Specialty Injectables Prior Authorization List
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Genmab and ADC Therapeutics Announce Amended Agreement for Camidanlumab Tesirine (Cami)
Genmab and ADC Therapeutics Announce Amended Agreement for Camidanlumab Tesirine (Cami) Media Release Copenhagen, Denmark and Lausanne, Switzerland, October 30, 2020 • ADC Therapeutics to continue the development and commercialization of Cami • Genmab to receive mid-to-high single-digit tiered royalty Genmab A/S (Nasdaq: GMAB) and ADC Therapeutics SA (NYSE: ADCT) today announced that they have executed an amended agreement for ADC Therapeutics to continue the development and commercialization of camidanlumab tesirine (Cami). The parties first entered into a collaboration and license agreement in June 2013 for the development of Cami, an antibody drug conjugate (ADC) which combines Genmab’s HuMax®-TAC antibody targeting CD25 with ADC Therapeutics’ highly potent pyrrolobenzodiazepine (PBD) warhead technology. Under the terms of the 2013 agreement, the parties were to determine the path forward for continued development and commercialization of Cami upon completion of a Phase 1a/b clinical trial. ADC Therapeutics previously announced that Cami achieved an overall response rate of 86.5%, including a complete response rate of 48.6%, in Hodgkin lymphoma patients in this trial who had received a median of five prior lines of therapy. Cami is currently being evaluated in a 100-patient pivotal Phase 2 clinical trial intended to support the submission of a Biologics License Application (BLA) to the U.S. Food and Drug Administration (FDA). The trial is more than 50 percent enrolled and ADC Therapeutics anticipates reporting interim results in the first half of 2021. “We have a long-standing relationship with the ADC Therapeutics team and believe they are an ideal partner for the ongoing development and potential commercialization of Cami,” said Jan van de Winkel, Ph.D., Chief Executive Officer of Genmab. -

Draft Minutes PDCO 12-15 November 2019
11 December 2019 EMA/PDCO/615413/2019 Inspections, Human Medicines Pharmacovigilance and Committees Division Paediatric Committee (PDCO) Minutes for the meeting on 12-15 November 2019 Chair: Koenraad Norga – Vice-Chair: Sabine Scherer Health and safety information In accordance with the Agency’s health and safety policy, delegates are to be briefed on health, safety and emergency information and procedures prior to the start of the meeting. Disclaimers Some of the information contained in these minutes is considered commercially confidential or sensitive and therefore not disclosed. With regard to intended therapeutic indications or procedure scopes listed against products, it must be noted that these may not reflect the full wording proposed by applicants and may also vary during the course of the review. Additional details on some of these procedures will be published in the PDCO Committee meeting reports (after the PDCO Opinion is adopted), and on the Opinions and decisions on paediatric investigation plans webpage (after the EMA Decision is issued). Of note, this set of minutes is a working document primarily designed for PDCO members and the work the Committee undertakes. Further information with relevant explanatory notes can be found at the end of this document. Note on access to documents Some documents mentioned in these minutes cannot be released at present following a request for access to documents within the framework of Regulation (EC) No 1049/2001 as they are subject to on- going procedures for which a final decision has not yet been adopted. They will become public when adopted or considered public according to the principles stated in the Agency policy on access to documents (EMA/127362/2006). -

