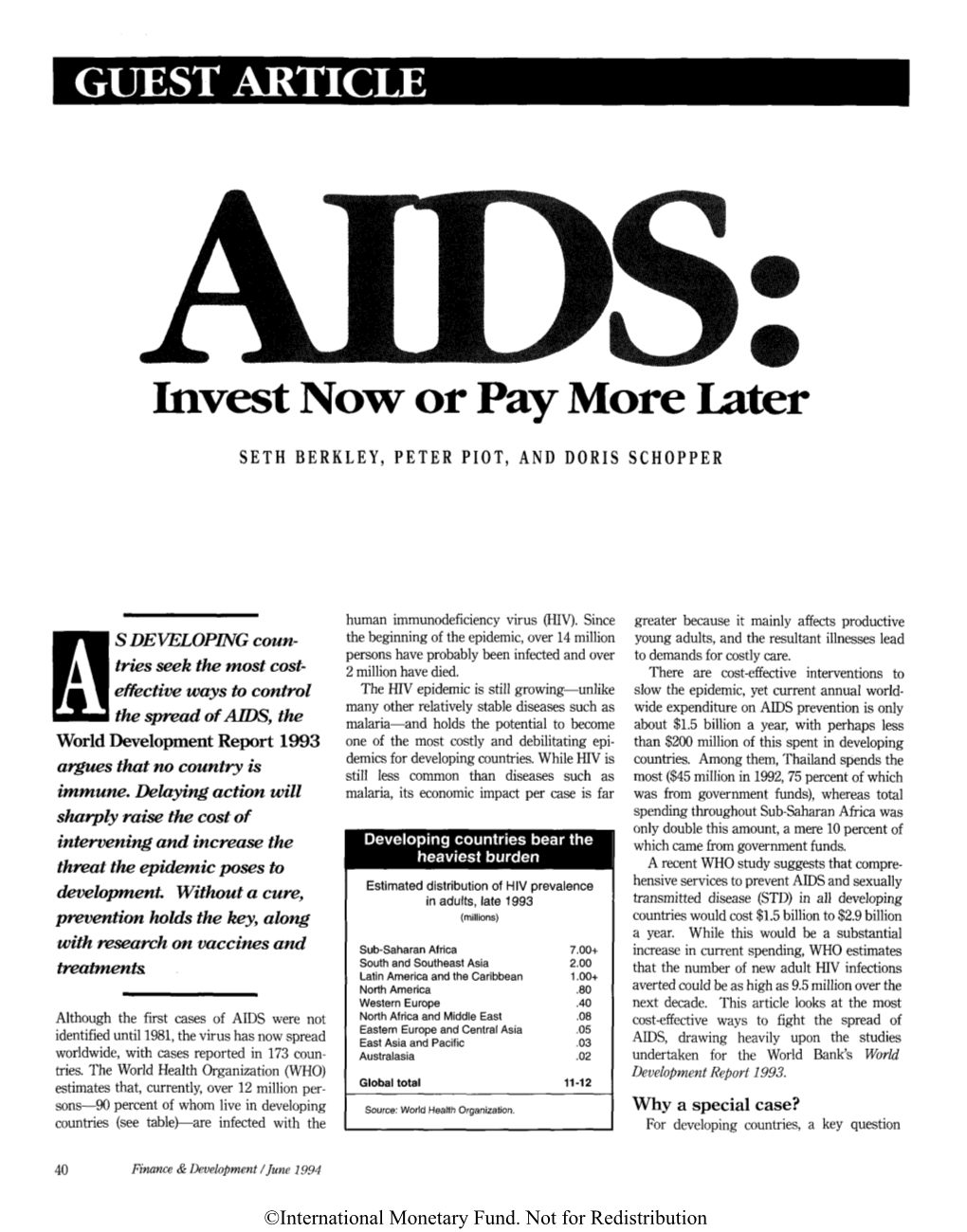
AIDS: Invest Now Or Pay More Later
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
KDHE News Release
News Room - 2012 - News Release A to Z Topic Listing KDHE News Release For Immediate Release KDHE Office of Communications January 3, 2012 [email protected], 785-296-0461 KDHE Promotes Cancer Screenings and HPV Vaccination During Cervical Health Awareness Month TOPEKA – In recognition of Cervical Health Awareness Month, the Kansas Department of Health and Environment (KDHE) encourages women to schedule their annual well-woman checkups. According to a 2010 Kansas Behavioral Risk Factor Surveillance System (BRFSS) report, approximately 17 percent of Kansas women aged 18 and older did not have a Pap test within the past three years. "Pap tests decrease the risk of developing cervical cancer by detecting precancerous cells which, when found early, are highly treatable," said Robert Moser, M.D., KDHE Secretary and State Health Officer. “Women should have their first screening Pap test at age 21, or within three years of becoming sexually active if younger." Although cervical cancer was once the leading cancer killer of women, the number of cases has declined 75 percent in the past 50 years, largely because of the widely available and reliable Pap test. Even so, an estimated 12,000 women in the United States are diagnosed with cervical cancer each year. In 2007, 4,021 women died from cervical cancer in the United States. In 2008, 76 Kansas cases were diagnosed, with 24 deaths due to cervical cancer in 2010. Most cervical cancer cases are caused by infection with human papillomavirus (HPV), a common sexually transmitted disease. HPV infection can also cause a number of other health problems for both men and women. -

