Buckinghamshire Sexual Health Needs Assessment
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Silverstone 11-14 July
Official Formula 1™ Media Kit Formula 1 Rolex British Grand Prix 2019 Silverstone 11-14 July Silverstone Circuit Silverstone Circuit, Northamptonshire NN12 8TN United Kingdom OC E T Tel: 0844 3728 200 www.silverstone.co.uk © 2019 Formula One World Championship Limited, a Formula 1 company. The F1 FORMULA 1 logo, F1 logo, FORMULA 1, F1, FIA FORMULA ONE WORLD CHAMPIONSHIP, GRAND PRIX, BRITISH GRAND PRIX and related marks are trade marks of Formula One Licensing BV, a Formula 1 company. All rights reserved. The FIA logo is a trade mark of Federation Internationale de l’Automobile. All rights reserved. The F1 logo, FORMULA 1, F1, FIASI FORMULA ONEL WORLDVERSTONE CHAMPIONSHIP, BRITISH GRAND PRIX and 1 related marks are trade marks of Formula One Licensing BV, a Formula 1 company. All rights reserved THURSDAY 11 - SUNDAY 14 JULY 2019 Official Formula 1™ Media Kit Formula 1 Rolex ritish Grand rix 2019 Silverstone 11-14 uly CONTENTS General Information Timetable 04 Silverstone Information Media Contacts 08 Useful Media information 09 Opening hours of media facilities 09 Accreditation Centre and Media Locations map 10 Red Zone Map 11 Pit Garage Allocation 12 Silverstone Circuit Facts 13 FIA Formula 1 World Championship & British Grand Prix 2019 Race Winners 14 Results of 2019 Races 15 Drivers’ Championship Standings (after Austrian GP) 24 Constructors’ Championship Standings (after Austrian GP) 25 FIA Formula 1 World Champions 1950 - 2018 26 British Grand Prix Winners 1950-2018 27 The British Racing Drivers’ Club 29 Silverstone Landmarks 1948 - 2018 30 Silverstone Circuit Silverstone Circuit, Northamptonshire NN12 8TN United Kingdom Tel: 0844 3728 200 www.silverstone.co.uk The F1 logo, FORMULA 1, F1, FIA FORMULA ONE WORLD CHAMPIONSHIP, BRITISH GRAND PRIX and 2 related marks are trade marks of Formula One Licensing BV, a Formula 1 company. -

Aylesbury Vale WCS Granborough CP
Aylesbury Vale District Granborough CP Aylesbury Vale District Parish Boundaries Development Sites Winslow Proposed Development Sites Surface Water WFD Surface Water Classifications High Good Moderate Poor Swanbourne CP Bad Groundwater Superficial Aquifers Secondary (undifferentiated) Secondary A Unproductive Granborough CP Bedrock Aquifers Principal Secondary (undifferentiated) Secondary A Secondary B Unproductive Source Protection Zones Zone 1 - Inner Protection Zone Zone 2 - Outer Protection Zone Zone 3 - Total Catchment Aylesbury Vale WCS Water Constraints Oving CP and Opportunities 0 0.2 0.4 0.8 Km Contains Ordnance Survey data (c) Crown copyright and database right 2016 Aylesbury Vale District Great Horwood CP Aylesbury Vale District Nash CP Parish Boundaries Development Sites Whaddon CP Proposed Development Sites Surface Water WFD Surface Water Classifications High Good Moderate Poor Bad Groundwater Superficial Aquifers Secondary (undifferentiated) Great Horwood CP Secondary A Unproductive Adstock CP Bedrock Aquifers Principal Little Horwood CP Secondary (undifferentiated) Secondary A Secondary B Unproductive Source Protection Zones Zone 1 - Inner Protection Zone Zone 2 - Outer Protection Zone Zone 3 - Total Catchment Aylesbury Vale WCS Water Constraints Swanbourne CP and Opportunities Winslow 0 0.3 0.6 1.2 Km Contains Ordnance Survey data (c) Crown copyright and database right 2016 Aylesbury Vale District Grendon Underwood CP Steeple Claydon CP Aylesbury Vale District Parish Boundaries Development Sites Proposed Development Sites -

