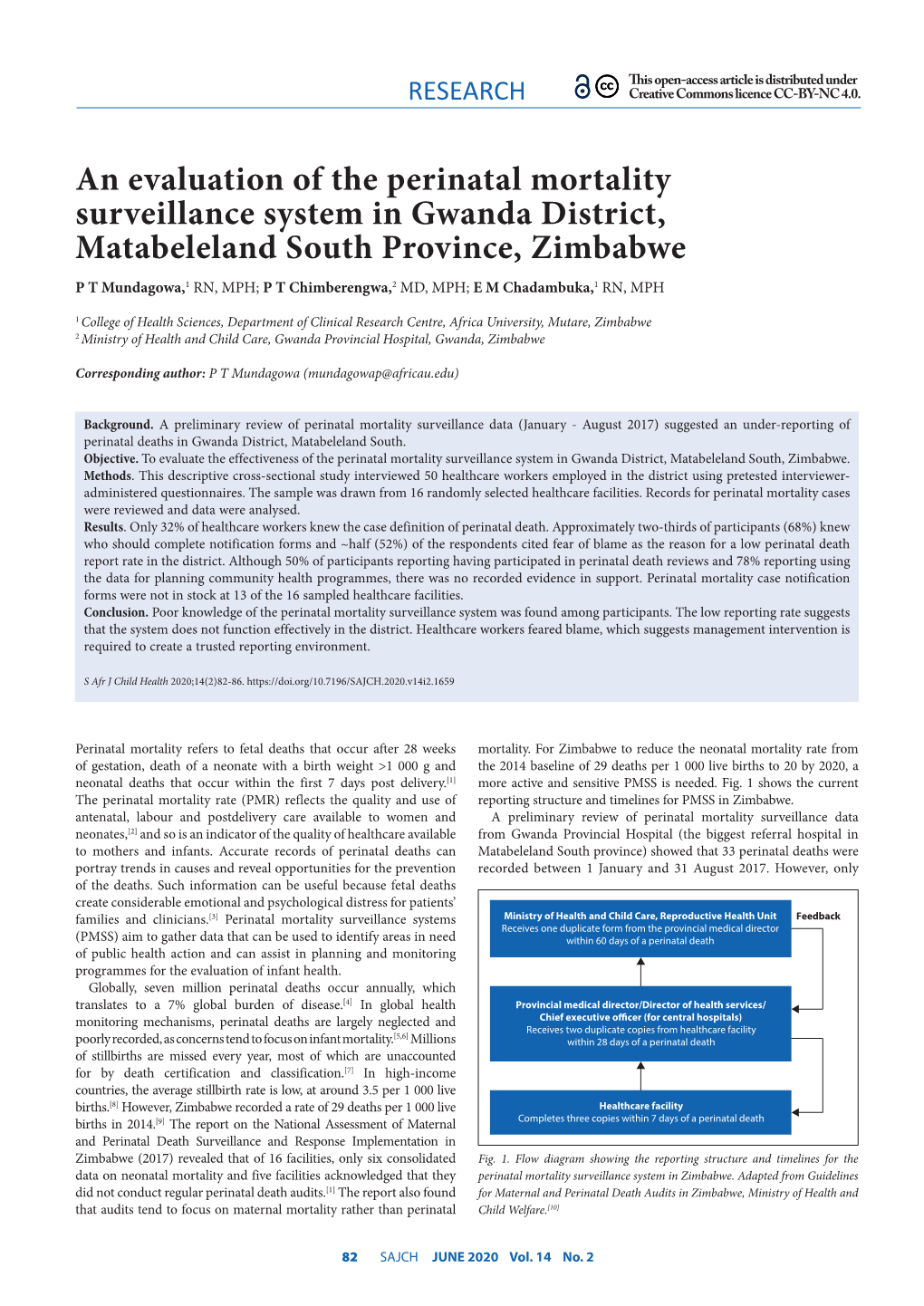
An Evaluation of the Perinatal Mortality Surveillance System in Gwanda
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Mopane Woodlands and the Mopane Worm: Enhancing Rural Livelihoods and Resource Sustainability
Mopane Woodlands and the Mopane Worm: Enhancing rural livelihoods and resource sustainability Final Technical Report Edited by Jaboury Ghazoul1, Division of Biology, Imperial College London Authors and contributors Mopane Tree Management: Dirk Wessels2, Member Mushongohande3, Martin Potgeiter7 Domestication Strategies: Alan Gardiner4, Jaboury Ghazoul Kgetsie ya Tsie Case Study: John Pearce5 Livelihoods and Marketing: Jayne Stack6, Peter Frost7, Witness Kozanayi3, Tendai Gondo3, Nyarai Kurebgaseka8, Andrew Dorward9, Nigel Poole5 New Technologies: Frank Taylor10, Alan Gardiner Choice experiments: Robert Hope11, Witness Kozanayi, Tendai Gondo Mopane worm diseases: Robert Knell12 Start and End Date 1 May 2001 – 31 January 2006 DFID Project Reference Number R 7822 Research Programme Forestry Research Programme (FRP) Research Production System Forest Agriculture Interface 1 Also ETH Zürich, Department of Environmental Sciences, ETH Zentrum CHN, Universitätstrasse 16, Zürich 8092, Switzerland 2 Department of Botany, university fo the North, South Africa 3 Forest Commission, Harare, Zimbabwe 4 Veld Products Research and Development, Gabarone, and Division of Biology, Imperial College London 5 Kgetsie ya Tsie, Tswapong Hills, Botswana 6 Imperial College London and University of Zimbabwe, Project Co-ordinator 7 Institute of Environmental Studies 8 Southern Alliance for Indigenous Resources 9 Imperial College London, Centre for Environmental Policy. 10 Veld Products Research and Development 11 University of Newcastle 12 Queen Mary College, University of London 1 Contents Executive Summary 3 Background 3 Project Purpose 6 Research Activities Section 1. Mopane tree ecology and management 7 Section 2.1 Mopane worm productivity and domestication 18 Section 2.2 Mini-livestock: Rural Mopane Worm Farming at the Household Level 34 Section 3. A case study of the Kgetsie ya Tsie community enterprise model for managing and trading mopane worms 59 Section 4. -

Malaria Outbreak Investigation in a Rural Area South of Zimbabwe: a Case–Control Study Paddington T
Mundagowa and Chimberengwa Malar J (2020) 19:197 https://doi.org/10.1186/s12936-020-03270-0 Malaria Journal RESEARCH Open Access Malaria outbreak investigation in a rural area south of Zimbabwe: a case–control study Paddington T. Mundagowa1* and Pugie T. Chimberengwa2 Abstract Background: Ninety percent of the global annual malaria mortality cases emanate from the African region. About 80–90% of malaria transmissions in sub-Saharan Africa occur indoors during the night. In Zimbabwe, 79% of the population are at risk of contracting the disease. Although the country has made signifcant progress towards malaria elimination, isolated seasonal outbreaks persistently resurface. In 2017, Beitbridge District was experiencing a second malaria outbreak within 12 months prompting the need for investigating the outbreak. Methods: An unmatched 1:1 case–control study was conducted to establish the risk factors associated with con- tracting malaria in Ward 6 of Beitbridge District from week 36 to week 44 of 2017. The sample size constituted of 75 randomly selected cases and 75 purposively selected controls. Data were collected using an interviewer-administered questionnaire and Epi Info version 7.2.1.0 was used to conduct descriptive, bivariate and multivariate analyses of the factors associated with contracting malaria. Results: Fifty-two percent of the cases were females and the mean age of cases was 29 13 years. Cases were diag- nosed using rapid diagnostic tests. Sleeping in a house with open eaves (OR: 2.97; 95% CI± 1.44–6.16; p < 0.01), spend- ing the evenings outdoors (OR: 2.24; 95% CI 1.04–4.85; p 0.037) and sleeping in a poorly constructed house (OR: 4.33; 95% CI 1.97–9.51; p < 0.01) were signifcantly associated= with contracting malaria while closing eaves was protec- tive (OR: 0.45; 95% CI 0.20–1.02; p 0.055). -

