The Case of Primary Health Care Services in Akwa Ibom State
Total Page:16
File Type:pdf, Size:1020Kb

Load more
Recommended publications
-

Comparative Analysis of Public and Private Borehole Water Supply Sources in Uruan Local Government Area of Akwa Ibom State
International Journal of Applied Science and Technology Vol. 3 No. 1; January 2013 Comparative Analysis of Public and Private Borehole Water Supply Sources in Uruan Local Government Area of Akwa Ibom State Ukpong, E. C B. B. Okon Civil Engineering Department Faculty of Engineering University of Uyo Akwa Ibom State, Nigeria Abstract Comparative analysis of public and private borehole water supply sources in Uruan Local Government Area of Akwa Ibom State, Nigeria, was conducted in order to examine their qualities. A total of 13 water samples collected from 10 randomly selected private and 3 functional public boreholes in the area were analysed using standard analytical techniques and instruments. Most of the physicochemical parameters of samples from the two sources were within the acceptable limits of the World Health Organisation (WHO) for drinking water. Eight different bacteria species were isolated and identified. They include Escherichia coli (18.75%), Bacillus subtilis (15.625%), Streptococcus faecalis (15.625%), Proteus vulgaris (12.50%), Klebsiella aerogenes (12.50%), Micrococcus varians (9.375%), Clostridium perfringens (9.37%) and Staphylococcus aureus (6.25%). Total viable count on private borehole water samples ranged from 1.6x103 to 5.5x103cfu/ml while that of the public was 9x101cfu/ml. In the private source, E.coli ranged from 1x100 to 4x100cfu/100ml, whereas 4x100 to 3.4x101cfu/100ml was recorded for the coliforms. Streptococcus faecalis and Clostridium perfringens ranged from 1x100 to 3x100cfu/100ml and 1x100 to 2x100cfu/100ml respectively, and did not meet the approved drinking water standard. There was no growth of indicator organism in samples from the public boreholes. -
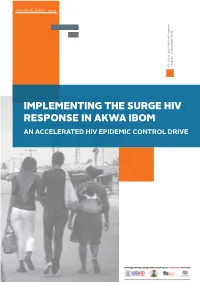
Implementing the Surge Hiv Response in Akwa Ibom an Accelerated Hiv Epidemic Control Drive Content
TECHNICAL BRIEF - 2019 A technical guide for local program local program for guide A technical Ibom State... in Akwa managers IMPLEMENTING THE SURGE HIV RESPONSE IN AKWA IBOM AN ACCELERATED HIV EPIDEMIC CONTROL DRIVE CONTENT 1 Understanding the shape of the HIV epidemic in Akwa Ibom 2 Rationale for the surge HIV response 3 Overaching themes of the surge HIV response 4 Community antiretroviral therapy management (CAM) 5 Preimplementation activities 6 The community antiretroviral therapy management team 7 HIV case finding; the fulcrum point of the surge HIV response 8 Linkage to antiretroviral therapy 9 Viral load services in the context of community ART services 10 Coordination and monitoring of CAM services 11 Conclusion 12 Annex TECHNICAL GUIDANCE TECHNICAL GUIDE PAGE 3 UNDERSTANDING THE SHAPE OF THE HIV EPIDEMIC IN AKWA IBOM STATE Fig 1: HIV prevalence in Nigeria (NAIIS 2018) Nigeria has made progress in the fight against HIV/AIDS. The just concluded national AIDS indicator impact survey (NAIIS) revealed that the national Estimated 13,000 new cases prevalence of HIV is 1.4% with an estimated 1.9 million people infected with per year Adolescents 15-19 years the virus. With a mixed epidemic, only 7 out of the 36 states in the country account for 5000 cases % Incidence among cohabiting partners: 1.60 ---- AKAIS account for over 50% of this burden. The top 3 states by burden include Rivers, Benue and Akwa Ibom states. Akwa Ibom state has the highest prevalence in the country at 5.5% with an estimated burden of 178,000 people living with HIV. -

