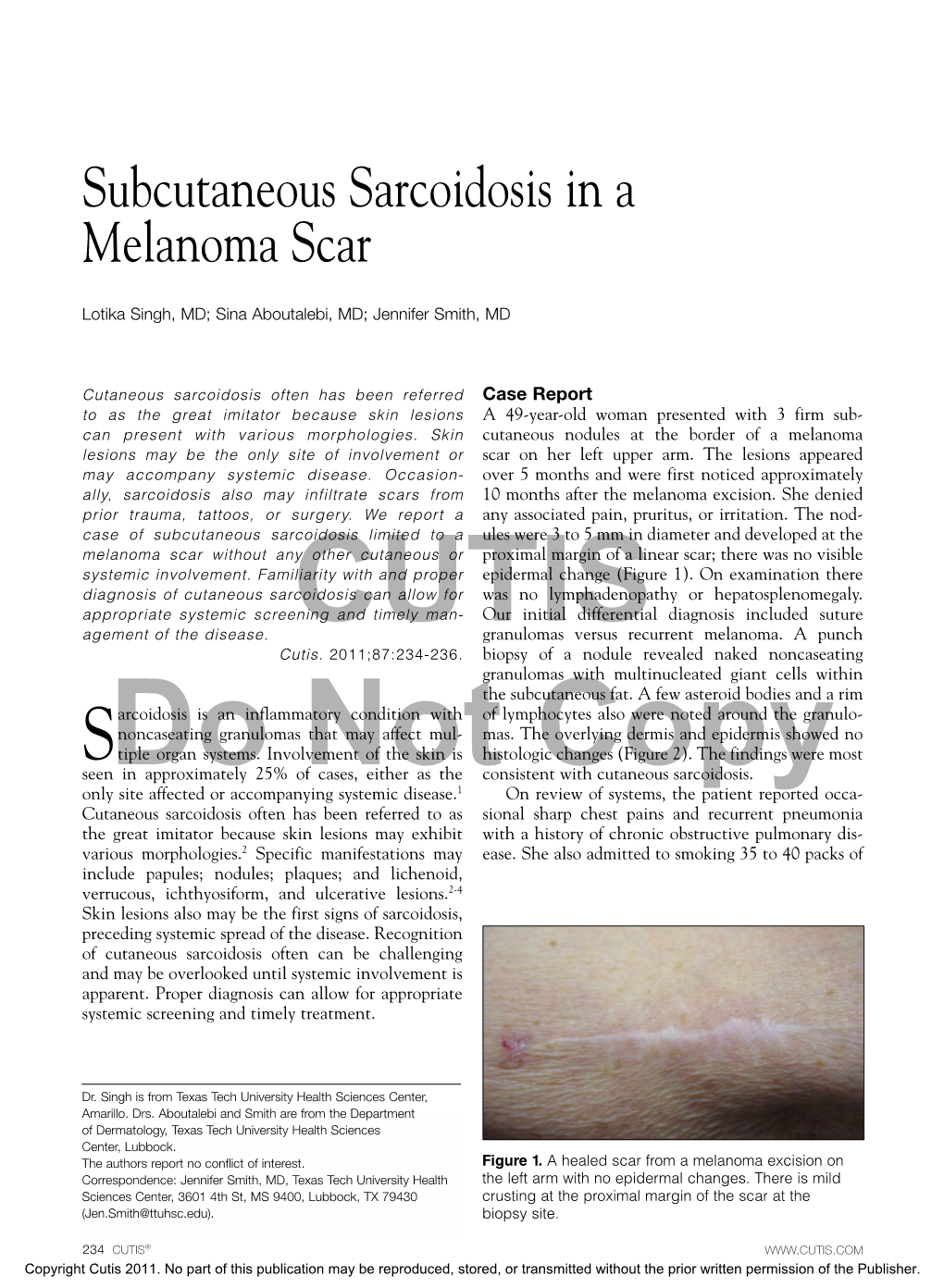
Subcutaneous Sarcoidosis in a Melanoma Scar
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Idiopathic Spiny Keratoderma: a Report of Two Cases and Literature Review
Idiopathic Spiny Keratoderma: A Report of Two Cases and Literature Review Jessica Schweitzer, DO,* Matthew Koehler, DO,** David Horowitz, DO*** *Intern, Largo Medical Center, Largo, FL **Dermatology Resident, Third Year, College Medical Center/Western University, Long Beach, CA ***Dermatology Residency Program Director, College Medical Center/Western University, Long Beach, CA Abstract Spiny keratoderma is a rare and likely underreported condition that presents with punctate hyperkeratotic growths localized to the palms and soles. We present two cases of clinically diagnosed spiny keratoderma. Although the lesions were asymptomatic, patients are at risk of an underlying internal malignancy with this condition, so diagnosis is crucial. Neither men were seeking treatment for the lesions when they were discovered, suggesting that this condition may be much more common than reported. Patients with histories of manual labor, increased UV exposure, and non-melanoma skin cancer (NMSC) may also be at higher risk for developing spiny keratoderma.1 The epidemiology, histopathologic features, differential diagnosis, and current treatments for spiny keratoderma are reviewed. Introduction Case 2 enthusiast for his entire life, spending significant Spiny keratoderma is a rare palmoplantar A 67-year-old Caucasian male presented with a time using his hands to maintain and fire his keratoderma that presents with keratotic, pinpoint one-year history of insidiously growing, pinpoint weapons and many hours outside without sun papules on the palms and soles. There are both hyperkeratotic papules projecting from his palms protection. The patient was referred back to his hereditary and acquired forms. When found, bilaterally (Figures 4-5). He presented to the clinic primary care physician for internal evaluation. -

A Review of the Evidence for and Against a Role for Mast Cells in Cutaneous Scarring and Fibrosis
International Journal of Molecular Sciences Review A Review of the Evidence for and against a Role for Mast Cells in Cutaneous Scarring and Fibrosis Traci A. Wilgus 1,*, Sara Ud-Din 2 and Ardeshir Bayat 2,3 1 Department of Pathology, Ohio State University, Columbus, OH 43210, USA 2 Centre for Dermatology Research, NIHR Manchester Biomedical Research Centre, Plastic and Reconstructive Surgery Research, University of Manchester, Manchester M13 9PT, UK; [email protected] (S.U.-D.); [email protected] (A.B.) 3 MRC-SA Wound Healing Unit, Division of Dermatology, University of Cape Town, Observatory, Cape Town 7945, South Africa * Correspondence: [email protected]; Tel.: +1-614-366-8526 Received: 1 October 2020; Accepted: 12 December 2020; Published: 18 December 2020 Abstract: Scars are generated in mature skin as a result of the normal repair process, but the replacement of normal tissue with scar tissue can lead to biomechanical and functional deficiencies in the skin as well as psychological and social issues for patients that negatively affect quality of life. Abnormal scars, such as hypertrophic scars and keloids, and cutaneous fibrosis that develops in diseases such as systemic sclerosis and graft-versus-host disease can be even more challenging for patients. There is a large body of literature suggesting that inflammation promotes the deposition of scar tissue by fibroblasts. Mast cells represent one inflammatory cell type in particular that has been implicated in skin scarring and fibrosis. Most published studies in this area support a pro-fibrotic role for mast cells in the skin, as many mast cell-derived mediators stimulate fibroblast activity and studies generally indicate higher numbers of mast cells and/or mast cell activation in scars and fibrotic skin. -

