Reserwd for Peoject Logo/Iieading Africai{Programme
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Non-Timber Forest Products and Climate Change Adaptation Among Forest-Dependent Communities in Bamboko Forest Reserve, the Southwest Region of Cameroon
Non-timber forest products and climate change adaptation among forest-dependent communities in Bamboko forest reserve, the southwest region of Cameroon Tieminie Robinson Nghogekeh ( [email protected] ) TTRECED Cameroon Chia Eugene Loh GIZ Yaounde,Cameroon Tieguhong Julius Chupezi African Development Bank Nghobuoche Frankline Mayiadieh Universite de Yaounde I Piabuo Serge Mandiefe ICRAF-Cameroon Mamboh Rolland Tieguhong Universite de Yaounde II Research Keywords: NTFPs, Climate change, adaptation, BFR, South West Region, Cameroon Posted Date: November 19th, 2020 DOI: https://doi.org/10.21203/rs.3.rs-61744/v2 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Version of Record: A version of this preprint was published on March 9th, 2021. See the published version at https://doi.org/10.1186/s40068-020-00215-z. Page 1/24 Abstract Background: Forests are naturally endowed to combat climate change by protecting people and livelihoods as well as creating a base for sustainable economic and social development. But this natural mechanism is often hampered by anthropogenic activities. It is therefore imperative to take measures that are environmentally sustainable not only for mitigation but also for its adaptation. This study was carried out to assess the role of Non-timber forest products (NTFPs) as a strategy to cope with the impacts of climate change among forest-dependent communities around the Bamkoko Forest Reserve in the South West Region of Cameroon. Methods: Datasets were collected through household questionnaires (20% of the population in each village that constitute the study site was a sample), participatory rural appraisal techniques, transect walks in the 4 corners of the Bamboko Forest Reserve with a square sample of 25 m2 x 25 m2 to identied and record NTFPs in the reserve, and direct eld observations. -
Rapid Protection Assessments Summary Report
Rapid Protection Assessments Summary Report Danish Refugee Council Southwest Cameroon December 2020 Cameroon – RPA Report – December 2020 Table of Content 1. Introduction ....................................................................................................... 4 1.2 Methodology ................................................................................................................................. 4 1.3 Information on Key Informants (KIs) ............................................................................................ 5 2. Communities’ General Profile ..................................................................................... 6 2.1 Pre and post crisis population movements ................................................................................. 6 2.2 Vulnerability profile ...................................................................................................................... 7 2.2.1 Displacement profile ................................................................................................................ 7 2.2.2 Vulnerability types .................................................................................................................... 7 3. Access to services ...................................................................................................... 8 3.1 Education ...................................................................................................................................... 8 3.2 Health ........................................................................................................................................... -

Shelter Cluster Dashboard NWSW052021
Shelter Cluster NW/SW Cameroon Key Figures Individuals Partners Subdivisions Cameroon 03 23,143 assisted 05 Individual Reached Trend Nigeria Furu Awa Ako Misaje Fungom DONGA MANTUNG MENCHUM Nkambe Bum NORD-OUEST Menchum Nwa Valley Wum Ndu Fundong Noni 11% BOYO Nkum Bafut Njinikom Oku Kumbo Belo BUI Mbven of yearly Target Njikwa Akwaya Jakiri MEZAM Babessi Tubah Reached MOMO Mbeggwi Ngie Bamenda 2 Bamenda 3 Ndop Widikum Bamenda 1 Menka NGO KETUNJIA Bali Balikumbat MANYU Santa Batibo Wabane Eyumodjock Upper Bayang LEBIALEM Mamfé Alou OUEST Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Fontem Nguti KOUPÉ HNO/HRP 2021 (NW/SW Regions) Toko MANENGOUBA Bangem Mundemba SUD-OUEST NDIAN Konye Tombel 1,351,318 Isangele Dikome value Kumba 2 Ekondo Titi Kombo Kombo PEOPLE OF CONCERN Abedimo Etindi MEME