Nyasa Clandestine Migration Through Southern Rhodesia Into the Union of South Africa: 1920S – 1950S
Settling in Motion: Nyasa Clandestine Migration through Southern Rhodesia into the Union of South Africa: 1920s – 1950s Anusa Daimon Centre for Africa Studies University of the Free State Bloemfontein, South Africa Abstract Illegal African migration into South Africa is not uniquely a post-apartheid phenomenon. It has its antecedents in the colonial/apartheid period. The South Africa colonial economy relied heavily on cheap African labour from both within and outside the Union. Most foreign migrant labourers came from the then Nyasaland (Malawi) and Portuguese East Africa (Mozambique) through official channels of the Witwatersrand Native Labour Association (WNLA). WNLA was active throughout the Southern Africa and competed for the same labour resource with other regional supranational ‘native’ labour recruitment agencies, providing various incentives to lure and transport potential employees to its bustling South African gold and diamond mining industry. However, not all migrant labourers found their way through formal WNLA channels. Using archival material from repositories in Harare (Zimbabwe), Zomba (Malawi), Grahamstown (South Africa), London and Oxford (UK), the article casts light on illicit migration mainly by Malawian labourers (Nyasas) through Southern Rhodesia into South Africa between the 1920s and 1950s. It argues that many transient Nyasas subverted the inhibitive WNLA contractual obligations by clandestinely migrating independently into the Union. They also exploited the labour recruitment infrastructure used by the state and labour bureaus to swiftly move across Southern Rhodesia. In essence, Nyasas settled in motion, using Southern Rhodesia as a stepping-stone or springboard en-route to the more lucrative Union of South Africa. An appreciation of such informal migration opens up space for creating a more comprehensive historiography of labour migration in Southern Africa. -
Fire Report 2014
ANNUAL FIRE REPORT 2014 FIRE Hay bailing along the Victoria Falls- Kazungula Road to reduce road side fires Page 1 of 24 ANNUAL FIRE REPORT 2014 Table of Contents 1.0 Introduction ......................................................................................................................................... 3 2.0 Fire Prediction Modelling ..................................................................................................................... 3 3.0 Fire Monitoring .................................................................................................................................... 7 4.0 Environmental Education and Training ................................................................................................ 8 5.0 EMA/ZRP Fire Management Awards ................................................................................................. 14 6.0 Law enforcement ............................................................................................................................... 17 7.0 Impacts of Fires .................................................................................................................................. 18 7.0 Conclusion .......................................................................................................................................... 21 8.0 Recommendations ............................................................................................................................. 22 Annex 1: Pictures .................................................................................................................................... -