An Unusual Course in Bullous Morphea
Case Report An Unusual Course in Bullous Morphea İlknur Kıvanç Altunay, MD, Hilal Kaya Erdoğan*, MD, Nurhan Döner, MD, Damlanur Sakız,1 MD. Address: Dermatology and 1Pathology Departments, Şişli Etfal Training and Research Hospital, Istanbul, 34377, Turkey. * Corresponding Author: Dr. Hilal Kaya Erdoğan, Şisli Etfal Training and Research Hospital. Istanbul, 34377, Turkey. E-mail: [email protected] Published: J Turk Acad Dermatol 2010; 4 (4): 04401c This article is available from: http://www.jtad.org/2010/4/jtad04401c.pdf Key Words: bullous morphea, drug reaction Abstract Observations: We report a 75-year-old woman with bullous morphea characterized by disseminated erythemato-pigmentous plaques and a few blisters on some morphea plaques at the beginning of first visit. While she was under narrow band UV therapy, she discontinued the treatment and refused to have any more after 13 sessions. One month later, she reapplied with extensive bullae and facial edema with severe itching. We learned that she had taken naproxen sodium one a day for two days ten days ago. Bullous drug reaction was diagnosed and systemic cortisone was started. She was in remission after fifteen days. The patient had very different clinical picture on her second visit with extensive, large and cadaverous bullae, facial eryhtema and edema. It seems to be a bullous drug reaction based on bullous morphea. However, it remains a mystery whether this clinical presentation is a peculiar drug reaction or is really a mere exacerbation of existed bullous morphea. Introduction noprost eye drop and tolterodine. These medicati- ons had been used for over a year. Her family his- Bullae formation in lesions of morphea is an tory was unremarkable. -

Oral Frictional Hyperkeratosis (FK)
Patient information Oral frictional hyperkeratosis (FK) What is oral frictional hyperkeratosis? Hyperkeratinisation - excessive growth of stubbornly attached keratin (a fibrous protein produced by the body) - may happen for a number of reasons, and may be genetic (runs in the family), physiological e.g. due to friction from a sharp tooth, pre-malignant (pre-cancerous) and malignant (cancerous). The change may result from chemical, heat or physical irritants. Friction (the constant rubbing of two surfaces against each other) in the mouth may result in benign (non-cancerous) white patches. Various names have been used to describe particular examples of FK, including those resulting from excessive tooth-brushing force (toothbrush keratosis), the constant rubbing of the tongue against the teeth (tongue thrust keratosis), and that produced by the habit of chronic cheek or lip biting (cheek or lip bite keratosis). What are the signs and symptoms of FK? Most patients with FK are free of symptoms. A patient may notice a thickening of an area of skin in the mouth, or FK may be discovered by accident during a routine oral examination. What are the causes of FK? The white patches of FK that develop in the mouth are formed in the same way that calluses form on the skin of hands and feet. The most common causes are long term tissue chewing (biting the inside of the cheek or lips), ill-fitting dentures, jagged teeth, poorly adapted dental fillings or caps, and constant chewing on jaws that have no teeth. The constant irritation encourages the growth of keratin, giving the skin involved a different thickness and colour. -

