenmesinde rolü olduğu gösteril- signalling explaining the actions of these factors have been achieved, miş ve bunların etki mekanizmalarındaki bazı anahtar basamaklar ile a good deal of information is still necessary to understand this vital ilgili gelişmeler kaydedilmiş olmasına karşın, bu yaşamsal işlevi daha process. -
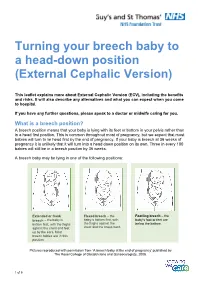
Turning Your Breech Baby to a Head-Down Position (External Cephalic Version)
Turning your breech baby to a head-down position (External Cephalic Version) This leaflet explains more about External Cephalic Version (ECV), including the benefits and risks. It will also describe any alternatives and what you can expect when you come to hospital. If you have any further questions, please speak to a doctor or midwife caring for you. What is a breech position? A breech position means that your baby is lying with its feet or bottom in your pelvis rather than in a head first position. This is common throughout most of pregnancy, but we expect that most babies will turn to lie head first by the end of pregnancy. If your baby is breech at 36 weeks of pregnancy it is unlikely that it will turn into a head down position on its own. Three in every 100 babies will still be in a breech position by 36 weeks. A breech baby may be lying in one of the following positions: Extended or frank Flexed breech – the Footling breech – the breech – the baby is baby is bottom first, with baby’s foot or feet are bottom first, with the thighs the thighs against the below the bottom. against the chest and feet chest and the knees bent. up by the ears. Most breech babies are in this position. Pictures reproduced with permission from ‘A breech baby at the end of pregnancy’ published by The Royal College of Obstetricians and Gynaecologists, 2008. 1 of 5 What causes breech? Breech is more common in women who are expecting twins, or in women who have a differently-shaped womb (uterus). -

Fetal Assement Methods
12/3/2020 Fetal Assement Methods 1 up to 9% of exam 5 to 9 questions 13.00 Adjunct Fetal Surveillance Methods 10%) 13.01 Auscultation (Intermittent Auscultation- IA) 13.02 Fetal movement counting 13.03 Nonstress testing 13.04 Fetal acid base interpretation – will be covered in a separate section 13.05 Biophysical profile 13.06 Fetal Acoustic Stimulation 2 1 12/3/2020 HERE IS ONE FOR YOU!! AWW… Skin to Skin in the OR ☺ 3 Auscultation 4 2 12/3/2020 Benefits of Auscultation • Based on Random Control Trials, neonatal outcomes are comparable to those monitored with EFM • Lower CS rates • Technique is non-invasive • Widespread application is possible • Freedom of movement • Lower cost • Hands on Time and one to one support are facilitated 5 Limitation of Auscultation • Use of the Fetoscope may limit the ability to hear FHR ( obesity, amniotic fluid, pt. movement and uterine contractions) • Certain FHR patterns cannot be detected – variability and some decelerations • Some women may think IA is intrusive • Documentation is not automatic • Potential to increase staff for 1:1 monitoring • Education, practice and skill assessment of staff 6 3 12/3/2020 Auscultation • Non-electronic devices such as a Fetoscope or Stethoscope • No longer common practice in the United States though may be increasing due to patient demand • Allows listening to sounds associated with the opening and closing of ventricular valves via bone conduction • Can hear actual heart sounds 7 Auscultation Fetoscope • A Fetoscope can detect: • FHR baseline • FHR Rhythm • Detect accelerations and decelerations from the baseline • Verify an FHR irregular rhythm • Can clarify double or half counting of EFM • AWHONN, (2015), pp. -