CV Seth Berkly2.Indd
Dr Seth Berkley Chief Executive Officer of the GAVI Alliance As a physician, epidemiologist and leading advocate for vaccines and immunisation, Dr Seth Berkley brings many years of experience and knowledge from the fields of public health, development and vaccines to the work of the Alliance. Seth joined the GAVI Alliance in August 2011 as it launched its five year strategy to immunise a quarter of a billion children in the developing world with life-saving vaccines by 2015. “I am impressed by GAVI’s life-saving work and have great admiration for its successful track record,” said Dr Berkley. “I am therefore honoured and excited to have been chosen to lead the GAVI Alliance as it works to deliver on an ambitious new strategy.” Prior to joining the GAVI Alliance, Seth was the founder, president and CEO for 15 years of the International AIDS Vaccine Initiative ( IAVI ), the first vaccine product development public-private sector partnership. Under his leadership, IAVI implemented a global advocacy programme that assured that vaccines received prominent attention in the media and in political forums such as the G 8, EU and the UN. He also oversaw the creation of a virtual vaccine product development effort involving industry, academia, and developing country scientists. Prior to founding IAVI, Seth served as associate director in the Health Sciences Division at The Rockefeller Foundation. He has also worked for the Center for Infectious Diseases of the U. S. Centers for Disease Control and Prevention ( CDC ), the Massachusetts Department of Public Health and for the Carter Center where he served as an epidemiologist at the Ministry of Health in Uganda. -

Fall 2011 MEDICINE
BROWN Volume 17 | Number 3 | Fall 2011 MEDICINE Gentleman Scholar Calm, cool, connected, Griffin Rodgers pushes for research that will serve the people. PS:l U PRIMARY CARE REIMAGINED MAKING BABIES c1BrMed_Spring11rev.indd 1 9/29/11 1:53 PM Letter from the dean Start of One Era, End of Another The opening of the new Medical School in Providence’s old Jewelry District on August 15 marked one of the most important mile- stones in our history. Now our students have a state-of-the-art, spacious, and absolutely stunning home to call their own. This his- toric, creatively restored building off Col- lege Hill is close to several of our major teaching hospitals and the Public Health Program. Furthermore, it symbolizes Brown’s commitment to the city and the state to educate the next generation of physicians for all of us. Reunion and Commencement were carried out with beautiful weather and our usual traditions. Alumnus Griffin P. Rodgers, director of the National Institute of Diabetes and Digestive and Kidney Diseases—one of the National Institutes of Health—gave an inspiring commencement speech to our graduating class and is featured in this issue. He emphasized the excitement of research in human biology in this era of genomics, proteomics, and systems biology. Advances over the next decades will be spectacular and will change the way we care for patients. Since the earliest classes, the Medical School’s graduates have enhanced the lives of their patients as well as their communities. Some, such as Dr. Rodgers, have gone on to national careers. -