Determinants of Exclusive Breastfeeding Among Mothers of Infants Aged 6 to 12 Months in Gwanda District, Zimbabwe Paddington T
Mundagowa et al. International Breastfeeding Journal (2019) 14:30 https://doi.org/10.1186/s13006-019-0225-x RESEARCH Open Access Determinants of exclusive breastfeeding among mothers of infants aged 6 to 12 months in Gwanda District, Zimbabwe Paddington T. Mundagowa1*, Elizabeth M. Chadambuka1, Pugie T. Chimberengwa2 and Fadzai Mukora-Mutseyekwa3 Abstract Background: In 2016, 98% of children in Zimbabwe received breastmilk, however only 40% of babies under six months were exclusively breastfed 24 h prior to data collection. A 2014 survey revealed that Matabeleland South Province had the country’s highest starvation rates and food insecurities were rife. This study aimed at investigating maternal, infant, household, environmental and cultural factors influencing exclusive breastfeeding (EBF) practice in Gwanda District. Methods: A cross-sectional study was conducted from January to March 2018. Interviews used pretested structured questionnaires for 225 mothers of infants aged between six and twelve months at immunization outreach points and health facilities. Descriptive statistics, bivariate and multivariate analysis estimated the association between the dependent and independent variables. Exclusive breastfeeding was defined as feeding an infant on breast milk only from birth up to the age of six months. Results: The majority of mothers (n = 193; 89%) had knowledge about EBF and 189 (84%) expressed a positive attitude towards the practice, however, only 81 (36%) practiced exclusive breastfeeding. The most common complementary food/fluid given to the infants was plain water (n = 85; 59%). Predictors for EBF were: maternal Human Immuno-deficiency Virus positive status (Odds Ratio [OR] 0.30; 95% Confidence Interval [CI] 0.17, 0.56) and being economically independent (OR 0.41; 95% CI 0.21, 0.79). -

For Human Dignity
ZIMBABWE HUMAN RIGHTS COMMISSION For Human Dignity REPORT ON: APRIL 2020 i DISTRIBUTED BY VERITAS e-mail: [email protected]; website: www.veritaszim.net Veritas makes every effort to ensure the provision of reliable information, but cannot take legal responsibility for information supplied. NATIONAL INQUIRY REPORT NATIONAL INQUIRY REPORT ZIMBABWE HUMAN RIGHTS COMMISSION ZIMBABWE HUMAN RIGHTS COMMISSION For Human Dignity For Human Dignity TABLE OF CONTENTS FOREWORD .................................................................................................................................................. vii ACRONYMS.................................................................................................................................................... ix GLOSSARY OF TERMS .................................................................................................................................. xi PART A: INTRODUCTION TO THE NATIONAL INQUIRY PROCESS ................................................................ 1 CHAPTER 1: INTRODUCTION ........................................................................................................................ 1 1.1 Establishment of the National Inquiry and its Terms of Reference ....................................................... 2 1.2 Methodology ..................................................................................................................................... 3 CHAPTER 2: THE NATIONAL INQUIRY PROCESS ......................................................................................... -