Number of PoC Reached per Subdivision Idabato Kumba 1 Bamuso 1 - 100 Kumba 3 101 - 2,000 LITTORAL 2,001 - 13,000 785,091 Mbongé Muyuka PEOPLE IN NEED West Coast Buéa FAKO Tiko Limbé 2 Limbé 1 221,642 Limbé 3 [ Kilometers PEOPLE TARGETED 0 15 30 *Note : Sources: HNO 2021 PiN includes IDP, Returnees and Host Communi�es The boundaries and names shown and the designations used on this map do not imply official endorsement or acceptance by the United Nations Key Achievement Indicators PoC Reached - AGD Breakdouwn 296 # of Households assisted with Children 27% 26% emergency shelter 1,480 Adults 21% 22% # of households assisted with core 3,769 Elderly 2% 2% relief items including prevention of COVID-19 21,618 female male 41 # of households assisted with cash for rental subsidies 41 Households Reached Individuals Reached Cartegories of beneficiaries reported People Reached by region Distribution of Shelter NFI kits integrated with COVID 19 KITS in Matoh town. -
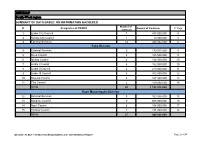
MINMAP South-West Region
MINMAP South-West region SUMMARY OF DATA BASED ON INFORMATION GATHERED Number of N° Designation of PO/DPO Amount of Contracts N° Page contracts 1 Limbe City Council 7 475 000 000 4 2 Kumba City Council 1 10 000 000 5 3 External Services 14 440 032 000 6 Fako Division 4 External Services 9 179 015 000 8 5 Buea Council 5 125 500 000 9 6 Idenau Council 4 124 000 000 10 7 Limbe I Council 4 152 000 000 10 8 Limbe II Council 4 219 000 000 11 9 Limbe III Council 6 102 500 000 12 10 Muyuka Council 6 127 000 000 13 11 Tiko Council 5 159 000 000 14 TOTAL 43 1 188 015 000 Kupe Muanenguba Division 12 External Services 5 100 036 000 15 13 Bangem Council 9 605 000 000 15 14 Nguti Council 6 104 000 000 17 15 Tombel Council 7 131 000 000 18 TOTAL 27 940 036 000 MINMAP / PUBLIC CONTRACTS PROGRAMMING AND MONITORING DIVISION Page 1 of 34 MINMAP South-West region SUMMARY OF DATA BASED ON INFORMATION GATHERED Lebialem Division 16 External Services 5 134 567 000 19 17 Alou Council 9 144 000 000 19 18 Menji Council 3 181 000 000 20 19 Wabane Council 9 168 611 000 21 TOTAL 26 628 178 000 Manyu Division 18 External Services 5 98 141 000 22 19 Akwaya Council 6 119 500 000 22 20 Eyomojock Council 6 119 000 000 23 21 Mamfe Council 5 232 000 000 24 22 Tinto Council 6 108 000 000 25 TOTAL 28 676 641 000 Meme Division 22 External Services 5 85 600 000 26 23 Mbonge Council 7 149 000 000 26 24 Konye Council 1 27 000 000 27 25 Kumba I Council 3 65 000 000 27 26 Kumba II Council 5 83 000 000 28 27 Kumba III Council 3 84 000 000 28 TOTAL 24 493 600 000 MINMAP / PUBLIC CONTRACTS -
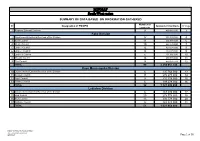
MINMAP South-West Region
MINMAP South-West region SUMMARY OF DATA BASED ON INFORMATION GATHERED Number of N° Designation of PO/DPO Amount of Contracts N° Page contracts 1 Regional External Services 9 490 982 000 3 Fako Division 2 Départemental External Services of the Division 17 352 391 000 4 3 Buea Council 11 204 778 000 6 4 Idenau Council 10 224 778 000 7 5 Limbe I Council 12 303 778 000 8 6 Limbe II Council 13 299 279 000 9 7 Limbe III Council 6 151 900 000 10 8 Muyuka Council 16 250 778 000 11 9 Tiko Council 14 450 375 748 12 TOTAL 99 2 238 057 748 Kupe Muanenguba Division 10 Départemental External Services of the Division 6 135 764 000 13 11 Bangem Council 11 572 278 000 14 12 Nguti Council 9 215 278 000 15 13 Tombel Council 6 198 278 000 16 TOTAL 32 1 121 598 000 Lebialem Division 14 Départemental External Services of the Division 6 167 474 000 17 15 Alou Council 20 278 778 000 18 16 Menji Council 13 306 778 000 20 17 Wabane Council 12 268 928 000 21 TOTAL 51 1 021 958 000 PUBLIC CONTRACTS PROGRAMMING AND MONITORING DIVISION /MINMAP Page 1 of 36 MINMAP South-West region SUMMARY OF DATA BASED ON INFORMATION GATHERED Number of N° Designation of PO/DPO Amount of Contracts N° Page contracts Manyu Division 18 Départemental External Services of the Division 9 240 324 000 22 19 Akwaya Council 10 260 278 000 23 20 Eyumojock Council 6 195 778 000 24 21 Mamfe Council 7 271 103 000 24 22 Tinto Council 7 219 778 000 25 TOTAL 39 1 187 261 000 Meme Division 23 Départemental External Services of the Division 4 82 000 000 26 24 Konye Council 5 171 533 000 26 25 Kumba -

South West Assessment