Investigating Biomarkers of Keloid Scarring
Investigating Biomarkers of Keloid Scarring Zoe Drymoussi 2015 A thesis presented for the degree of Doctor of Philosophy Centre for Cutaneous Research, Blizard Institute, Barts and The London School of Medicine and Dentistry, Queen Mary, University of London 1 Declaration I, Zoe Drymoussi, declare that the work presented in this thesis is my own and has not been submitted in any form for another degree or diploma at any university or other institute of tertiary education. Information derived from the published or unpublished work of others has been acknowledged in the text and a list of references is given. Zoe Drymoussi, PhD Student 1st August 2015 2 Abstract Keloids are fibroproliferative scars that form in response to abnormal healing processes. The extracellular matrix (ECM) remodelling of the dermis in the maturation phase of normal wound healing is insufficient in keloids, leading to excessive ECM proteins being deposited in the granulation tissue. Keloid scars are unique to humans, and show increased prevalence in darker skin types. Current treatments rarely lead to permanent regression, and despite decades of study, the key molecular processes responsible for keloid scarring are still largely elusive. The research presented in this thesis aims to investigate markers of keloid scars, and to examine the impact of both the dermis and epidermis in keloid pathogenesis. Histological examination of the keloid scars showed a thickened epidermis and densely collagenous dermis, both of which demonstrated a higher level of cell proliferation and myofibroblast expression, as compared to normal skin. Differences between the central and marginal regions of the scars were also noted. -

Fundamentals of Dermatology Describing Rashes and Lesions
Dermatology for the Non-Dermatologist May 30 – June 3, 2018 - 1 - Fundamentals of Dermatology Describing Rashes and Lesions History remains ESSENTIAL to establish diagnosis – duration, treatments, prior history of skin conditions, drug use, systemic illness, etc., etc. Historical characteristics of lesions and rashes are also key elements of the description. Painful vs. painless? Pruritic? Burning sensation? Key descriptive elements – 1- definition and morphology of the lesion, 2- location and the extent of the disease. DEFINITIONS: Atrophy: Thinning of the epidermis and/or dermis causing a shiny appearance or fine wrinkling and/or depression of the skin (common causes: steroids, sudden weight gain, “stretch marks”) Bulla: Circumscribed superficial collection of fluid below or within the epidermis > 5mm (if <5mm vesicle), may be formed by the coalescence of vesicles (blister) Burrow: A linear, “threadlike” elevation of the skin, typically a few millimeters long. (scabies) Comedo: A plugged sebaceous follicle, such as closed (whitehead) & open comedones (blackhead) in acne Crust: Dried residue of serum, blood or pus (scab) Cyst: A circumscribed, usually slightly compressible, round, walled lesion, below the epidermis, may be filled with fluid or semi-solid material (sebaceous cyst, cystic acne) Dermatitis: nonspecific term for inflammation of the skin (many possible causes); may be a specific condition, e.g. atopic dermatitis Eczema: a generic term for acute or chronic inflammatory conditions of the skin. Typically appears erythematous, -

