Management of Urosepsis in 2018
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Forensic Medicine
YEREVAN STATE MEDICAL UNIVERSITY AFTER M. HERATSI DEPARTMENT OF Sh. Vardanyan K. Avagyan S. Hakobyan FORENSIC MEDICINE Handout for foreign students YEREVAN 2007 This handbook is adopted by the Methodical Council of Foreign Students of the University DEATH AND ITS CAUSES Thanatology deals with death in all its aspects. Death is of two types: (1) somatic, systemic or clinical, and (2) molecular or cellular. Somatic Death: It is the complete and irreversible stoppage of the circulation, respiration and brain functions, but there is no legal definition of death. THE MOMENT OF DEATH: Historically (medically and legally), the concept of death was that of "heart and respiration death", i.e. stoppage of spontaneous heart and breathing functions. Heart-lung bypass machines, mechanical respirators, and other devices, however have changed this medically in favor of a new concept "brain death", that is, irreversible loss of Cerebral function. Brain death is of three types: (1) Cortical or cerebral death with an intact brain stem. This produces a vegetative state in which respiration continues, but there is total loss of power of perception by the senses. This state of deep coma can be produced by cerebral hypoxia, toxic conditions or widespread brain injury. (2) Brain stem death, where the cerebrum may be intact, though cut off functionally by the stem lesion. The loss of the vital centers that control respiration, and of the ascending reticular activating system that sustains consciousness, cause the victim to be irreversibly comatose and incapable of spontaneous breathing. This can be produced by raised intracranial pressure, cerebral oedema, intracranial haemorrhage, etc.(3) Whole brain death (combination of 1 and 2). -

Coma Stimulation: Suggested Activities
Coma stimulation: suggested activities Headway’s publications are all available to freely download from the information library on the charity’s website, while individuals and families can request hard copies of the booklets via the helpline. As a charity, we rely on donations from people like you to continue providing free information to people affected by brain injury. Donate today: www.headway.org.uk/donate. Introduction It is quite common for family members to feel ‘useless’ when a relative is in a coma, and to be desperate to do something to help. A coma stimulation programme (sometimes called a coma arousal programme) is an approach based on stimulating the unconscious person’s senses of hearing, touch, smell, taste and vision individually in order to help their recovery. There is still controversy over how effective it is to try to stimulate a person in coma. However, most would say that such programmes have some beneficial effect, even if only to provide something constructive for the family to do. It is very important that the activities used would have been enjoyable for the patient before the injury. For example, only play music they like and talk to them about subjects they are interested in. Try not to do anything for too long in order to avoid tiring the person out. A stimulation programme must only be started after discussion with the clinical staff, who will advise you what might be appropriate at any particular stage in the recovery process. Activity suggestions Here are some examples of activities that could form part of a coma stimulation programme: • Make sure that a few friends and family members visit regularly, rather than in large groups at a time. -

CMS Manual System Human Services (DHHS) Pub
Department of Health & CMS Manual System Human Services (DHHS) Pub. 100-07 State Operations Centers for Medicare & Provider Certification Medicaid Services (CMS) Transmittal 8 Date: JUNE 28, 2005 NOTE: Transmittal 7, of the State Operations Manual, Pub. 100-07 dated June 27, 2005, has been rescinded and replaced with Transmittal 8, dated June 28, 2005. The word “wound” was misspelled in the Interpretive Guidance section. All other material in this instruction remains the same. SUBJECT: Revision of Appendix PP – Section 483.25(d) – Urinary Incontinence, Tags F315 and F316 I. SUMMARY OF CHANGES: Current Guidance to Surveyors is entirely replaced by the attached revision. The two tags are being combined as one, which will become F315. Tag F316 will be deleted. The regulatory text for both tags will be combined, followed by this revised guidance. NEW/REVISED MATERIAL - EFFECTIVE DATE*: June 28, 2005 IMPLEMENTATION DATE: June 28, 2005 Disclaimer for manual changes only: The revision date and transmittal number apply to the red italicized material only. Any other material was previously published and remains unchanged. However, if this revision contains a table of contents, you will receive the new/revised information only, and not the entire table of contents. II. CHANGES IN MANUAL INSTRUCTIONS: (N/A if manual not updated.) (R = REVISED, N = NEW, D = DELETED) – (Only One Per Row.) R/N/D CHAPTER/SECTION/SUBSECTION/TITLE R Appendix PP/Tag F315/Guidance to Surveyors – Urinary Incontinence D Appendix PP/Tag F316/Urinary Incontinence III. FUNDING: Medicare contractors shall implement these instructions within their current operating budgets. IV. ATTACHMENTS: Business Requirements x Manual Instruction Confidential Requirements One-Time Notification Recurring Update Notification *Unless otherwise specified, the effective date is the date of service. -