Aylesbury Vale Community Chest Grants April 2014 - March 2015
Aylesbury Vale Community Chest Grants April 2014 - March 2015 Amount Granted Total Cost Award Aylesbury Vale Ward Name of Organisation £ £ Date Purpose Area Buckinghamshire County Local Areas Artfully Reliable Theatre Society 1,000 1,039 Sep-14 Keyboard for rehearsals and performances Aston Clinton Wendover Aylesbury & District Table Tennis League 900 2,012 Sep-14 Wall coverings and additional tables Quarrendon Greater Aylesbury Aylesbury Astronomical Society 900 3,264 Aug-14 new telescope mount to enable more community open events and astrophotography Waddesdon Waddesdon/Haddenham Aylesbury Youth Action 900 2,153 Jul-14 Vtrek - youth volunteering from Buckingham to Aylesbury, August 2014 Vale West Buckingham/Waddesdon Bearbrook Running Club 900 1,015 Mar-15 Training and raceday equipment Mandeville & Elm Farm Greater Aylesbury Bierton with Broughton Parish Council 850 1,411 Aug-14 New goalposts and goal mouth repairs Bierton Greater Aylesbury Brill Memorial Hall 1,000 6,000 Aug-14 New internal and external doors to improve insulation, fire safety and security Brill Haddenham and Long Crendon Buckingham and District Mencap 900 2,700 Feb-15 Social evenings and trip to Buckingham Town Pantomime Luffield Abbey Buckingham Buckingham Town Cricket Club 900 1,000 Feb-15 Cricket equipment for junior section Buckingham South Buckingham Buckland and Aston Clinton Cricket Club 700 764 Jun-14 Replacement netting for existing practice net frames Aston Clinton Wendover Bucks Play Association 955 6,500 Apr-14 Under 5s area at Play in The Park event -
![Training and Enterprise Councils [Appendix I Revised 1 August 1997]](https://docslib.b-cdn.net/cover/1842/training-and-enterprise-councils-appendix-i-revised-1-august-1997-471842.webp)
Training and Enterprise Councils [Appendix I Revised 1 August 1997]
Training and Enterprise Councils Research Paper 97/48 7 May 1997 [Appendix I revised 1 August 1997] Between the Spring of 1990 and the Autumn of 1991, responsibility for the administration of most Government training and enterprise programmes was transferred from the Department of Employment to a new network of 82 (now 79) Training and Enterprise Councils (TECs) in England and Wales and 22 Local Enterprise Companies (LECs) in Scotland. This Research Paper gives a brief account of the reasons for this change and some details of the composition, functions, funding and mechanics of TECs. It concentrates on TECs rather than LECs, although much of what is said about TECs applies equally to LECs. To help Members who may need to approach their local TEC, Appendix 1 lists all Parliamentary constituencies with the name of the TEC or LEC operating in their area. This has been compiled by Susan Kielty. Appendix 2 gives the address and telephone numbers of the TECs. Appendix 3 lists the LECs in Scotland. This Paper replaces Research Note 92/21, "Training and Enterprise Councils", which has been updated with the help of Jeremy Gyepi-Garbrah. Julia Lourie Business and Transport Section House of Commons Library Library Research Papers are compiled for the benefit of Members of Parliament and their personal staff. Authors are available to discuss the contents of these papers with Members and their staff but cannot advise members of the general public. CONTENTS Page Summary 5 I Background 7 A. TEC Mergers 10 B. TEC National Council 12 II Status and Composition 12 A. -

Aylesbury Vale Housing and Economic Land Availability Assessment (HELAA) Report V4 –To Inform VALP Proposed Submission Plan
AYLESBURY VALE DISTRICT COUNCIL Aylesbury Vale Housing and Economic Land Availability Assessment (HELAA) Report v4 –To inform VALP Proposed Submission Plan Report January 2017 HELAA version 4 – Erratum 13.03.2017 Page 17 Corrected Table 4 – Economic Development over 500sqm outside HELAA settlements (corrections – additions or amendments in Bold) Site Monitoring Planning Floorspace - area Ref Parish Address application sqm (net) (ha) Kingspan Environmental Ltd, College Road North, Aston 026i0119 ASTON CLINTON Clinton app/0319/16 587 0.07 030i0029 BIDDLESDEN Partnership Poultry Farm, Whitfield Road, Biddlesden app/1965/15 903 0.09 049i0010 EDGCOTT Faccenda Chicken Ltd, Marsh Gibbon Road, Edgcott app/0012/16 602 0.06 059i0032 HALTON Land at Wendover Woods, Chivery, Halton App/0344/13 535 6.18 Green Dragon Rare Breeds Farm & Eco Centre, Claydon 063i0016 HOGSHAW Road, Hogshaw app/1744/15 752 2.56 071i0022 Silverstone Motor Racing Circuit and Silverstone Park, 071i0008 LILLINGSTONE DAYRELL Silverstone Road aop/01785/11 191,775 184 076i0013 LUDGERSHALL Kings Farm, Piddington Road, Ludgershall app/0690/15 570 0.09 110i0046 TINGEWICK land adj Barton Road, Tingewick app/1122/16 2,665 0.93 115i0008 WATER STRATFORD Scirese Farm, Brackley Road, Water Stratford couaf/2422/14 545 0.05 119i0051 WESTCOTT Westcott Venture Park, High Street, Westcott app/0073/16 2,290 0.23 119i0052 WESTCOTT Westcott Venture Park, High Street, Westcott app/1116/16 651 0.04 119i0046 WESTCOTT Westcott Venture Park, Bicester Road, Westcott app/0869/14 4,180 1.35 Plot 1070, Westcott -