Activity of Rituximab and Ofatumumab Against Mantle
ACTIVITY OF RITUXIMAB AND OFATUMUMAB AGAINST MANTLE CELL LYMPHOMA(MCL) IN VITRO IN MCL CELL LINES BY COMPLEMENT DEPENDENT CYTOTOXICITY (CDC)AND ANTIBODY-DEPENDENT CELL MEDIATED CYTOTOXICITY ASSAYS(ADCC) Dr. Gopichand Pendurti M.B.B.S Mentor: Dr. Francisco J. Hernandez-Ilizaliturri MD Overview of presentation •Introduction to mantle cell lymphoma. •Concept of minimal residual disease. •Anti CD 20 antibodies. •51Cr release assays. •Flow cytometry on cell lines. •Results. •Future. MANTLE CELL LYMPHOMA •Mantle cell lymphoma is characterized by abnormal proliferation of mature B lymphocytes derived from naïve B cells. •Constitutes about 5% of all patients with Non Hodgkin's lymphoma. •Predominantly in males with M:F ratio 2.7:1 with onset at advanced age (median age 60yrs). •It is an aggressive lymphoma with median survival of patients being 3-4 years. •Often presents as stage III-IV with lymphadenopathy, hepatosplenomegaly, gastrointestinal involvement, peripheral blood involvement. Pedro Jares, Dolors Colomer and Elias Campo Genetic and molecular pathogenesis of mantle cell lymphoma: perspectives for new targeted therapeutics Nature revision of cancer 2007 October:7(10):750-62 •Genetic hallmark is t(11:14)(q13:q32) translocation leading to over expression of cyclin D1 which has one of the important pathogenetic role in deregulating the cell cycle. •Other pathogentic mechanisms include molecular and chromosomal alterations that Target proteins that regulate the cell cycle and senecense (BMI1,INK4a,ARF,CDK4 AND RB1). Interfere with cellular -

Pharmacologic Considerations in the Disposition of Antibodies and Antibody-Drug Conjugates in Preclinical Models and in Patients
antibodies Review Pharmacologic Considerations in the Disposition of Antibodies and Antibody-Drug Conjugates in Preclinical Models and in Patients Andrew T. Lucas 1,2,3,*, Ryan Robinson 3, Allison N. Schorzman 2, Joseph A. Piscitelli 1, Juan F. Razo 1 and William C. Zamboni 1,2,3 1 University of North Carolina (UNC), Eshelman School of Pharmacy, Chapel Hill, NC 27599, USA; [email protected] (J.A.P.); [email protected] (J.F.R.); [email protected] (W.C.Z.) 2 Division of Pharmacotherapy and Experimental Therapeutics, UNC Eshelman School of Pharmacy, University of North Carolina at Chapel Hill, Chapel Hill, NC 27599, USA; [email protected] 3 Lineberger Comprehensive Cancer Center, University of North Carolina at Chapel Hill, Chapel Hill, NC 27599, USA; [email protected] * Correspondence: [email protected]; Tel.: +1-919-966-5242; Fax: +1-919-966-5863 Received: 30 November 2018; Accepted: 22 December 2018; Published: 1 January 2019 Abstract: The rapid advancement in the development of therapeutic proteins, including monoclonal antibodies (mAbs) and antibody-drug conjugates (ADCs), has created a novel mechanism to selectively deliver highly potent cytotoxic agents in the treatment of cancer. These agents provide numerous benefits compared to traditional small molecule drugs, though their clinical use still requires optimization. The pharmacology of mAbs/ADCs is complex and because ADCs are comprised of multiple components, individual agent characteristics and patient variables can affect their disposition. To further improve the clinical use and rational development of these agents, it is imperative to comprehend the complex mechanisms employed by antibody-based agents in traversing numerous biological barriers and how agent/patient factors affect tumor delivery, toxicities, efficacy, and ultimately, biodistribution. -

Chemokine Receptors in Allergic Diseases Laure Castan, A
Chemokine receptors in allergic diseases Laure Castan, A. Magnan, Grégory Bouchaud To cite this version: Laure Castan, A. Magnan, Grégory Bouchaud. Chemokine receptors in allergic diseases. Allergy, Wiley, 2017, 72 (5), pp.682-690. 10.1111/all.13089. hal-01602523 HAL Id: hal-01602523 https://hal.archives-ouvertes.fr/hal-01602523 Submitted on 11 Jul 2018 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Distributed under a Creative Commons Attribution - ShareAlike| 4.0 International License Allergy REVIEW ARTICLE Chemokine receptors in allergic diseases L. Castan1,2,3,4, A. Magnan2,3,5 & G. Bouchaud1 1INRA, UR1268 BIA; 2INSERM, UMR1087, lnstitut du thorax; 3CNRS, UMR6291; 4Universite de Nantes; 5CHU de Nantes, Service de Pneumologie, Institut du thorax, Nantes, France To cite this article: Castan L, Magnan A, Bouchaud G. Chemokine receptors in allergic diseases. Allergy 2017; 72: 682–690. Keywords Abstract asthma; atopic dermatitis; chemokine; Under homeostatic conditions, as well as in various diseases, leukocyte migration chemokine receptor; food allergy. is a crucial issue for the immune system that is mainly organized through the acti- Correspondence vation of bone marrow-derived cells in various tissues. Immune cell trafficking is Gregory Bouchaud, INRA, UR1268 BIA, rue orchestrated by a family of small proteins called chemokines. -