Urinary Tract Infection (Uti) Fact Sheet
URINARY TRACT INFECTION (UTI) FACT SHEET Overview A urinary tract infection (UTI) is an infection that involves any part of the urinary tract, including the kidneys, bladder and urethra. It is usually caused by exposure of the urinary tract to a fecal organism such as Escherichia coli (E. coli) but also may be caused by other organisms. An indwelling urinary catheter is a drainage tube that is inserted into the urinary bladder through the urethra, is left in place and is connected to a closed urine collection system. Urinary tract infections in patients with an indwelling urinary catheter are called catheter-associated UTIs, or CAUTIs. Signs and Symptoms Common symptoms of UTI include: • fever; • pain or burning in the lower abdomen; • burning during urination; • an increase in the frequency of urination; and • cloudy appearing urine. Causes and Transmission A UTI occurs when germs (usually bacteria) enter the urinary tract through the meatus (the opening of the urinary tract). These germs then cause infection. The urinary tract is normally sterile, meaning it contains no germs. A CAUTI occurs when germs (usually bacteria) enter the urinary tract through the urinary catheter and cause infection. This can occur when health care worker hands are not properly cleaned before the insertion of a catheter or during the process of cleaning or emptying of the urine collection system. Risk Factors Sexually active women, people with blockages in the urinary tract, such as prostate enlargement, and women using certain types of birth control, such as diaphragms, or those who are undergoing menopause are at higher risk of UTI. -

Evaluation and Management in an Urgent Care Setting
Syncope Evaluation and Management in an Urgent Care Setting Urgent message: When a patient presents to urgent care after a syncopal event, the clinician’s charge is to determine whether the episode was of benign or potentially life-threatening etiology and whether the patient should be transferred for further evaluation. Kenneth V. Iserson, MD, MBA, FACEP, FAAEM, Professor of Emergency Medicine, The University of Arizona, Tucson, AZ Introduction yncope is a sudden, transient loss of consciousness with a loss of postural tone (typically, falling). It results from an abrupt, transient, and diffuse cerebral Smalfunction and is quickly followed by sponta- neous recovery. The term syncope excludes seizures, coma, shock, or other states of altered consciousness. Many patients will ascribe their syncopal episode to a sit- uationally mediated vasovagal episode. Despite this, the goals in the urgent care setting include the following: Ⅲ Determining whether the patient’s episode was actually a syncopal or presyncopal event, and if it could have a life-threatening etiology Ⅲ Stabilizing the patient Ⅲ Transferring those patients who need further diag- nostic studies or therapeutic interventions © John Bolesky, Artville © John Bolesky, Epidemiology Syncope accounts for up to 3% of emergency depart- common in young adults, while cardiac syncope ment (ED) visits and up to 6% of hospital admissions becomes increasingly more frequent with advancing each year in the United States.1,2 At some time in their age.4 The chance of having at least one syncopal episode lives, up to about half the population (12% to 48%) of in childhood is between 15% and 50%.5 Though a people may experience syncope.3 benign cause is usually found, syncope in children war- Syncope occurs in all age groups, but it is most com- rants prompt detailed evaluation.6 mon in adults. -