Inaugural Keynote Lecture: Contributions of Gavi and DCVMN to the Global Vaccine Markets
Inaugural Keynote Lecture: Contributions of Gavi and DCVMN to the global vaccine markets DCVMN 18th AGM Seth Berkley M.D, CEO 26 September 2017, Seoul www.gavi.org Gavi’s mission, model and 1 achievements to date Gavi’s mission Saving by increasing and protecting in lower-income children’s equitable use of people’s health countries lives vaccines DCVMN 18th AGM 26 September 2017 Gavi’s partnership model IMPLEMENTING COUNTRY DONOR COUNTRY GOVERNMENTS GOVERNMENTS CIVIL SOCIETY RESEARCH & ORGANISATIONS TECHNICAL AGENCIES VACCINE PRIVATE MANUFACTURERS SECTOR PARTNERS DCVMN 18th AGM 26 September 2017 Increasing immunisation coverage Launch of Gavi Post-Gavi 20% increase points 2000-2016 1980 1985 1990 1995 2000 2005 2010 2016 2020 Expanded Programme Stall in immunisation Support from Gavi to world’s on Immunization takes off coverage lowest-income countries * Based on data officially reported to WHO and UNICEF by current member states. Note: Includes DTP-containing vaccines, such as pentavalent vaccine. th Source: WHO/UNICEF Estimates of National Immunization Coverage, 2017 DCVMN 18 AGM 26 September 2017 Accelerating access to new vaccines in poorest countries Prior to Gavi support Now High-income countries Low-income countries High-income countries Low-income countries 100% 100% 100% 91% 86% 86% 77% 72% Hepatitis B 67% Hib Pneumococcal % of countries introduced vaccines nationally 3% 6% 6% 2000 2009 2000 2009 2016 Note: Only countries with universal national introduction are included. World Bank 2016 country classification has been applied to the whole time series. DCVMN 18th AGM Source: The International Vaccine Access Center (IVAC) VIMS database. Data as of 31 December 2016. -

Seth Berkley MD
Seth Berkley M.D. Chief Executive Officer of the GAVI Alliance Seth Berkley joined the GAVI Alliance as CEO in August 2011, as it launched its five year strategy to immunise a quarter of a billion children in the developing world with life-saving vaccines by 2015. Prior to joining the GAVI Alliance, Seth was the founder, president and CEO for 15 years of the International AIDS Vaccine Initiative ( IAVI ), the first vaccine product development public-private sector partnership. Under his leadership, IAVI implemented a global advocacy programme that assured that vaccines received prominent attention in the media and in forums such as the G 8, EU and the UN. He also oversaw the creation of a virtual vaccine product development effort involving industry, academia, and developing country scientists. Prior to founding IAVI, Seth served as associate director in the Health Sciences Division at The Rockefeller Foundation. He has also worked for the Center for Infectious Diseases of the U. S. Centers for Disease Control and Prevention ( CDC ), the Massachusetts Department of Public Health and for the Carter Center where he served as an epidemiologist at the Ministry of Health in Uganda. He has consulted or worked in more than 25 countries in Asia, Africa and Latin America. Seth sits on a number of international steering committees and corporate and not-for-profit boards, including those of Gilead Sciences, the New York Academy of Sciences and the Acumen Fund. In the past, he has also served on the boards of public and private vaccine companies such as PowderJect and VaxInnate and health and development organisations such as OXFAM America. -

COVID-19 Vaccine Development, Strategy and Implementation
Symposium: Vaccines and Global Health: COVID-19 Vaccine Development, Strategy and Implementation The Program in Vaccine Education at the Columbia University Vagelos College of Physicians & Surgeons’ mission is to educate medical students and to inform health care professionals, public health experts, academic, government and industry researchers, policy makers, global health non-governmental organizations, journalists, and the general public as to the cutting-edge advances and challenges in modern vaccine development. The Columbia University convenors are Drs. Lawrence Stanberry (Co-Director, PVE), Philip LaRussa (Co-Director, PVE), Wilmot James (Associate Director, PVE), and Marc Grodman (Special Advisor, PVE). We have put together a group of 25 outstanding speakers who have been intimately involved with all aspects of COVID-19 vaccine development, strategy, and implementation. We are delighted to present this five-day virtual symposium at the cusp of the world’s transition to controlling the COVID-19 pandemic. Monday, February 22 National, Regional and Global Response to an Unprecedented Challenge 12:00-12:10 Welcome: Lee Bollinger, JD – President, Columbia University 12:10-12:15 Moderator: Lawrence R. Stanberry, MD, PhD – Director of the Programs in Global Health, Columbia University Vagelos College of Physicians and Surgeons 12:15-12:45 Keynote: Sir Jeremy Farrar, BSc, MBBS, PhD – Director, Wellcome Trust The Role of the Wellcome Trust in COVID-19 Vaccine Preparedness 12:45-1:30 Speakers: - Shabir Madhi, MBChB, MMed, FCPaeds PhD – Professor of Vaccinology, University of the Witwatersrand – A South African perspective on vaccine preparedness and availability. - Nancy Messonnier, MD – Director, National Center for Immunization and Respiratory Diseases, US CDC – A US CDC perspective on vaccine preparedness and availability. -
2021 GTFCC World Health Assembly Side Event 20 May 2021 Biographies: Speakers and Moderators
2021 GTFCC World Health Assembly Side Event 20 May 2021 Biographies: Speakers and Moderators 1 Biographies: Table of Contents Dr. Tedros Adhanom Ghebreyesus..................................................................................... 3 Dr. Frew Benson ............................................................................................................... 4 Dr. Seth Berkley ............................................................................................................... 5 Dr. Christopher R. Braden.................................................................................................. 6 Dr. Godfrey Bwire ............................................................................................................. 7 Mr. Emanuele Capobianco ................................................................................................ 8 Ms. Simone Carter ............................................................................................................ 9 Mr. Wiseman Chimwaza ................................................................................................. 10 Ms. Pamela Mwelala Chisanga ....................................................................................... 11 Dr. Marc Gastellu-Etchegorry .......................................................................................... 12 Christine Marie George, PhD ........................................................................................... 13 Dr. Myriam Henkens ...................................................................................................... -