Leapfrog Hospital Survey Hard Copy
Leapfrog Hospital Survey Hard Copy QUESTIONS & REPORTING PERIODS ENDNOTES MEASURE SPECIFICATIONS FAQS Table of Contents Welcome to the 2016 Leapfrog Hospital Survey........................................................................................... 6 Important Notes about the 2016 Survey ............................................................................................ 6 Overview of the 2016 Leapfrog Hospital Survey ................................................................................ 7 Pre-Submission Checklist .................................................................................................................. 9 Instructions for Submitting a Leapfrog Hospital Survey ................................................................... 10 Helpful Tips for Verifying Submission ......................................................................................... 11 Tips for updating or correcting a previously submitted Leapfrog Hospital Survey ...................... 11 Deadlines ......................................................................................................................................... 13 Deadlines for the 2016 Leapfrog Hospital Survey ...................................................................... 13 Deadlines Related to the Hospital Safety Score ......................................................................... 13 Technical Assistance....................................................................................................................... -

Recommended Guidelines for Perinatal Care in Georgia
Section Two: Recommended Guidelines for Perinatal Care in Georgia Table of Contents Introduction to the Seventh Edition 3 Section I. Strategy for Action 4-8 Section II. Preconception and Interconception Health Care 9-10 Section III. Antepartum Care 11-15 Section IV. Intrapartum Care 16-24 Section V. Postpartum Care 25-27 Section VI. Perinatal Infections 28-30 Appendices Appendix A1. Perinatal Consultation and Transport Guidelines Georgia 31 Appendix A2. Suggested Parameters for Implementing Guidelines for Neonatal/ Maternal Transport 32-33 Appendix A3. Suggested Medical Criteria when determining the need for Consultation of Transport of the Maternal/Neonatal/Patient 34-35 Appendix A4. Perinatal Consultation/Transport Agreement 36 Appendix A5. Regional Perinatal Centers 37 Appendix B. Georgia Guidelines for Early Newborn Discharge, Minimal Criteria for Newborn Discharge, Late Preterm Discharge and Recommendation for Discharge Education Minimum Criteria for Newborn Discharge 38- 40 Appendix C. Capabilities of Health Care Providers in Hospital Delivery, Basic, Specialty and Specialty Care 41-42 Appendix D. Definitions Capabilities and Health Care Provider Types: Neonatal Levels of Care 43-44 Appendix F. Risk Identification 45 Appendix G. Maps of Georgia’s Counties Health Districts and Regions 46-50 Appendix H. Maternal and Child Health Sites 51-56 2 Introduction to the Seventh Edition This document, the Recommended Guidelines for Perinatal Care in Georgia, henceforth referred to as Guidelines, is the most comprehensive version to date. It is the culmination of work done by members and staff of the Regional Perinatal Centers and the Georgia Department of Public health (DPH), Division of Maternal & Child Health Section. This is the Third Edition under the title Recommended Guidelines for Perinatal Care in Georgia. -

Maternal Movement and Position Changes to Facilitate Labor Progress Have Been Discussed in the Literature for Decades
ELAINE ZWELLING, PHD, RN, LCCE, FACCE Abstract The benefi ts of maternal movement and position changes to facilitate labor progress have been discussed in the literature for decades. Recent routine interventions such as amniotomy, induction, fetal monitoring, and epidural anesthesia, as well as an increase in maternal obesity, have made position changes during labor challenging. The lack of maternal changes in position throughout labor can contribute to dystocia and increase the risk of cesarean births for failure to progress or descend. This article provides a historical review of the research fi ndings related to the effects of maternal positioning on the labor process and uses six physiological principles as a framework to offer sug- gestions for maternal positioning both before and after epidural anesthesia. Key Words Birth; Childbirth; Labor, fi rst stage; Labor, second stage; Maternity nursing; Obstetrical nursing; Maternal postures; Maternal positioning. Overcoming the Challenges: Maternal Movement 72 volume 35 | number 2 March/April 2010 or centuries laboring women chose to remain dural anesthesia, found that women who were able to mobile and upright, using positions such as change positions regularly or maintain upright positions standing, sitting, kneeling, hands and knees, or during labor were more comfortable and required less Fsquatting (Gupta & Nikodem, 2000; Johnson, pain medication (Atwood, 1976; de Jong et al., 1997; En- Johnson, & Gupta, 1991). Today immobility throughout gelmann, 1977; Johnson et al., 1991). For instance, Ada- the labor process has become a common occurrence for chi, Shimada, and Usul (2003) found in their study of 58 many childbearing women. Increased medical manage- laboring women that a sitting position decreased labor ment, obesity, lack of patient understanding about the pain in contrast with supine positioning. -