Advances in Seborrheic Keratosis
A CME/CE-Certified Supplement to Original Release Date: December 2018 Advances in Seborrheic Expiration Date: December 31, 2020 Estimated Time To Complete Activity: 1 hour Participants should read the activity information, Keratosis review the activity in its entirety, and complete the online post-test and evaluation. Upon completing this activity as designed and achieving a passing score on FACULTY the post-test, you will be directed to a Web page that will Joseph F. Fowler Jr, MD Michael S. Kaminer, MD allow you to receive your certificate of credit via e-mail Clinical Professor and Director Associate Clinical Professor of Dermatology or you may print it out at that time. Contact and Occupational Yale Medical School The online post-test and evaluation can be accessed Dermatology New Haven, Connecticut at http://tinyurl.com/SebK2018. University of Louisville School of Adjunct Assistant Professor of Medicine Medicine (Dermatology), Warren Alpert Medical School Inquiries about continuing medical education (CME) Louisville, Kentucky of Brown University accreditation may be directed to the University of Providence, Rhode Island Louisville Office of Continuing Medical Education & Professional Development (CME & PD) at cmepd@ louisville.edu or (502) 852-5329. Designation Statement eborrheic keratosis (SK) has been called keratinizing surface.12 They can develop virtually The University of Louisville School of Medicine the “Rodney Dangerfield of skin lesions”— anywhere except for the palms, soles, and mucous designates this Enduring material for a maximum of 9 1.0 AMA PRA Category 1 Credit(s)™. Physicians should it earns little respect (as a clinical concern) membranes, but are most commonly observed claim only the credit commensurate with the extent of Sbecause of its benignity, commonality, usual on the trunk and face.6,13 The tendency to develop their participation in the activity. -

“Relationship Between Smoking and Plantar Callus
C HA PTER 3 8 RELATIONSHIP BETWEEN SMOKING AND PLANTAR CALLUS FORMATION OF THE FOOT Thomas J. Merrill, DPM Virginio Vena, DPM Luis A. Rodriguez, DPM Despite the decline in cigarette smoking in the last few smoke can remain in the body (6). The tobacco smoke years as reported by the Centers for Disease Control and components absorbed from the lungs reach the heart Prevention, and the well known health risks in cardiovascular immediately. Smoking increases the heart rate, arterial blood and pulmonary diseases, millions of Americans continue to pressure, and cardiac output. There is a 42% reduction in the smoke cigarettes. It has been proven by both experimental digital blood flow after a single cigarette (7, 8). Nicotine has and clinical observation that cigarettes impair bone and a direct cutaneous vasoconstrictive effect and is the principle wound healing. The purpose of this article is to review the vasoactive component in the gas phase of cigarette smoke. chemical components of cigarette smoke and its relationship It is an odorless, colorless, and poisonous alkaloid that when with plantar callus formation. inhaled or injected, can activate the adrenal catecholamines Increased plantar callus formation with patients who from the adrenergic nerve endings and from the adrenal smoke cigarettes seems to be a common problem. There are medulla, which cause vasoconstriction of vessels especially in approximately 46.6 million smokers in the US. There was a the extremities. Nicotine also induces the sympathetic decline during 1997-2003 in the youth population but nervous system, which results in the release of epinephrine during the last years the rates are stable (1). -