The Food Poverty Atlas
Zimbabwe Food Poverty Atlas2016_FINAL.qxp_Layout 1 4/10/2016 10:44 Page 1 The Food Poverty Atlas SMALL AREA FOOD POVERTY ESTIMATION Statistics for addressing food and nutrition insecurity in Zimbabwe SEPTEMBER, 2016 Zimbabwe Food Poverty Atlas2016_FINAL.qxp_Layout 1 4/10/2016 10:44 Page 2 2 Zimbabwe Food Poverty Atlas2016_FINAL.qxp_Layout 1 4/10/2016 10:44 Page i The Food Poverty Atlas SMALL AREA FOOD POVERTY ESTIMATION Statistics for addressing food and nutrition insecurity in Zimbabwe SEPTEMBER, 2016 i Zimbabwe Food Poverty Atlas2016_FINAL.qxp_Layout 1 4/10/2016 10:44 Page ii © UNICEF Zimbabwe, The World Bank and Zimbabwe National Statistics Agency All rights reserved. No part of this report may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording or by any information storage or retrieval system, without permission in writing from the publishers. Zimbabwe National Statistics Agency 20th Floor, Kaguvi Building, Cnr 4th Street and Central Avenue, Harare, Zimbabwe P.O. Box CY342, Causeway, Harare, Zimbabwe. Tel: (+263-4) 706681/8 or (+263-4) 703971/7 Fax: (+263-4) 762494 E-mail: [email protected] This publication is available on the following websites: www.unicef.org/zimbabwe www.worldbank.org/ www.zimstat.co.zw/ ISBN: 978-92-806-4824-9 The Food Poverty Atlas was produced by the Zimbabwe National Statistics Agency (ZIMSTAT). Technical and financial support was provided by the United Nations Children’s Fund (UNICEF) and the World Bank Design and layout: K. Moodie Photographs by: © UNICEF/2015/T. Mukwazhi ii Zimbabwe Food Poverty Atlas2016_FINAL.qxp_Layout 1 4/10/2016 10:44 Page iii Food poverty prevalence at a glance Map 1: Food poverty prevalence by district* Figure 1 400,000 Number of food poor 350,000 and non poor households 300,000 250,000 by province* 200,000 150,000 100,000 50,000 0 Harare Central N.B 1. -

OPHID Annual Report 2019.Pdf
ANNUAL REPORT 2019 Table of Contents Table of Contents ............................................................................ 1 Acknowledgements ......................................................................... 2 Acronyms ........................................................................................ 3 Executive Director’s Statement - ..................................................... 6 Chairperson’s Statement – .............................................................. 8 Treasurer’s Statement – .................................................................. 9 Families and Communities for the Elimination of HIV .................... 11 The Cervical Cancer Screening and Treatment (C-CAST) ............ 17 Zimbabwe Emergency Response – Integrating HIV services into Humanitarian preparedness and response plans .......................... 18 Mbereko+Men: Tackling barriers to Accessing Maternal, Neonatal and Child Health Services in Zimbabwe ........................................ 19 Documenting Evidence and Learning ............................................ 21 OPHID ACCEPTED ABSTRACTS: IAS 2019: Mexico City Mexico, July 21-24 2019 ............................................................ 21 OPHID ACCEPTED ABSTRACTS: INTEREST 2019, Accra, Ghana, May 14-17 2019 ............................................................ 23 OPHID ACCEPTED ABSTRACTS: ICASA Conference, Kigali, Rwanda, 7 Abstracts (all FACE HIV Program/USAID): 1 oral abstract, 6 posters .................................................................... -