Cameroon Emergency Response – South West Assessment SOUTH WEST CAMEROON November 2018 – January 2019 - i - CONTENTS 1 CONTEXT ..................................................................................................................... 4 1.1 The crisis in numbers:.................................................................................................... 5 1.2 Overall Objectives of SW Assessment ........................................................................... 5 1.3 Area of Intervention ...................................................................................................... 6 2 METHODOLOGY .......................................................................................................... 6 2.1 Assessment site selection: ............................................................................................ 8 2.2 Configuration of the assessment team: ........................................................................ 8 2.3 Indicators of vulnerability verified during the rapid assessment: ................................ 9 2.3.1 Nutrition and Health ............................................................................................. 9 2.3.2 WASH ..................................................................................................................... 9 3.1.1 Food Security ......................................................................................................... 9 2.4 Sources of Information ............................................................................................... -
2017/2018 Annual Report
Service to humanity TABLE OF CONTENTS 1 TABLE OF CONTENTS TABLE OF CONTENTS ..................................................................................................................................................... 1 ACRONYMS .................................................................................................................................................................... 2 ACKNOWLEDGMENT ..................................................................................................................................................... 4 FOREWORD .................................................................................................................................................................... 5 1. OVERVIEW OF AJESH ................................................................................................................................................. 6 1.1 Organisation Background .................................................................................................................................... 6 1.1.1 Vision ............................................................................................................................................................ 6 1.1.2 Mission ......................................................................................................................................................... 6 1.1.3 Global objective .......................................................................................................................................... -

206 Villages Burnt in the North West and South West Regions
CHRDA Email: [email protected] Website: www.chrda.org Cameroon: The Anglophone Crisis 206 Villages burnt in the North West and South West Regions April 2019 SUMMARY The Center for Human Rights and Democracy in Africa (CHRDA) has analyzed data from local sources and identified 206 villages that have been partially, or completely burnt since the beginning of the immediate crisis in the Anglophone regions. Cameroon is a nation sliding into civil war in Africa. In 2016, English- speaking lawyers, teachers, students and civil society expressed “This act of burning legitimate grievances to the Cameroonian government. Peaceful protests villages is in breach of subsequently turned deadly following governments actions to prevent classical common the expression of speech and assembly. Government forces shot peaceful article 3 to the Four protesters, wounded many and killed several. Geneva Convention 1949 and the To the dismay of the national, regional and international communities, Additional Protocol II the Cameroon government began arresting activists and leaders to the same including CHRDA’s Founder and CEO, Barrister Agbor Balla, the then Convention dealing President of the now banned Anglophone Consortium. Internet was shut with the non- down for three months and all forms of dissent were stifled, forcing international conflicts. hundreds into exile. Also, the burning of In August 2017, President Paul Biya of Cameroon ordered the release of villages is in breach of several detainees, but avoided dialogue, prompting mass protests in national and September 2017 with an estimated 500,000 people on the streets of international human various cities, towns and villages. The government’s response was a rights norms and the brutal crackdown which led to a declaration of independence on October host of other laws” 1, 2017. -