An Injection of Trust
VACCINES OUTLOOK in the United States alone1. Since the 1980s, every US state has required a standard bat- tery of vaccines for school enrolment. There is strong participation too in much of West- ern Europe, where these vaccines are merely ‘recommended’. “The vast majority of children are immunized, with coverage of over 90% MARMADUKE ST. JOHN/ALAMY MARMADUKE ST. across Europe,” says Pier Luigi Lopalco, head of the vaccine-preventable diseases programme at the European Centre for Disease Prevention and Control (ECDC) in Stockholm. When Australia faced falling vaccination rates in the 1990s it introduced incentives that rewarded both clinics and parents. “Our immunization rates rose by at least 10%, which was a major increase,” says Julie Leask, a social scientist Health-care workers in New York protest against compulsory swine flu vaccination. specializing in immunization policy at the University of Sydney. PUBLIC HEALTH But some vaccination programmes allow people to refuse for personal reasons. In much of Europe, no medical consultation is required. In the United States, parents must actively An injection register their refusal; 48 states recognize reli- gious exemptions and 18 allow ‘personal belief exemptions’. The refusal numbers are low — just 2% for 2010–2011, according to the CDC of trust — but epidemiologist Saad Omer of Emory University in Atlanta, Georgia, has observed a disconcerting rise. “The rate of refusal has Faced with outbreaks of preventable diseases, public-health gone up, and even the rate of change compared experts need to win over parents who refuse vaccinations. to previous years has accelerated,” he says. Indeed, CDC data indicate that the percent- age of non-medical exemptions essentially BY MICHAEL EISENSTEIN 5,442 in just the first 4 months of 2013. -

NEWSLETTER: FEBRUARY 28, 2020 Scaling up Community of Practice
NUMBER 16 NEWSLETTER: FEBRUARY 28, 2020 Scaling Up Community of Practice Dear Colleagues, We are pleased to share with you Newsletter #16 of the Scaling Up Community of Practice (CoP). In this Newsletter we report on the recent meeting of the Executive Committee (ExCom) of the CoP, including the decision to go ahead with the establishment of a new Working Group on Climate Change and Environment. We thank the members of the ExCom for their engagement. As usual, this Newsletter also (a) summarizes recent activity of our eight existing working groups; (b) presents updates that members have submitted on their scaling activities, (c) provides references to publications and other relevant items that have come across our desks, and (d) includes some special blog-length features reporting on lessons from scaling experience. Finally, as a new segment, we dug into our “archive” of early contributions to the scaling literature. We are very grateful to all of you who have responded to our request for inputs. We are also making progress on launching a dedicated CoP website that includes a consolidated schedule of CoP and Working Group meetings along with interactive pages for each of the Working Groups, an inventory of newsletters and other relevant resources, and an associated social media platform for more informal exchanges among CoP members. We expect to announce the launch in our next newsletter. Finally, we want to remind you that we plan for our next two-day, in-person workshop for the CoP participants on October 23-24, 2020 in the Washington Metropolitan Area. Invitations will be sent to you all in June 2020. -

Kno Wledg E Su M Mary: 'S & '
25 INTEGRATING IMMUNIZATION AND OTHER KNOWLEDGE SUMMARY KNOWLEDGE SERVICES FOR WOMEN AND CHILDREN : WOMEN he Expanded Programme on Immunizations (EPI) has dramatically decreased childhood T morbidity and mortality since its introduction in 1974, and now reaches over 85% of the world’s children. Some countries and regions are still working to achieve high coverage, ’ however, and many non-vaccine programmes have not gained the same traction needed for S maximum impact. Integrating service delivery, by providing a range of non-vaccine health & interventions to families at the same time as an immunization visit, can create a programme CHILDREN foundation through which broad services can be equitably provided as well as give a beneficial boost to EPI coverage. While integration requires thoughtful and measured planning, the potential impact for families and communities is great. ’ S HEALTH 2013 Photo: WHO / Christopher Black he Expanded Programme on Immunization (EPI) was DTP3 vaccine coverage, which has been a traditional 4 T established in 1974 to provide life-saving vaccines to the measurement of a countries’ health system capacity . world’s children. EPI now reaches more than 4 out of 5 of In the mid-1990s, the WHO and UNICEF created the guideline the world’s children and, with its strong delivery platform, for Integrated Management of Childhood Illnesses (IMCI), is becoming a sustained foundation for broader health interventions1, 2. The list of recommended vaccines has grown, recognizing the need to address the whole child, and the 5 and since 2000 the GAVI Alliance has helped low- and middle- continuum of care, in combating childhood illness . -