125 Timber Dealers' Perception of Their Knowledge of the Forest Law
International Multi-Disciplinary Journal Vol. 3 (1), 2009 ISSN 1994-9057 (Print) ISSN 2070-0083 (Online) Timber Dealers’ Perception of their Knowledge of the Forest Law in Uyo Senatorial District of Akwa Ibom State, Nigeria (Pp. 125-135) Enefiok S. Udo , - Department of Forestry and Wildlife, University of Uyo, P.M.B. 1017, Uyo, Nigeria Samuel I. Udofia - Department of Forestry and Wildlife, University of Uyo, P.M.B. 1017, Uyo, Nigeria. Olajide, O. - Department of Forestry and Wildlife, University of Uyo, P.M.B. 1017, Uyo, Nigeria. Abstract This study investigated timber dealers’ knowledge of the forest law and regulations in Uyo Senatorial District. Five timber markets were selected through two-stage sampling. Data were collected from 238 traders in the selected markets using structured questionnaires and subjected to descriptive and inferential statistics. Results showed that over 90% of the respondents knew and understood the forest law and penalties for violation. Thus, forest offences were not committed out of ignorance, but for undue profits. Knowledge and understanding of the law were independent of respondents’ Local Government Areas (LGAs), but knowledge of penalties for forest offences significantly varied with LGA (p = 0.05). Recommendations for improved compliance with the law and its enforcement strategies include employment of more forest policemen, provision of vehicles for patrol and evacuation of illegal forest produce, adequate penalties on culprits, and adequate political will and earnest tackling of corruption by government. Key words: Timber dealers, Knowledge, Forest Law, Uyo Senatorial District, Nigeria. Copyright © IAARR 2009: www.afrrevjo.com 125 Indexed African Journals Online: www.ajol.info African Research Review Vol. -

Socioeconomic Development Inequalities Among Geographic Units in Akwa Ibom State, Nigeria Umoren, V
Ethiopian Journal of Environmental Studies and Management Vol. 6 No.3 2013 SOCIOECONOMIC DEVELOPMENT INEQUALITIES AMONG GEOGRAPHIC UNITS IN AKWA IBOM STATE, NIGERIA UMOREN, V. E. http://dx.doi.org/10.4314/ejesm.v6i3.11 Received 12th February 2013; accepted 17th April 2013 Abstract Socio-economic development inequality among geographic units is a phenomenon common in both the developed and developing countries. Regional inequality may result in dissension among geographic units of the same state due to the imbalance in socio-economic development. This study examines the inequality and the pattern in socio-economic development in Akwa Ibom State. Data on socio-economic development indicators was collected using field survey, questionnaire and data from relevant agencies across the 24 areas or nodes selected out of the 31 areas or nodes. The factor analysis technique was applied to the 26 variables to achieve a parsimonious description and identify the major factors to indicate the socio-economic dimensions. From the analysis seven major factors were identified. Factor 1 identified and named as education/communication factor, factor 2 identified and named Health institution/small scale industry factor, factor 3 identified and named as means of transport factor, factor 4 identified and named as land area factor, factor 5 identified and named as distance factor, factor 6 identified and named as income/household size factor and factor 7 identified and named as car ownership factor. The total variance for the factors is 82%. The study revealed that there exist variation and patterns in the socio-economic development in the study area.The pattern shows factor 1 has Essien Udium and Onna indicating high performance .Factor 2 , has 3 areas that indicate high performance Okobo, Ibeno, and Oruk Anam.Factor 3 has 3 areas that indicate high performance Ibesikpo Asutan, Abak and Etinan. -

S/No Accreditation Number Name of Driving School Address 1 Frsc/00446/Akb/0016 Aa Driving School Akwa Ibom 132,Nsikak Eduok, Uy
S/NO ACCREDITATION NUMBER NAME OF DRIVING SCHOOL ADDRESS 1 FRSC/00446/AKB/0016 AA DRIVING SCHOOL AKWA 132,NSIKAK EDUOK, UYO AKWA IBOM IBOM STATE 2 FRSC/00222/AKB/0013 AKAMASIO DRIVER'S 155, UDO UMANA STREET,UYO, TRAINING CENTRE AKWA IBOM 3 FRSC/00710/AKB/0017 AKWA IMA DRIVING SCHOOL NO. 1 IKOT OBIOBO ROAD ANUA OBIO, UYO, AKWA IBOM STATE 4 FRSC/00711/AKB/0018 A-Z INT’L DRIVING SCH 5, UBI INYANG STRRT UYO AKWA IBOM 5 FRSC/00004/AKB/0002 CODESWAY DRIVING UYO TOWNSHIP. SCHOOL 6 FRSC/00221/AKB/0012 DABOO DRIVING SCHOOL 78 ABIAKPO ROAD IKOT EKPENE. 7 FRSC/00223/AKB/0014 FAITH DRIVING SCHOOL 1 EDEM UDO STR. EKET. EKET 8 FRSC/00008/AKB/0006 GODSWILL NO 151 EKET ORON ROAD,EKET. GENERALMECHANICAL A/IBOM DRIVING SCHOOL 9 FRSC/00005/AKB/0003 ID DRIVING SCHOOL NO. 76, NWANGA IBA ROAD UYO. 10 FRSC/00006/AKB/0004 JEKAS INTERNATIONAL 5 SANNI OGUN ROAD IKOT- DRIVING SCHOOL EKPENE. 11 FRSC/00010/AKB/0008 KOKO DRIVING SCHOOL 68, AKA OBOT IDIM RD UYO. 12 FRSC/00007/AKB/0005 MIDDLE SEX DRIVING NO.19 URUAN STR. UYO AKWA SCHOOL IBOM 13 FRSC/00713/AKB/0020 MT DRIVING SCHOOL 273 NWANAIBA ROAD UYO 14 FRSC/00445/AKB/0015 OJETOR DRIVERS TRAINING NO 2 OFFOT ROAD ABAK CENTRE 15 FRSC/00012/AKB/0010 UDUAK ABASI DRIVING 230 IDORO ROAD UYO. SCHOOL 16 FRSC/00011/AKB/0009 UNIMESCO INTERNATIONAL 25,NWANBA RD IDU URUAN LGA DRIVING SCHOOL AKWA IBOM. 17 FRSC/00003/AKB/0001 VICTORY DRIVING SCHOOL NO. 56 ABA ROAD,IKOT EKPENE UYO 18 FRSC/00712/AKB/0019 WISDOM DRIVING SCH IKOT ESE.IKOT MKPORIKPO ETIM EKPO A/IBOM 19 FRSC/00890/AKB/0021 SUCCESS MOTOR DRIVING NO.15 IBAKA STREET ORON, -