Directory of Organisations Supporting Older People in Areas Around Buckingham¹
Directory of organisations supporting older people in areas around Buckingham¹ Haddenham² and Winslow³ ¹ Addington, Adstock, Akeley, Barton Hartshorn, Beachampton, Biddlesden, Buckingham, Calvert, Charndon, Chetwode, East Claydon, Foscott, Gawcott with Lenborough, Hillesden, Hogshaw, Leckhampstead, Lillingstone Dayrell with Luffield Abbey, Lillingstone Lovell, Maids Moreton, Middle Claydon, Nash, Padbury, Poundon, Preston Bissett, Radclive-cum-Chackmore, Shalstone, Steeple Claydon, Stowe, Thornborough, Thornton, Tingewick, Turweston, Twyford, Water Stratford, Westbury and Whaddon. ² Aston Sandford, Boarstall, Brill, Chearsley, Chilton, Cuddington, Dinton-with-Ford and Upton, Haddenham, Ickford, Kingsey, Long Crendon, Oakley, Shabbington, Stone with Bishopstone and Hartwell, and Worminghall ³ Creslow, Dunton, Granborough , Great Horwood , Hardwick, Hoggeston, Little Horwood , Mursley, Newton Longville , North Marston , Oving , Pitchcott, Swanbourne, Whitchurch and Winslow This pack is produced as part of the Building Community Capacity Project by AVDC’s Lynne Maddocks. Contact on 01296 585364 or [email protected] for more information. July 2013 Index All groups are listed alphabetically according to organisation name. This list is not a fully comprehensive listing of older people’s services in these areas, but is designed to be a good starting point. Every effort has been made to ensure the accuracy of this information. It is up to date at the time of printing which is July 2013. Page No Organisation name 4 Abbeyfield (Haddenham) -

Haddenham to Aylesbury (Via Gibraltar and Ford)
Haddenham to Aylesbury (via Gibraltar and Ford) 1st walk check 2nd walk check 3rd walk check 26th October 2013 25th March 2016 18th August 2021 Current status Document last updated Thursday, 19th August 2021 This document and information herein are copyrighted to Saturday Walkers’ Club. If you are interested in printing or displaying any of this material, Saturday Walkers’ Club grants permission to use, copy, and distribute this document delivered from this World Wide Web server with the following conditions: • The document will not be edited or abridged, and the material will be produced exactly as it appears. Modification of the material or use of it for any other purpose is a violation of our copyright and other proprietary rights. • Reproduction of this document is for free distribution and will not be sold. • This permission is granted for a one-time distribution. • All copies, links, or pages of the documents must carry the following copyright notice and this permission notice: Saturday Walkers’ Club, Copyright © 2013-2021, used with permission. All rights reserved. www.walkingclub.org.uk This walk has been checked as noted above, however the publisher cannot accept responsibility for any problems encountered by readers. Haddenham to Aylesbury (via Gibraltar and Ford) Start: Haddenham & Thame Parkway station Finish: Aylesbury station Haddenham & Thame Parkway station, map reference SP 731 085, is 10 km south west of Aylesbury, 22km east of Oxford, and 81m above sea level. Aylesbury Station, map reference SP 817 134, is 78m above sea level. Both are in Buckinghamshire. Length: 23.4 km (14.6 mi), of which 5.8 km (3.6 mi) on roads or pavements. -