Linear Scleroderma “En Coup De Sabre” Coexisting with Plaque-Morphea
661 J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.74.5.661 on 1 May 2003. Downloaded from SHORT REPORT Linear scleroderma “en coup de sabre” coexisting with plaque-morphea: neuroradiological manifestation and response to corticosteroids I Unterberger, E Trinka, K Engelhardt, A Muigg, P Eller, M Wagner, N Sepp, G Bauer ............................................................................................................................. J Neurol Neurosurg Psychiatry 2003;74:661–664 progression of skin lesions or any neurological abnormalities A 24 year old woman in the 33rd week of pregnancy during follow up. developed progressive neurological complications with On admission the patient was in the 33rd week of right sided hemiparesis in association with the occurrence pregnancy. She was fully oriented, had normal speech, and of linear scleroderma “en coup de sabre” (LSCS) and pre- presented with a right sided hemiparesis (grade 3/5, MRC existing plaque-morphea, already being treated by scale) with a positive Babinski sign on the right. There was no balneophototherapy. Further progression of neurological history of head trauma. symptoms led to a caesarean section with the delivery of a Routine laboratory testing and comprehensive serological healthy child. Brain magnetic resonance imaging (MRI) screening including antineutrophilic cytoplasmic antibodies showed focal T2 signal increases in the left frontoparietal (ANCA), anticardiolipin antibodies, and antibodies against region directly adjacent to the area of LSCS. -
Nodular Morphea
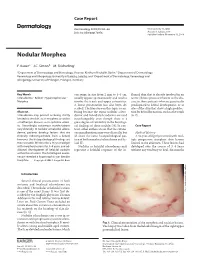
Case Report Dermatology 2009;218:63–66 Received: July 13, 2008 DOI: 10.1159/000173976 Accepted: July 23, 2008 Published online: November 13, 2008 Nodular Morphea a b c F. Kauer J.C. Simon M. Sticherling a b Department of Dermatology and Venerology, Vivantes Klinikum Neukölln, Berlin , Department of Dermatology, c Venerology and Allergology, University of Leipzig, Leipzig , and Department of Dermatology, Venerology and Allergology, University of Erlangen, Erlangen , Germany Key Words can range in size from 2 mm to 4–5 cm, flamed skin that is already involved in an -Scleroderma ؒ Keloid ؒ Hypertrophic scar ؒ usually appear spontaneously and tend to active fibrotic process inherent to the dis Morphea involve the trunk and upper extremities. ease in those patients who are genetically A linear presentation has also been de- predisposed to keloid development, or at scribed. The literature on this topic is con- sites of the skin that show a high predilec- Abstract fusing because the terms ‘nodular sclero- tion for keloid formation, such as the trunk Scleroderma may present as being strictly derma’ and ‘keloidal scleroderma’ are used [6, 7] . limited to the skin, as in morphea, or within interchangeably even though there is a a multiorgan disease, as in systemic sclero- great degree of variability in the histologi- sis. Accordingly, cutaneous manifestations cal findings of these nodules [4] . In con- C a s e R e p o r t vary clinically. In nodular or keloidal sclero- trast, other authors stress that the cutane- derma, patients develop lesions that are ous manifestations may vary clinically, but Medical History clinically indistinguishable from a keloid; all share the same histopathological pat- A 16-year-old girl presented with mul- however, the histopathological findings are tern of both morphea/scleroderma and ke- tiple progressive morpheic skin lesions more variable. -