Automatic Contraction Detection Using Uterine Electromyography
applied sciences Article Automatic Contraction Detection Using Uterine Electromyography Filipa Esgalhado 1,2, Arnaldo G. Batista 1,3,* , Helena Mouriño 4, Sara Russo 1, Catarina R. Palma dos Reis 5,6,Fátima Serrano 5,6, Valentina Vassilenko 1,2 and Manuel Duarte Ortigueira 1,3 1 NOVA School of Science and Technology, NOVA University Lisbon, 2829-516 Caparica, Portugal; [email protected] (F.E.); [email protected] (S.R.); [email protected] (V.V.); [email protected] (M.D.O.) 2 NMT, S.A., Parque Tecnológico de Cantanhede, Núcleo 04, Lote 3, 3060-197 Cantanhede, Portugal 3 Center of Technology and Systems—UNINOVA, NOVA School of Science and Technology—NOVA University Lisbon, 2829-516 Caparica, Portugal 4 Faculdade de Ciências, Universidade de Lisboa, Campo Grande, 1749-016 Lisboa, Portugal; [email protected] 5 Maternidade Alfredo da Costa, Rua Viriato 1, 1050-170 Lisboa, Portugal; [email protected] (C.R.P.d.R.); [email protected] (F.S.) 6 Nova Medical School, Faculty of Medical Sciences, Universidade Nova de Lisboa, 1169-056 Lisboa, Portugal * Correspondence: [email protected]; Tel.: +351-21-2949637 Received: 14 September 2020; Accepted: 4 October 2020; Published: 9 October 2020 Abstract: Electrohysterography (EHG) is a promising technique for pregnancy monitoring and preterm risk evaluation. It allows for uterine contraction monitoring as early as the 20th gestational week, and it is a non-invasive technique based on recording the electric signal of the uterine muscle activity from electrodes located in the abdominal surface. In this work, EHG-based contraction detection methodologies are applied using signal envelope features. -

Variation in Fetal Presentations and Positions Among Women in Warri, Delta State, Nigeria
World Research Journal of Obstetrics and Gynecology ISSN: 2277-6001, Volume 2, Issue 1, 2013, pp.-10-12. Available online at http://www.bioinfopublication.org/jouarchive.php?opt=&jouid=BPJ0000126 VARIATION IN FETAL PRESENTATIONS AND POSITIONS AMONG WOMEN IN WARRI, DELTA STATE, NIGERIA OLANIYAN O.T.1*, MERAIYEBU A.B.1, ALELE J.Y.1, DARE J.B.2, ATSUKWEI D.1 AND ADELAIYE A.B.1 1Department of Physiology, Bingham University, Karu, Nasarawa, Nigeria. 2Department of Anatomy, Bingham University, Karu, Nasarawa, Nigeria. *Corresponding Author: Email- [email protected] Received: November 21, 2013; Accepted: December 23, 2013 Abstract- This study investigates the various fetal presentations among women in Warri and the various predisposing factors which may have possibly brought about these variations; the major positions considered were cephalic, breech and transverse, with the considered influencing factors being gestational age of the fetus, maternal age, amniotic fluid volume, parity, and method of previous deliveries. A total of 105 ultra- sound fetal biometries with a total of 108 fetuses, between 15-40 weeks of gestational age, and maternal age between 19 and 40 were used for this study. Fetal ultrasound biometry was used to find out information about the fetus including gestational age, amniotic fluid volume, presentation of the fetus and a questionnaire was used to take information about the mother including maternal age, parity, and method of previous delivery (ies). The result showed that a total of 82 fetuses (75.9%) were Cephalic babies, 19 (17.6%) were Breech and 7 (6.5%) are transverse. Out of the 105 women, there were 102 (77.1% cephalic, 18.3% breech, 4.8% transverse) women with adequate amniotic fluid volume and 1 woman (with a cephalic fetus) with average amniotic fluid volume and 2 women (with transverse foetuses) with low amniotic fluid volume.