Sustainable Efficiencies in Small Scale Cassava Farmers in Oruk Anam Local Government Area of Akwa Ibom State, Nigeria
Agrosearch, 19(2): 64-86 (2019) https://dx.doi.org/10.4314/agrosh.v19i2.6 SUSTAINABLE EFFICIENCIES IN SMALL SCALE CASSAVA FARMERS IN ORUK ANAM LOCAL GOVERNMENT AREA OF AKWA IBOM STATE, NIGERIA *Akpan, S. B., Udo, U. J., and Okon, U. E. Department of Agricultural Economics and Extension, Akwa Ibom State University, Obio Akpa Campus, Akwa Ibom State, Nigeria *Corresponding Author: [email protected]. ABSTRACT This study derived sustainable technical, economic and allocative efficiencies from a set of efficiencies generated from the maximum likelihood estimation of stochastic production and profit functions fitted with data collected from small scale cassava farmers. The study was conducted in Oruk Anam Local Government Area of Akwa Ibom State, Nigeria. A three-stage sampling method was employed to select choose respondents’ to which structured questionnaire was administered to obtain the necessary information for the study. The result revealed an average sustainable technical efficiency of 81.60%, 30.40% for profit efficiency and 38.40% for allocative efficiency. Results further showed that farming experience, membership in social organization, years of formal education, farm capital and farm size were the positive determinants of sustainable technical efficiency while household size, number of female cultivating cassava, poor farming households and the use of organic manure were negative. In the same Vein, farming experience, education farm size, gender and the use of tillage technology were identified as positive determinants of sustainable economic or profit efficiency while household size and quantity of fertilizer use had negative impacts. Similarly, cassava farmers’ farm size, age, educational level, farming experience, gender and the use of tillage technology impacted positively on sustainable allocative efficiency while household size and the quantity of fertilizer have negative relationships. -

Assessment of Surface and Ground Water Quality of Uruan in Akwa Ibom State of Nigeria
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by International Institute for Science, Technology and Education (IISTE): E-Journals Journal of Natural Sciences Research www.iiste.org ISSN 2224-3186 (Paper) ISSN 2225-0921 (Online) Vol.4, No.6, 2014 Assessment of Surface and Ground Water Quality of Uruan in Akwa Ibom State of Nigeria Imaobong Udousoro *and Ini Umoren Chemistry Department, University of Uyo, Uyo, P. M. B. 1017, Uyo, Akwa Ibom State, Nigeria *E-mail of corresponding author: [email protected] Abstract The water quality status of rivers, streams, and underground water in Uruan Local Government Area, Nigeria was investigated in this study. Inhabitants of this region depend on these water resources for drinking and other purposes. Water samples were collected from four rivers, nine streams, six boreholes and a well from various points across three study zones in the local government. Standard analytical methods were employed for all analyses and the results are compared with water quality standards of the World Health Organisation (WHO) and the Nigerian Standard for Drinking Water Quality (NSDWQ). Most quality determinands are within WHO guidelines except pH, EC, turbidity, TDS, total coliform, and Fe. The overall ionic dominance pattern for the - - - river, stream, borehole and well follow the same trend Fe>Na>Mn>K and Cl >NO 3 >NO 2 . The hygienic condition of the water bodies is found to be poor. High BOD 5, coliform count and BOD 5:NO 3 ratio of river, stream and ground water samples are indicative of organic pollution due to faecal contamination. -