The Temple Memoirs
THE TEMPLE MEMOIRS eAn account of this Historic Family and its Demesnes; with 'Biographical Sletches, Anecdotes ~ Legends from Saxon Times to the present day; including a frontispiece in colours, thirty-four plates ~ two sheet pedigrees. By CoLONELJOHN ALEXANDER TEMPLE, vfuthor of ''Annals of Two extinct Families," ''Woo/ stone, a Cotswold Hamlet," assisted 6y HARALD MARKHAM TEMPLE H. F. ~ G. WITHERBY 3 2 6 High Hol/Jorn, London, 117. C. I 1925 Printed i11 Great Britain THE TEMPLE MEMOIRS QCARTERINGS OF SIR \\"ILLL\:\l TE.'.\IPLE, 5n1 B.\RO~ET, 1749-1760. 1 TEMPLE 10 WARSTE.\D 19 SCOC.\THE 2 GEDNEY. 11 S>.IITH 20 WAKESTED 3 WALKINGHAM 12 LEE 21 ARDERBOt:GIIE 4 EVERTOS 13 WILCOTTES 22 P.\RSC.\LL 5 SPE:SCER OF EVERTO:S 14 MOLLISS 23 BERWJCKE 6 SPENCER 15 HALL 24 SIJERSH.\LL 7 LEDESPEXCER 16 GREESE 25 PR.\TTEI.L 8 DEVERELL 17 GLANVILLE 9 LINCOLN 18 LYONS PREFACE Ta1s little History has been compiled in the belief that the time has now come to put on record a connected account of the fortunes and experiences of this ancient family, as it does not seem to have been hitherto attempted in detail by any writer. Its history is so intimately and closely bound up with that of England, politically and generally, during the sixteenth, seventeenth, eighteenth, nineteenth and twentieth centuries, that it is impossible to study the one without becoming acquainted and interested in the other, and now that the break up of their seats at Stowe and The Nash is, unfortunately, more or less complete, it seems a pity that no effort should be made to rescue from oblivion the many noteworthy facts and varied experiences of the distinguished men who have contributed to its history from time to time during past centuries, and to give details of the numerous estates, mansions, heirlooms, literary and artistic possessions that were acquired by them, and have, during the past two years, been scattered and dispersed under the hammer of the auctioneer. -
AVDC Sub Groups Local Lettings Policy
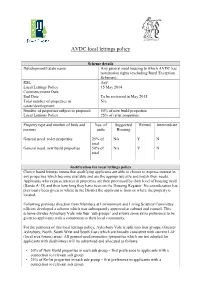
AVDC local lettings policy Scheme details Development/Estate name Any general need housing to which AVDC has nomination rights (excluding Rural Exception Schemes). RSL Any Local Lettings Policy – 15 May 2014 Commencement Date End Date To be reviewed in May 2015 Total number of properties in N/a estate/development Number of properties subject to proposed 50% of new build properties Local Lettings Policy 25% of re let properties Property type and number of beds and Nos. of Supported Rented Intermediate persons units Housing General need, re-let properties 25% of N/a Y N total General need, new build properties 50% of N/a Y N total Justification for local lettings policy Choice based lettings means that qualifying applicants are able to choose to express interest in any properties which become available and are the appropriate size and match their needs. Applicants who express interest in properties are then prioritised by their level of housing need (Bands A- D) and then how long they have been on the Housing Register. No consideration has previously been given to where in the District the applicant is from or where the property is located. Following previous direction from Members at Environment and Living Scrutiny Committee officers developed a scheme which was subsequently approved at cabinet and council. This scheme divides Aylesbury Vale into four ‘sub groups’ and allows some extra preference to be given to applicants with a connection to their local community. For the purposes of this local lettings policy, Aylesbury Vale is split into four groups, (Greater Aylesbury, North, South West and South East) which are broadly consistent with current LAF (local area forum) areas. -

Biddlesden Abbey and Its Lands. Rev. H. Roundell
BIDDLESDEN ABBEY AND ITS LANDS. BY REV. H. ROUNDELL. "Kings and princes became as fathers imto the Church, the hearts of all men inclined towards it, and there grew unto it every day earthly possessions in more and more abundance, till the greatness thereof bred envy, which no diminutions are able to satisfy.” Hooker. —Eccl. Pol., Bk. vii. ch. 21. Although no vestiges of Monastic buildings or of the Conventual and Parish Church can now be traced, and not a stone remains to mark the ancient boundaries of a Burial Ground, to which were once committed the bodies of munificent or noble benefactors, St. Mary's Abbey at Biddlesden, formerly occupied an important position among the Religious Houses of Buckinghamshire. In 1812 its Abbot was summoned to the Conference of Cistercian Monks in London, held under the Presidency of the Pope's Legate, and three years later with consent of his Convent, advanced a loan of 100l. to Edward the Second. The possessions of the Abbey, lying partly in Northamptonshire, and partly in Bucks, comprised lands or houses in twenty-one parishes, and at the last survey before the Dissolution of Religious Houses the revenues were returned of the annual value of 138/. 4s. 3d. It is stated in the Monasticon Anglicanum that in the Library at Stowe were preserved no fewer than eighty-one original documents of this Abbey, with seals appendant to most of them, commencing from the reign ojf King John, and among them a sentence of excommunication issued by the Pope against the Abbot and Monks in 1245. -