Basal Cell Papilloma, Senile Keratosis, Seborrheic Wart)
ATLAS OF HEAD AND NECK PATHOLOGY SEBORRHEIC KERATOSIS SEBORRHEIC KERATOSIS (BASAL CELL PAPILLOMA, SENILE KERATOSIS, SEBORRHEIC WART) These lesions, often multiple, and occurring for the most part after 50 years of age, are most common on the face and upper body. They are brownish to black, slightly greasy, slightly raised, with either a smooth or mildly verrucous surface and a “stuck-on” appearance. They measure from a few millimeters to several centimeters in diameter. Microscopically, there is variance in appearance but all types show hyperkerato- sis, acanthosis (thickening of the epidermis) and a papillary formation sharply demar- cated from the adjacent epidermis. Generally a straight line drawn from one edge of the lesion to the other will pass just under the deeper part of the tumor. Horny invaginations from the epidermis appear on cross-section as pseudo- horn cysts and there are also true horn cysts. Both of these cysts show complete keratinization, concentrically arranged, and only a thin granulosal cell layer. Melanin is prevalent in many tumors and accounts for the dark appearance as seen clinically. Both squamous and basal (“basaloid”) cells are seen in this lesion and they are ar- ranged in sheets. In some types of seborrheic keratoses there are interwoven tracts of basal cells and in others the basal cells are in nests. Intercellular bridges are common. Seborrheic keratosis, showing how the tumor tends to have a straight edge along its deep margin. Also seen are acantho- sis (large arrow), papillary projections (triangles), and hyperkeratosis (small arrows). Several cysts are present with keratin concentrically arranged. Most of the epithelial cells here are dark and, having the appearance of epidermoid basal cells, are called basaloid cells. -

Seborrheic Keratosis
Benign Epidermal and Dermal Tumors REAGAN ANDERSON, DO- PROGRAM DIRECTOR, COLORADO DERMATOLOGY INSTITUTE, RVU PGY3 RESIDENTS- JONATHAN BIELFIELD, GEORGE BRANT PGY2 RESIDENT- MICHELLE ELWAY Seborrheic Keratosis Common benign growth seen after third/fourth decade of life Ubiquitous among older individuals Tan to black, macular, papular, or verrucous lesion Occur everywhere except palms, soles, and mucous membranes Can simulate melanocytic neoplasms Pathogenesis: Sun exposure- Australian study found higher incidence in the head/neck Alteration in distribution of epidermal growth factors Somatic activating mutations in fibroblast growth factor receptor and phosphoinositide-3-kinase Seborrheic Keratosis Sign of Leser-Trelat: Rare cutaneous marker of internal malignancy • Gastric/colonic adenocarcinoma, breast carcinoma, and lymphoma m/c • Abrupt increase in number/size of SKs that can occur before, during, or after an internal malignancy is detected • 40% pruritus • M/C location is the back • Malignant acanthosis nigricans may also appear in 20% of patients • Should resolve when primary tumor is treated, and reappear with recurrence/mets Seborrheic Keratosis 6 Histologic types Acanthotic Hyperkeratotic Reticulated Irritated Clonal Melanoacanthoma Borst-Jadassohn phenomenon Well-demarcated nests of keratinocytes within the epidermis Seborrheic Keratoses Treatment Reassurance Irritated SKs (itching, catching on clothes, inflamed) Cryotherapy, curettage, shave excision Pulsed CO2, erbium:YAG lasers Electrodessication Flegel