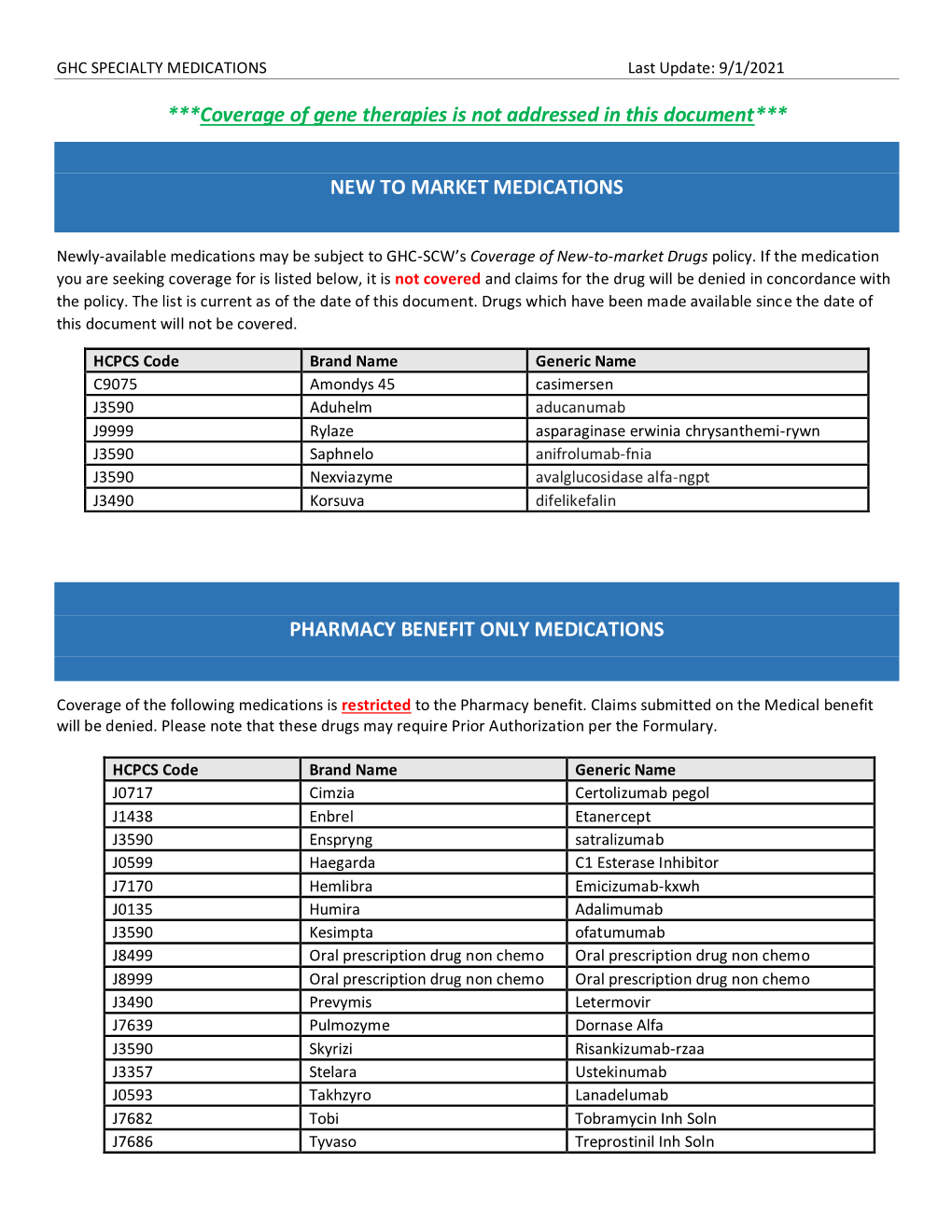
DRUGS REQUIRING PRIOR AUTHORIZATION in the MEDICAL BENEFIT Page 1
Effective Date: 08/01/2021 DRUGS REQUIRING PRIOR AUTHORIZATION IN THE MEDICAL BENEFIT Page 1 Therapeutic Category Drug Class Trade Name Generic Name HCPCS Procedure Code HCPCS Procedure Code Description Anti-infectives Antiretrovirals, HIV CABENUVA cabotegravir-rilpivirine C9077 Injection, cabotegravir and rilpivirine, 2mg/3mg Antithrombotic Agents von Willebrand Factor-Directed Antibody CABLIVI caplacizumab-yhdp C9047 Injection, caplacizumab-yhdp, 1 mg Cardiology Antilipemic EVKEEZA evinacumab-dgnb C9079 Injection, evinacumab-dgnb, 5 mg Cardiology Hemostatic Agent BERINERT c1 esterase J0597 Injection, C1 esterase inhibitor (human), Berinert, 10 units Cardiology Hemostatic Agent CINRYZE c1 esterase J0598 Injection, C1 esterase inhibitor (human), Cinryze, 10 units Cardiology Hemostatic Agent FIRAZYR icatibant J1744 Injection, icatibant, 1 mg Cardiology Hemostatic Agent HAEGARDA c1 esterase J0599 Injection, C1 esterase inhibitor (human), (Haegarda), 10 units Cardiology Hemostatic Agent ICATIBANT (generic) icatibant J1744 Injection, icatibant, 1 mg Cardiology Hemostatic Agent KALBITOR ecallantide J1290 Injection, ecallantide, 1 mg Cardiology Hemostatic Agent RUCONEST c1 esterase J0596 Injection, C1 esterase inhibitor (recombinant), Ruconest, 10 units Injection, lanadelumab-flyo, 1 mg (code may be used for Medicare when drug administered under Cardiology Hemostatic Agent TAKHZYRO lanadelumab-flyo J0593 direct supervision of a physician, not for use when drug is self-administered) Cardiology Pulmonary Arterial Hypertension EPOPROSTENOL (generic) -