Akwa Ibom Vo L U M E 1 , N U M B E R 1
Explore Akwa Ibom Vo l u m e 1 , N u m b e r 1 UGE: Building an Akwa Ibom for all Akwa Ibom: An Investment Destination People, Arts & Culture www.akwaibomstate.gov.ng f © Ministry of Information & Strategy 2021 Free Copy for more on Akwa Ibom CALL our Info HOTLINE 070 0000 0001 call, text & whatsapp www.akwaibomstate.gov.ng Inside... Inside Akwa Ibom Quick Facts 04 Editorial Suite 05 Now, Akwa Ibom is Home 10 Akwa Ibom is Home to Foreigners 12 Akwa Ibom is a Destination for any Serious Business Person 12 Tropicana Mall 16 Investment Opportunities 18 Akwa Ibom Udom Emmanuel in the Eye of Others 23 The People and Culture 07 Some Places of Interest 29 ...Potentials Tourism The Bridge of No Return The 21 Storey 13 Ibeno Beach 14 09 Dakkada Tower Ikot Ekpene Raffia UGE: Building an Ibom Air: Redefining the 21 Akwa Ibom for all 26 Nigerian airspace' Editorial Team Publisher Editor Graphics The Ministry of Information and James Edet Nsikan Ekwere Strategy/Nouveau Edge PR Edidiong George Production Editors Editor-in-Chief Aniekan Ukpong Photography Comrade Ini Ememobong Idris Mabadeje Mbedabasi Etim (Carrot) Editorial Adviser Ubokobong Udo Akpan Contributors Inyang Jameson Annie Essienette Concept Glory James General Editor Nouveau Edge PR Marvelous Friday © A Production of The Ministry of Information and Strategy/Nouveau Edge PR for more on Akwa Ibom, call our Info HOTLINE 070 0000 0001 03 Explore call, text & whatsapp Akwa Ibom AKWA IBOM Quick facts Dakkada Tower, Uyo Area: 7,249 Square kilometers o 0 Ibom Location: Lying between Latitudes 4 32" and 5 33" Connection, Uyo North and Longitudes 7035 and 8025 east. -

A Case Study of Odiok Itam and Ibiaku Uruan Rivers in Itu and Uruan Local Government Area of Akwa Ibom, Nigeria
Available online a twww.scholarsresearchlibrary.com Scholars Research Library Archives of Applied Science Research, 2014, 6 (6):7-15 (http://scholarsresearchlibrary.com/archive.html) ISSN 0975-508X CODEN (USA) AASRC9 Water quality assessment: A case study of Odiok Itam and Ibiaku Uruan Rivers in Itu and Uruan local government area of Akwa Ibom, Nigeria Denise E. M. and John V. S. Department of Botany and Ecological Studies, University of Uyo, Uyo, AkwaIbom State, Nigeria _________________________________________________________________________________________ ABSTRACT A study on the effects of anthropogenic activities on water quality of OdiokItam and IbiakuUruan rivers in Itu and Uruan Local Government Areas of AkwaIbom state were assessed on the basis of their physicochemical parameters between January and December 2013. The following ranges were obtained for the parameter assessed. pH(5.4-5.9), electrical conductivity(11-38µs/cm), total dissolved solids (1.7-6.5mg/l), dissolved oxygen (0.31-0.7mg/L), biological oxygen demand (1.4-1.8mg/L), chemical oxygen demand (21-66mg/L), sulphate (0.6-6.8mg/L), phosphate (0.03-0.2.3mg/L), and calcium (2.2-3.7mg/L). The pH was slightly acidic across the stations. Values obtained forother physicochemical parameters falls within the WHO permissible limit. The results show the absence of pollution threat arising from anthropogenic activities in the various stations. The water of the above rivers could be considered safe for domestic purpose . Key words: Water quality assessment, Anthropogenic and physicochemical properties _____________________________________________________________________________________________ INTRODUCTION Globally, water is one of the most abundant and essential commodities of man and occupies about 97% of the earth surface. -
Projected Population 2007 - 2015
GOVERNMENT OF AKWA IBOM STATE OF NIGERIA PROJECTED POPULATION 2007 - 2015 MINISTRY OF ECONOMIC DEVELOPMENT UYO, AKWA IBOM STATE April, 2014 PREFACE This is the first edition of the publication on the projected population of Akwa Ibom State. It covers the period 2007 – 2015 and gives the projected population of the State by year, sex, residence, age group and Local Government Area. The projection was obtained from 2006 population census figure for Akwa Ibom State using the acceptable growth rate of 3.4 per cent all round. The growth rate was obtained from the National Population Commission, Akwa Ibom State Office, Uyo. The projection was done by staff of the Directorate of Statistics, Ministry of Economic n Development and is based on the Compound Interest Formula, P n = P o + (1 + r) , where; Pn = projected population for year n Po = 2006 population census figure 1 = constant r = population growth rate for Akwa Ibom State n = number of years On behalf of the Permanent Secretary and staff of Ministry of Economic Development, I wish to thank His Excellency, the Executive Governor of Akwa Ibom State, Chief Godswill O. Akpabio (CON), for the love and support to enhance the production of quality and timely statistics in the State. It is hoped that this publication will be useful to politicians, academicians, researchers, Non-Governmental Organizations (NGOs), students, industrialists and the general public in their day-to-day activities. Akan Okon Honourable Commissioner Ministry of Economic Development Akwa Ibom State April, 2014 i TABLE -