University of Pretoria Etd – Nsingo, SAM (2005)
University of Pretoria etd – Nsingo, S A M (2005) - 181 - CHAPTER FOUR THE PROFILE, STRUCTURE AND OPERATIONS OF THE BEITBRIDGE RURAL DISTRICT COUNCIL INTRODUCTION This chapter describes the basic features of the Beitbridge District. It looks at the organisation of the Beitbridge Rural District Council and explores its operations as provided in the Rural District Councils Act of 1988 and the by-laws of council. The chapter then looks at performance measurement in the public sector and local government, in particular. This is followed by a discussion of democratic participation, service provision and managerial excellence including highlights of their relevance to this study. BEITBRIDGE DISTRICT PROFILE The Beitbridge District is located in the most southern part of Zimbabwe. It is one of the six districts of Matebeleland South province. It shares borders with Botswana in the west, South Africa in the south, Mwenezi District from the north to the east, and Gwanda District in the northwest. Its geographical area is a result of amalgamating the Beitbridge District Council and part of the Mwenezi- Beitbridge Rural District Council. The other part of the latter was amalgamated with the Mwenezi District to form what is now the Mwenezi District Council. Significant to note, from the onset, is that Beitbridge District is one of the least developed districts in Zimbabwe. Worse still, it is located in region five (5), which is characterized by poor rainfall and very hot conditions. As such, it is not suitable for crop farming, although this takes place through irrigation schemes. University of Pretoria etd – Nsingo, S A M (2005) - 182 - The district is made up of an undulating landscape with shrubs, isolated hills and four big rivers. -

The Geology of the Country East of Beitbridge
ZIMBABWE GEOLOGICAL SURVEY BULLETIN NO. 87 The Geology of the Country East of Beitbridge by MPR LIGHT & TJ. BRODERICK ISSUED BY AUTHORITY HARARE 1998 PREFACE Bulletin No. 87 and accompanying 1: I 00000 scale map describes the geology of an area about 1765 km2 in Beitbridge District. The area is bounded by longitudes 300 00' E to 300 30' E, and latitude 220 00' S, the southern boundary being the Limpopo River. M.P.R. Light carried out the geological mapping between 1973 and 1975, and the map was published in 1981. Publication of the Bulletin text, rc-written by TJ. Broderick, was delayed by lack of funds. This publication has bcen madc possible, courtesy of funds provided by Centrum fuer Internationale Migration unci Entwicklung (CIM) of Frankfurt, Germany. The area first described by Carl Mauch in 187 I comprises complexly deformed gneisses and granulites of the Central Zone of the Limpopo Mobile Belt. Rare exposures of enderbites and dioritic gneisses form a basement to the Beitbridge Group deposited as various sediments, limestones and volcanic rocks, but now intensely cleformed and metamorphosed to clifferent gneisses and granulites. Karoo sediments lying uneonfonnably on the Beitbridge Group, are preserved in grabens. The whole area is intensely fractured. Most fractures are radial to post Karoo volcanic centres, and are filled by dykes of various rock types. Patt 11 of the Bulletin describes the cconomic geology of the area. Bcitbridge West has been subject to numerous Exclusive Prospecting Orders concerned mainly with exploration for base metals, Messina-type copper mineralization in particular. Though few claims were pegged, there has not been any mining of base metals from the area. -