233 the Use of Absorbent Pads Increases the Risk For
233 Omli R1, Skotnes L H1, Romild U1, Kuhry E1 1. Namsos Hospital THE USE OF ABSORBENT PADS INCREASES THE RISK FOR LOWER URINARY TRACT INFECTIONS IN NURSING HOMES RESIDENTS. Hypothesis / aims of study Urinary incontinence is a common medical problem in the nursing home population. The aim of this study was to determine whether use of absorbent pads is a risk factor for the development of lower urinary tract infections in nursing home residents. Introduction Lower urinary tract infections (UTIs) are a common medical problem in the elderly. Different kinds of absorbent products, such as diapers, pad and pant combinations, are used in incontinence care. In some cases, indwelling catheters, external condom catheters or in-and-out catheterisation are options for managing bladder dysfunction. About 23% of the residents in nursing homes don’t need toilet assistance. That means that the majority of residents is dependent on help from nursing staff for toileting and help to change soiled absorbent pads. Transmission of bacteria during incontinence care is associated with UTIs in elderly. In the vulnerable nursing home population, UTIs are a frequent problem and can lead to increased morbidity and even mortality. The prevalence of UTIs in nursing home residents is approximately 30%. Improving hand hygiene among staffing in nursing homes is one of the most important and effective methods to reduce hand born transmission of pathological microbes. Studies in long-term-care facilities document a lack of hand hygiene in connection to staff-resident interactions. This study studies the association between the use of absorbent pads and symptomatic UTIs in the nursing home population. -
Module 3: Benign Prostatic Hypertrophy
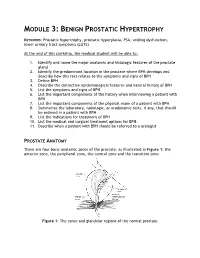
MODULE 3: BENIGN PROSTATIC HYPERTROPHY KEYWORDS: Prostatic hypertrophy, prostatic hyperplasia, PSA, voiding dysfunction, lower urinary tract symptoms (LUTS) At the end of this clerkship, the medical student will be able to: 1. Identify and name the major anatomic and histologic features of the prostate gland 2. Identify the predominant location in the prostate where BPH develops and describe how this fact relates to the symptoms and signs of BPH 3. Define BPH 4. Describe the distinctive epidemiological features and natural history of BPH 5. List the symptoms and signs of BPH 6. List the important components of the history when interviewing a patient with BPH 7. List the important components of the physical exam of a patient with BPH 8. Summarize the laboratory, radiologic, or urodynamic tests, if any, that should be ordered in a patient with BPH 9. List the indications for treatment of BPH 10. List the medical and surgical treatment options for BPH. 11. Describe when a patient with BPH should be referred to a urologist PROSTATE ANATOMY There are four basic anatomic zones of the prostate, as illustrated in Figure 1: the anterior zone, the peripheral zone, the central zone and the transition zone. Figure 1: The zones and glandular regions of the normal prostate. The anterior zone is entirely fibromuscular and non-glandular, and it appears to have little significance in prostatic function or pathology. This area comprises approximately 20% of the bulk of prostatic tissue. The peripheral zone is composed entirely of acinar tissue. It comprises the posterior surface of the prostate, including the apical, lateral, posterolateral and anterolateral portions of the prostate. -