Phase I/II Study Evaluating the Safety and Clinical Efficacy of Temsirolimus and Bevacizumab in Patients with Chemotherapy Refra
Investigational New Drugs (2019) 37:331–337 https://doi.org/10.1007/s10637-018-0687-5 PHASE II STUDIES Phase I/II study evaluating the safety and clinical efficacy of temsirolimus and bevacizumab in patients with chemotherapy refractory metastatic castration-resistant prostate cancer Pedro C. Barata1 & Matthew Cooney2 & Prateek Mendiratta 2 & Ruby Gupta3 & Robert Dreicer4 & Jorge A. Garcia3 Received: 25 September 2018 /Accepted: 16 October 2018 /Published online: 7 November 2018 # Springer Science+Business Media, LLC, part of Springer Nature 2018 Summary Background Mammalian target of rapamycin (mTOR) pathway and angiogenesis through vascular endothelial growth factor (VEGF) have been shown to play important roles in prostate cancer progression. Preclinical data in prostate cancer has suggested the potential additive effect dual inhibition of VEGF and mTOR pathways. In this phase I/II trial we assessed the safety and efficacy of bevacizumab in combination with temsirolimus for the treatment of men with metastatic castration-resistant prostate cancer (mCRPC). Methods In the phase I portion, eligible patients received temsirolimus (20 mg or 25 mg IV weekly) in combination with a fixed dose of IV bevacizumab (10 mg/kg every 2 weeks). The primary endpoint for the phase II portion was objective response measured by either PSA or RECIST criteria. Exploratory endpoints included changes in circulating tumor cells (CTC) and their correlation with PSA response to treatment. Results Twenty-one patients, median age 64 (53–82), with pre- treatment PSA of 205.3 (11.1–1801.0), previously treated with a median of 2 (0–5) lines of therapy for mCRPC received the combination of temsirolimus weekly at 20 mg (n =4)or25mg(n = 17) with bevacizumab 10 mg/kg every 2 weeks (n =21). -