ZIMBABWEAN GOVERNMENT GAZETTE Published by Authority
ZIMBABWEAN GOVERNMENT GAZETTE Published by Authority Vol. XCIX, No. 60 21st MAY, 2021 Price RTGS$155,00 General Notice 974 of 2021. Bidding documents are available at Chipinge Town Council offices upon payment of a non-refundable tender fee of CHAMINUKA RURAL DISTRICT COUNCIL ZW$800,00, for each document. Tenders in sealed envelopes clearly marked with tender number Invitation to Competitive Bidding must be hand delivered or couriered to the undermentioned address before the closing date and time shown. TENDERS are invited from reputable and registered companies for the supply of the following: The Acting Town Secretary, Chipinge Town Council, Tender number Stand No. 281, Emmerson Dambudzo Mnangagwa Street, CRDC.06/2021. Supply and delivery of building materials. Closing PO. Box 90, date: 1st June, 2021. Chipinge. CRDC.07/2021. Supply and delivery of a borehole drilling rig. Tel: 027-2653/2734/2858/3239/3321 Quantity: 1. Closing date: 1st June, 2021. Email: [email protected] CRDC.08/2021. Supply, installation and configuration of wide area General Notice 976 of 2021. network. Site visit date: 2nd June, 2021. Closing date: 10th June, 2021. NYANGA RURAL DISTRICT COUNCIL Tender conditions Invitation to Competitive Bidding 1. Tender document must be obtained upon payment of a non-refundable fee of ZWL$800,00, from Chaminuka Rural District Council, Adams Plot Offices, Shamva or NYANGA Rural District Council is inviting bids from reputable bidders registered with Procurement Regulatory Authority of upon written request to pmu.chaminukardc@gmail. Zimbabwe to participate in the following tender: com Tender number 2. Tenders must be enclosed in sealed envelopes and endorsed on the outside with advertised tender number NRDC.02/2021. -

Examining the Sources of Smallholder Horticultural
Bindu Samuel,Chigusiwa Lloyd., Int. J. Eco. Res., 2013, v4i6, 1-12 ISSN: 2229-6158 EXAMINING THE SOURCES OF SMALLHOLDER HORTICULTURAL FARMERS EXCLUSION FROM FORMAL URBAN MARKETS IN ZIMBABWE: THE CASE OF CHIHOTA COMMUNAL AREAS Bindu Samuel1 Chigusiwa Lloyd Department of Economics, Bindura University of Science Education Abstract The study seeks to establish why some smallholder horticultural famers in Chihota communal areas market their produce in communal markets which are known to generate less revenue for any given quality and quantity of produce than urban formal markets. It uses primary data collected from 119 farming households randomly selected from four villages that were selected on the basis of horticultural intensity. MLE technique through logit analysis is used to establish the determinants of smallholder horticultural farmers’ exclusion from formal urban markets. The results show that while diversification and household size reduces participation in urban markets, having own transport, input use, land size, age of the household head and access to information increase farmer participation in urban markets. Policy to improve SHFs participation should thus increase specialization, transport availability, input use and information access to SHFs. Keywords Smallholder horticulture farmers, communal markets, market exclusion 1 Introduction At independence, in 1980, the new Zimbabwean majority government prioritized correction of developmental imbalances created by the colonial regime (GoZ, 1982). Chief among the priorities of the new government was black empowerment and rural development. Rural development was a priority since most of the black majority lived in reserve and tribal trust lands which are now known as communal areas2. Most of these communal areas had lagged behind in development due to the reserve status accorded to them.