High Level Meeting of the Global Polio Partners Group (PPG)
Global Polio Partners Group High Level Meeting of the Global Polio Partners Group (PPG) Wednesday, 10 April 2013 09:00 – 13:00 Canadian Mission, 5 avenue de l’Ariana Geneva, Switzerland REPORT Summary The spring High Level PPG meeting (HLM) was attended by approximately 75 representatives from a large number of missions to the United Nations and other representatives of GPEI partners and stakeholders. In keeping with recent HLM practice to feature a high-level speaker, Dr Seth Berkley, CEO of the GAVI Alliance, was the key note speaker and focused on the necessary collaboration between GAVI and the Global Polio Eradication Initiative (GPEI) in efforts to eradicate polio and to sustain the gains by strengthening routine immunization. PPG members were provided with a briefing on the current polio situation and contingency planning to address insecurity situations in the three remaining endemic countries; the engagement of Islamic Scholars and leaders; and a preview of World Health Assembly discussions of polio in May 2013, including on the 2013-2018 Polio Eradication and Endgame Strategic Plan. Participants discussed the funding of the polio program and resource mobilization for 2013- 2018, including the April 24-25 Vaccine Summit in Abu Dhabi and an outline of the current thinking on the legacy of the program. Overview of Remarks Ambassador Elissa Golberg of Canada, PPG Co-Chair, welcomed the group noting the breadth of missions and organizations present and provided an outline of the program for the meeting before proceeding to the approval of the agenda. Continuing the tradition of having a high level speaker with whom polio partners can engage in a substantive dialogue, Dr Seth Berkley, CEO of the GAVIl Alliance, addressed the Polio Partners Group, speaking to the renewed urgency to strengthening routine immunization and the importance of GPEI and GAVI collaboration to achieve the goal of polio eradication. -
2004 Annual Progress Report
IAVI’S WORLDWIDE PARTNERS AND PROGRAMS Countries where IAVI has Governments that are Countries in which IAVI has scientific collaborators financial donors to IAVI advocacy or policy programs Belgium Rwanda Canada Belgium Netherlands Canada South Africa Denmark Brazil Norway China Sweden European Union Canada Rwanda Finland Switzerland Ireland Denmark South Africa France Uganda Netherlands Finland Spain Germany UK Norway France Sweden India US Sweden Germany Switzerland Kenya Zambia UK India Uganda Netherlands US Ireland UK Japan US Kenya Front Cover: (Left) Lab technician Moses Kwizera working on samples from a feasibility site at the MRC/IAVI laboratory in Masaka (Photo IAVI). (Middle) IAVI President and CEO Dr. Seth Berkley meets with Indian Prime Minister Dr. Manmohan Singh in New Delhi on 7 December, 2004. (Photo India Prime Minister’s office). (Right) Part-Time Study Physician Dr. Immaculee Mukatete (left) and Study Nurse Kephas Kafwimbi (right) joined other participants at a GCP (Good Clinical Practices) training workshop hosted by IAVI in Entebbe, Uganda in November (Photo Vanessa Vick/IAVI). Back Cover: (Left) HIV rapid testing at an IAVI vaccine research site in Kigali, Rwanda (Photo IAVI). (Middle) An HIV voluntary counseling and testing (VCT) session at the CGMRC center in Kilifi, Kenya (Photo IAVI). (Right) Fred Oyugi, Quality Control Manager for the Kenya AIDS Vaccine Initiative at an IAVI-sponsored GCP training workshop in Entebbe (Photo Vanessa Vick/IAVI). IAVI 2004 Annual Progress Report TABLE OF CONTENTS President’s Note Executive Summary of 2004 Activities and Key Milestones............................................................... i Detailed 2004 Annual Progress Report...................................................................................... 1 Introduction................................................................................................................ 1 IAVI 2005-2007 Strategic Plan.....................................................................................