The Parliamentary Constituencies (England) (Miscellaneous Changes) Order 1990
Status: This is the original version (as it was originally made). This item of legislation is currently only available in its original format. STATUTORY INSTRUMENTS 1990 No. 1307 REPRESENTATION OF THE PEOPLE REDISTRIBUTION OF SEATS The Parliamentary Constituencies (England) (Miscellaneous Changes) Order 1990 Made - - - - 26th June 1990 Coming into force in accordance with article 1(2) At the Court of Saint James, the 26th day of June 1990 Present, The Counsellors of State in Council Whereas in pursuance of section 3(3) of the Parliamentary Constituencies Act 1986(1) the Boundary Commission for England have submitted to the Secretary of State a report dated 28th February 1990 with respect to the areas comprised in certain constituencies in England and showing the constituencies into which they recommend, in accordance with the Parliamentary Constituencies Act 1986, that the areas should be divided: And whereas the Secretary of State has laid that report before Parliament together with the draft of this Order in Council to give effect to the recommendations contained in the report and each House of Parliament has by resolution approved the said draft: And whereas Her Majesty, in pursuance of the Regency Acts 1937 to 1953, was pleased, by Letters Patent dated the 15th day of June 1990 to delegate to the six Counsellors of State therein named or any two or more of them full power and authority during the period of Her Majesty’s absence from the United Kingdom to summon and hold on Her Majesty’s behalf Her Privy Council and to signify thereat Her Majesty’s approval for anything for which Her Majesty’s approval in Council is required: Now, therefore, His Royal Highness the Prince Charles, Prince of Wales and His Royal Highness the Prince Edward, being authorised thereto by the said Letters Patent, and in pursuance of section 4 of the Parliamentary Constituencies Act 1986 and by and with the advice of Her Majesty’s Privy Council, do on Her Majesty’s behalf order, and it is hereby ordered, as follows: (1) 1986 c. -

Volume 3. 1705–1712
Buckinghamshire Sessions Records County of Buckingham CALENDER to the SESSIONS RECORDS VOLUME III. 1705 to 1712 AND APPENDIX, 1647 Edited by WILLIAM LE HARDY, M.C., F.S.A. GEOFFREY LI. RECKITT, M.C., F.S.A. AYLESBURY: Published by Guy R. Crouch, LL.B., Clerk of the Peace, County Hall. 1939 COMPILED UNDER THE DIRECTION OF THE STANDING JOINT COMMITTEE OF THE BUCKINGHAMSHIRE QUARTER SESSIONS AND COUNTY COUNCIL. [All Rights Reserved] Printed by HUNT, BARNARD & CO. LTD., AYLESBURY. CONTENTS PAGE Preface . vii-xxxxii Calendar to the Sessions Records, 1705 TO 1712 . 1-305 Appendix i, (a) Justices of the Peace, (B) Sheriffs, 1705 to 1712 306-308 Appendix ii, Document at Doddershall, 1647 . 309-316 Appendix III, Addenda to Volume II . 317-325 Appendix IV, Writs of venire facias and capias ad respondendum, 1705 to 1712 . 326-334 Appendix V, Register of Gamekeepers, 1707 to 1712. 335-345 Appendix VI, Steeple Claydon Highway Rate, 1710 . 346 Appendix VII, Dinton Poor Rate, 1711 . 347-349 Index . 350-427 PREFACE Those who believe that the value of a work of this nature lies in its completeness must suffer a disappointment in the fact that it is now nearly three years since the publication of the last volume of the calendar, and with those who hold such an opinion we have much sympathy and offer our apologies to them. This delay has been caused mainly by the discovery, during the preparation of the work, that many of the documents which go to make up a Sessions Roll had become misplaced. It was thus necessary to examine and arrange all the rolls for a period long after the date when this calendar was likely to end, in order to ensure that all records covering the period would be brought together and noted in the calendar.