Women's Participation in Lower Ikpa River Fisheries of Akwa Ibom State
FSN-PW 0011 WOMEN’S PARTICIPATION IN LOWER IKPA RIVER FISHERIES OF AKWA IBOM STATE, NIGERIA: A CASE STUDY OF IFIAYONG EKPO, I. E. and UDOH, J. P. Department of Fisheries and Aquaculture, University of Uyo, Uyo Copyright 2010, Fisheries Society of Nigeria. INTRODUCTION This paper was prepared for presentation at the 25th Annual International Conference and Exhibition in Administrative Staff College of Nigeria Fisheries is an important sub-sector of the (ASCON), Topo-Badagry, Lagos, Nigeria, 25th – 29th October, 2010. Nigerian economy (Shinkafi, 2007) which This paper was selected for presentation by an FISON Program Committee following review of information contained in an abstract submitted by the attracts various participants and author(s). Contents of the paper, as presented, have not been reviewed by the Fisheries Society of Nigeria and are subject to correction by the author(s). contributors to the economic development The material, as presented, does not necessarily reflect any position of the Fisheries Society of Nigeria, its officers, or members. Papers presented at of the nation. Fishing is the main FISON meetings are subject to publication review by Editorial Committees of the Fisheries Society of Nigeria. Electronic reproduction, distribution, or occupation of the people of Akwa Ibom storage of any part of this paper for commercial purposes without the written consent of the Fisheries Society of Nigeria is prohibited. Permission to State of Nigeria. The State is blessed with reproduce in print is restricted to an abstract of not more than 300 words; illustrations may not be copied. The abstract must contain conspicuous several networks of streams, rivers and acknowledgement of where and by whom the paper was presented. -

Determinants of Obong Victor Attah International Airport, Akwa Ibom State on the Employment Status of the Host Communities
Arts and Humanities Open Access Journal Review Article Open Access Determinants of obong victor attah international airport, Akwa Ibom state on the employment status of the host communities Abstract Volume 3 Issue 4 - 2019 The aviation industry has a vital role to play in achieving sustainable development in Ihuoma Blossom Adindu,1 Joseph C Udoh,1 austerity nations like Africa, particularly in Nigeria. Interestingly, Africa accounts for just 2 2% of world GDP but hosts 13% of its population. As a result, GDP per capita in Africa is Raimi Morufu Olalekan 1Department of Geography and Natural Resources the lowest of the world’s regions. The general picture is one of underdevelopment, political Management, Faculty of Social Sciences, University of Uyo, instability, economic volatility and pervasive poverty. While there is a major opportunity to Nigeria improve living standards, quality of life and alleviate poverty through sustained economic 2Department of Community Medicine, Environmental Health growth. This research work measured the contributions of the Obong Victor Attah Unit, Faculty of Clinical Sciences, Niger Delta University, International Airport to the social and economic life of host communities of Uruan, Okobo Wilberforce Island, Nigeria and Nsit-Atai. LGA’s in Akwa-Ibom State. Employment is one of the major parameters used in measuring these contributions. A buffer was used to demarcate the study into zones Correspondence: Raimi Morufu Olalekan, Department of and a systematic sampling technique was employed in selecting the households to be Community Medicine, Environmental Health Unit, Faculty of sampled. The sample size composed of 400 respondents and this was determined from the Clinical Sciences, Niger Delta University, Wilberforce Island, population of the host communities using the Taro Yamane formula.