(CHMP) Agenda for the Meeting on 22-25 February 2021 Chair: Harald Enzmann – Vice-Chair: Bruno Sepodes
22 February 2021 EMA/CHMP/107904/2021 Human Medicines Division Committee for medicinal products for human use (CHMP) Agenda for the meeting on 22-25 February 2021 Chair: Harald Enzmann – Vice-Chair: Bruno Sepodes 22 February 2021, 09:00 – 19:30, room 1C 23 February 2021, 08:30 – 19:30, room 1C 24 February 2021, 08:30 – 19:30, room 1C 25 February 2021, 08:30 – 19:30, room 1C Disclaimers Some of the information contained in this agenda is considered commercially confidential or sensitive and therefore not disclosed. With regard to intended therapeutic indications or procedure scopes listed against products, it must be noted that these may not reflect the full wording proposed by applicants and may also vary during the course of the review. Additional details on some of these procedures will be published in the CHMP meeting highlights once the procedures are finalised and start of referrals will also be available. Of note, this agenda is a working document primarily designed for CHMP members and the work the Committee undertakes. Note on access to documents Some documents mentioned in the agenda cannot be released at present following a request for access to documents within the framework of Regulation (EC) No 1049/2001 as they are subject to on- going procedures for which a final decision has not yet been adopted. They will become public when adopted or considered public according to the principles stated in the Agency policy on access to documents (EMA/127362/2006). Official address Domenico Scarlattilaan 6 ● 1083 HS Amsterdam ● The Netherlands Address for visits and deliveries Refer to www.ema.europa.eu/how-to-find-us Send us a question Go to www.ema.europa.eu/contact Telephone +31 (0)88 781 6000 An agency of the European Union © European Medicines Agency, 2021. -

New Biological Therapies: Introduction to the Basis of the Risk of Infection
New biological therapies: introduction to the basis of the risk of infection Mario FERNÁNDEZ RUIZ, MD, PhD Unit of Infectious Diseases Hospital Universitario “12 de Octubre”, Madrid ESCMIDInstituto de Investigación eLibraryHospital “12 de Octubre” (i+12) © by author Transparency Declaration Over the last 24 months I have received honoraria for talks on behalf of • Astellas Pharma • Gillead Sciences • Roche • Sanofi • Qiagen Infections and biologicals: a real concern? (two-hour symposium): New biological therapies: introduction to the ESCMIDbasis of the risk of infection eLibrary © by author Paul Ehrlich (1854-1915) • “side-chain” theory (1897) • receptor-ligand concept (1900) • “magic bullet” theory • foundation for specific chemotherapy (1906) • Nobel Prize in Physiology and Medicine (1908) (together with Metchnikoff) Infections and biologicals: a real concern? (two-hour symposium): New biological therapies: introduction to the ESCMIDbasis of the risk of infection eLibrary © by author 1981: B-1 antibody (tositumomab) anti-CD20 monoclonal antibody 1997: FDA approval of rituximab for the treatment of relapsed or refractory CD20-positive NHL 2001: FDA approval of imatinib for the treatment of chronic myelogenous leukemia Infections and biologicals: a real concern? (two-hour symposium): New biological therapies: introduction to the ESCMIDbasis of the risk of infection eLibrary © by author Functional classification of targeted (biological) agents • Agents targeting soluble immune effector molecules • Agents targeting cell surface receptors -