Urinary Incontinence ! ! !What Is Urinary Incontinence? Leakage of Urine Is Called Urinary Incontinence
! ! ! Urinary Incontinence ! ! !What is urinary incontinence? Leakage of urine is called urinary incontinence. Some women leak small amounts of !urine. At other times, leakage of urine is frequent or severe. !Are there different types of urinary incontinence? !There are several types of urinary incontinence: • Stress urinary incontinence is loss of urine when a woman coughs, laughs, or sneezes. Leaks also can happen when a woman walks, runs, or exercises. It is caused by a weakening of the tissues that support the bladder or the muscles of the ! urethra. • Urge incontinence is leakage of urine caused by overactive bladder muscles that ! contract too often or problems with the nerves that send signals to the bladder !• Mixed incontinence is a combination of both stress and urge incontinence symptoms • Overflow incontinence is a steady loss of small amounts of urine when the bladder does not empty all the way during voiding. It can be caused by an underactive bladder ! muscle or blockage of the urethra. !What are the symptoms of urinary incontinence? !In addition to leaking urine, a woman with incontinence also may have other symptoms: • Urgency— A strong urge to urinate whether or not the bladder is full, often with pelvic ! pressure !• Frequency— Voiding more often than she considers usual !• Nocturia — The need to void during hours of sleep !• Dysuria — Painful voiding !• Enuresis— Bed-wetting or leaking while sleeping ! What causes urinary incontinence? ! Urinary incontience can have short-term causes and long-term causes. Short-term !causes are easier to treat and include the following: • Urinary tract infection— Loss of bladder control may be caused by an infection of the urinary tract. -

The Vegetative State: Guidance on Diagnosis and Management
n CLINICAL GUIDANCE The vegetative state: guidance on diagnosis and management A report of a working party of the Royal College of Physicians contrasts with sleep, a state of eye closure and motor Clin Med 1INTRODUCTION quiescence. There are degrees of wakefulness. 2003;3:249–54 Wakefulness is normally associated with conscious awareness, but the VS indicates that wakefulness and Background awareness can be dissociated. This can occur because 1.1 This guidance has been compiled to replace the brain systems controlling wakefulness, in the the recommendations published by the Royal College upper brainstem and thalamus, are largely distinct of Physicians in 1996, 1 in response to requests for from those which mediate awareness. 6 clarification from the Official Solicitor. The guidance applies primarily to adult patients and older children Awareness in whom it is possible to apply the criteria for diagnosis discussed below. 1.6 Awareness refers to the ability to have, and the having of, experience of any kind. We are typically aware of our surroundings and of bodily sensations, Wakefulness without awareness but the contents of awareness can also include our 1.2 Consciousness is an ambiguous term, encom- memories, thoughts, emotions and intentions. passing both wakefulness and awareness. This dis- Although understanding of the brain mechanisms of tinction is crucial to the concept of the vegetative awareness is incomplete, structures in the cerebral state, in which wakefulness recovers after brain hemispheres clearly play a key role. Awareness is not injury without recovery of awareness. 2–5 a single indivisible capacity: brain damage can selectively impair some aspects of awareness, leaving others intact. -

Factors Predicting Acute Brain Injury in Cases of Carbon Monoxide Poisoning: a Prospective Registry-Based Study
toxics Article Factors Predicting Acute Brain Injury in Cases of Carbon Monoxide Poisoning: A Prospective Registry-Based Study Hoon Lim 1,†, Young Hwan Lee 1,†, Sangun Nah 1 , Sungwoo Choi 1 , Young Soon Cho 1, Gi Woon Kim 1, Ji Eun Moon 2 and Sangsoo Han 1,* 1 Department of Emergency Medicine, Soonchunhyang University Bucheon Hospital, Bucheon 14584, Korea; [email protected] (H.L.); [email protected] (Y.H.L.); [email protected] (S.N.); [email protected] (S.C.); [email protected] (Y.S.C.); [email protected] (G.W.K.) 2 Department of Biostatistics, Clinical Trial Center, Soonchunhyang University Bucheon Hospital, Bucheon 14584, Korea; [email protected] * Correspondence: [email protected] † Hoon Lim and Young Hwan Lee contributed equally to this work. Abstract: Carbon monoxide (CO) is one of the most common poisoning substances worldwide. Since acute brain injury (ABI) is an important determinant of the neurological outcome in CO poisoning, screening for patients at a high risk of developing ABI is essential for the proper treatment. This study identified predictors of ABI in patients with CO poisoning. This prospective registry-based study was conducted in patients who visited a tertiary care hospital for CO poisoning from August 2016 to June 2020. ABI was defined as the presence of acute hypoxic lesions on diffusion-weighted magnetic resonance imaging. Multiple logistic regression analysis was performed to identify the predictors of ABI. Of 231 patients, 64 (27.7%) showed ABI. Multiple logistic regression analysis showed that a Citation: Lim, H.; Lee, Y.H.; Nah, S.; Glasgow Coma Scale (GCS) score <9 at presentation (odds ratio [OR] 3.28, 95% confidence interval Choi, S.; Cho, Y.S.; Kim, G.W.; Moon, (CI) 1.08–10.01), creatinine level >1.2 mg/dL (OR 3.04, 95% CI 1.16–8.01), and C-reactive protein J.E.; Han, S. -