Therapeutic Inhibition of VEGF Signaling and Associated Nephrotoxicities
REVIEW www.jasn.org Therapeutic Inhibition of VEGF Signaling and Associated Nephrotoxicities Chelsea C. Estrada,1 Alejandro Maldonado,1 and Sandeep K. Mallipattu1,2 1Division of Nephrology, Department of Medicine, Stony Brook University, Stony Brook, New York; and 2Renal Section, Northport Veterans Affairs Medical Center, Northport, New York ABSTRACT Inhibition of vascular endothelial growth factor A (VEGFA)/vascular endothelial with hypertension and proteinuria. Re- growth factor receptor 2 (VEGFR2) signaling is a common therapeutic strategy in ports describe histologic changes in the oncology, with new drugs continuously in development. In this review, we consider kidney primarily as glomerular endothe- the experimental and clinical evidence behind the diverse nephrotoxicities associ- lial injury with thrombotic microangiop- ated with the inhibition of this pathway. We also review the renal effects of VEGF athy (TMA).8 Nephrotic syndrome has inhibition’s mediation of key downstream signaling pathways, specifically MAPK/ also been observed,9 with the clinical ERK1/2, endothelial nitric oxide synthase, and mammalian target of rapamycin manifestations varying according to (mTOR). Direct VEGFA inhibition via antibody binding or VEGF trap (a soluble decoy mechanism and direct target of VEGF receptor) is associated with renal-specific thrombotic microangiopathy (TMA). Re- inhibition. ports also indicate that tyrosine kinase inhibition of the VEGF receptors is prefer- Current VEGF inhibitors can be clas- entially associated with glomerulopathies such as minimal change disease and FSGS. sifiedbytheirtargetofactioninthe Inhibition of the downstream pathway RAF/MAPK/ERK has largely been associated VEGFA-VEGFR2 pathway: drugs that with tubulointerstitial injury. Inhibition of mTOR is most commonly associated with bind to VEGFA, sequester VEGFA, in- albuminuria and podocyte injury, but has also been linked to renal-specificTMA.In hibit receptor tyrosine kinases (RTKs), all, we review the experimentally validated mechanisms by which VEGFA-VEGFR2 or inhibit downstream pathways. -

Antibody–Drug Conjugates
Published OnlineFirst April 12, 2019; DOI: 10.1158/1078-0432.CCR-19-0272 Review Clinical Cancer Research Antibody–Drug Conjugates: Future Directions in Clinical and Translational Strategies to Improve the Therapeutic Index Steven Coats1, Marna Williams1, Benjamin Kebble1, Rakesh Dixit1, Leo Tseng1, Nai-Shun Yao1, David A. Tice1, and Jean-Charles Soria1,2 Abstract Since the first approval of gemtuzumab ozogamicin nism of activity of the cytotoxic warhead. However, the (Mylotarg; Pfizer; CD33 targeted), two additional antibody– enthusiasm to develop ADCs has not been dampened; drug conjugates (ADC), brentuximab vedotin (Adcetris; Seat- approximately 80 ADCs are in clinical development in tle Genetics, Inc.; CD30 targeted) and inotuzumab ozogami- nearly 600 clinical trials, and 2 to 3 novel ADCs are likely cin (Besponsa; Pfizer; CD22 targeted), have been approved for to be approved within the next few years. While the hematologic cancers and 1 ADC, trastuzumab emtansine promise of a more targeted chemotherapy with less tox- (Kadcyla; Genentech; HER2 targeted), has been approved to icity has not yet been realized with ADCs, improvements treat breast cancer. Despite a clear clinical benefit being dem- in technology combined with a wealth of clinical data are onstrated for all 4 approved ADCs, the toxicity profiles are helping to shape the future development of ADCs. In this comparable with those of standard-of-care chemotherapeu- review, we discuss the clinical and translational strategies tics, with dose-limiting toxicities associated with the mecha- associated with improving the therapeutic index for ADCs. Introduction in antibody, linker, and warhead technologies in significant depth (2, 3, 8, 9). Antibody–drug conjugates (ADC) were initially designed to leverage the exquisite specificity of antibodies to deliver targeted potent chemotherapeutic agents with the intention of improving Overview of ADCs in Clinical Development the therapeutic index (the ratio between the toxic dose and the Four ADCs have been approved over the last 20 years (Fig. -

Oregon Medicaid Pharmaceutical Services Prior Authorization Criteria
Oregon Medicaid Pharmaceutical Services Prior Authorization Criteria HEALTH SYSTEMS DIVISION Prior authorization (PA) criteria for fee-for-service prescriptions for Oregon Health Plan clients March 1, 2021 Contents Contents ................................................................................................................................................................ 2 Introduction........................................................................................................................................................... 7 About this guide ......................................................................................................................................... 7 How to use this guide ................................................................................................................................. 7 Administrative rules and supplemental information .................................................................................. 7 Update information............................................................................................................................................... 8 Effective March 1, 2021 ............................................................................................................................ 8 Substantive updates and new criteria ............................................................................................. 8 Clerical changes ............................................................................................................................