Pharmacologic Treatment of Meningitis and Encephalitis in Adult Patients
Published online: 2019-06-19 THIEME Review Article 145 Pharmacologic Treatment of Meningitis and Encephalitis in Adult Patients Andrew K. Treister1 Ines P. Koerner2 1Department of Neurology, Oregon Health & Science University, Address for correspondence Andrew K. Treister, MD, Department Portland, Oregon, United States of Neurology, Oregon Health & Science University, 3181 SW Sam 2Department of Anesthesiology and Perioperative Medicine, Jackson Park, CR 120, Portland, OR 97239-3098, United States Oregon Health & Science University, Portland, Oregon, (e-mail: [email protected]). United States J Neuroanaesthesiol Crit Care 2019;6:145–152 Abstract Meningitis and encephalitis are two inflammatory, often infectious, disorders of the meninges and the central nervous system. Both are associated with significant morbidity and mortality, and require early and aggressive targeted treatment. This article reviews pharmacologic treatment strategies for infectious meningitis and encephalitis, using Keywords the latest available research and guidelines. It provides an overview of empiric anti- ► meningitis microbial treatment approaches for a variety of organisms, including a discussion of ► encephalitis trends in antibiotic resistance where applicable. Key steps in diagnosis and general ► antibiotic resistance management are briefly reviewed. Introduction care–associated infections are not covered in detail, as they are excellently discussed in a recent guideline statement.4 The terms meningitis and encephalitis comprise a broad array of infectious and inflammatory processes involving the central nervous system (CNS) that carry significant morbidity Literature Review 1,2 and mortality. Meningitis refers to inflammation of PubMed was searched in January 2019 for articles published primarily the meninges, although it may spread to involve the between January 1, 2009, and December 31, 2018. -

Antimicrobial Treatment Guidelines for Common Infections
Antimicrobial Treatment Guidelines for Common Infections June 2016 Published by: The NB Provincial Health Authorities Anti-infective Stewardship Committee under the direction of the Drugs and Therapeutics Committee Introduction: These clinical guidelines have been developed or endorsed by the NB Provincial Health Authorities Anti-infective Stewardship Committee and its Working Group, a sub- committee of the New Brunswick Drugs and Therapeutics Committee. Local antibiotic resistance patterns and input from local infectious disease specialists, medical microbiologists, pharmacists and other physician specialists were considered in their development. These guidelines provide general recommendations for appropriate antibiotic use in specific infectious diseases and are not a substitute for clinical judgment. Website Links For Horizon Physicians and Staff: http://skyline/patientcare/antimicrobial For Vitalité Physicians and Staff: http://boulevard/FR/patientcare/antimicrobial To contact us: [email protected] When prescribing antimicrobials: Carefully consider if an antimicrobial is truly warranted in the given clinical situation Consult local antibiograms when selecting empiric therapy Include a documented indication, appropriate dose, route and the planned duration of therapy in all antimicrobial drug orders Obtain microbiological cultures before the administration of antibiotics (when possible) Reassess therapy after 24-72 hours to determine if antibiotic therapy is still warranted or effective for the given organism or