“These Killings Can Be Stopped” RIGHTS Government and Separatist Groups Abuses in Cameroon’S WATCH Anglophone Regions
HUMAN “These Killings Can Be Stopped” RIGHTS Government and Separatist Groups Abuses in Cameroon’s WATCH Anglophone Regions “These Killings Can Be Stopped” Abuses by Government and Separatist Groups in Cameroon’s Anglophone Regions Copyright © 2018 Human Rights Watch All rights reserved. Printed in the United States of America ISBN: 978-1-6231-36352 Cover design by Rafael Jimenez Human Rights Watch defends the rights of people worldwide. We scrupulously investigate abuses, expose the facts widely, and pressure those with power to respect rights and secure justice. Human Rights Watch is an independent, international organization that works as part of a vibrant movement to uphold human dignity and advance the cause of human rights for all. Human Rights Watch is an international organization with staff in more than 40 countries, and offices in Amsterdam, Beirut, Berlin, Brussels, Chicago, Geneva, Goma, Johannesburg, London, Los Angeles, Moscow, Nairobi, New York, Paris, San Francisco, Sydney, Tokyo, Toronto, Tunis, Washington DC, and Zurich. For more information, please visit our website: http://www.hrw.org JULY 2018 ISBN: 978-1-6231-36352 “These Killings Can Be Stopped” Abuses by Government and Separatist Groups in Cameroon’s Anglophone Regions Map .................................................................................................................................... i Summary ........................................................................................................................... 1 Recommendations ............................................................................................................. -
SSA Infographic
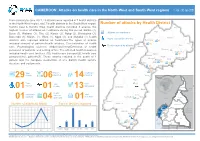
CAMEROON: Attacks on health care in the North-West and South-West regions 1 Jan - 30 Jun 2021 From January to June 2021, 29 attacks were reported in 7 health districts in the North-West region, and 7 health districts in the South West region. Number of attacks by Health District Kumbo East & Kumbo West health districts recorded 6 attacks, the Ako highest number of attacks on healthcare during this period. Batibo (4), Wum Buea (3), Wabane (3), Tiko (2), Konye (2), Ndop (2), Benakuma (2), Attacks on healthcare Bamenda (1), Mamfe (1), Wum (1), Nguti (1), and Muyuka (1) health Injury caused by attacks Nkambe districts also reported attacks on healthcare.The types of attacks Benakuma 01 included removal of patients/health workers, Criminalization of health 02 Nwa Death caused by attacks Ndu care, Psychological violence, Abduction/Arrest/Detention of health Akwaya personnel or patients, and setting of fire. The affected health resources Fundong Oku Kumbo West included health care facilities (10), health care transport(2), health care Bafut 06 Njikwa personnel(16), patients(7). These attacks resulted in the death of 1 Tubah Kumbo East Mbengwi patient and the complete destruction of one district health service Bamenda Ndop 01 Batibo Bali 02 structure and equipments. Mamfe 04 Santa 01 Eyumojock Wabane 03 Total Patient Healthcare 29 Attacks 06 impacted 14 impacted Fontem Nguti Total Total Total 01 Injured Deaths Kidnapping EXTRÊME-NORD Mundemba FAR-NORTH CHAD 01 01 13 Bangem Health Total Ambulance services Konye impacted Detention Kumba North Tombel NONORDRTH 01 04 destroyed 01 02 NIGERIA Bakassi Ekondo Titi Number of attacks by Month Type of facilities impacted AADAMAOUADAMAOUA NORTH- 14 13 NORD-OUESTWEST Kumba South CENTRAL 12 WOUESTEST AFRICAN Mbonge SOUTH- SUD-OUEST REPUBLIC 10 WEST Muyuka CCENTREENTRE 8 01 LLITITTORALTORAL EASESTT 6 5 4 4 Buea 4 03 Tiko 2 Limbe Atlantic SSUDOUTH 1 02 Ocean 2 EQ. -
REPUBLIQUE DU CAMEROUN ************** Paix – Travail
REPUBLIQUE DU REPUBLIC OF CAMEROUN CAMEROON ************** **************** Paix – Travail – Patrie Peace – Work – Fatherland **************** **************** REGION DE SUD OUEST SOUTH WEST REGION **************** *************** DEPARTEMENT DU LEBIALEM DIVISION LEBIALEM ************** *************** BANGEM COUNCIL COMMUNE DE BANGEM SURVEY REPORT MECHANISM OF CITIZEN CONTROL OF THE PUBLIC ACTION IN THE COUNCIL OF BANGEM May 2018 Technical and financial support of the National Community-Driven Development Program (NCDDP) in collaboration with the National Institute of Statistics (INS) Realised by: AJEMALEBU SELF HELP (AJESH) TABLE OF CONTENTS TABLE OF CONTENTS ................................................................................................................. i LIST OF ACRONYMS ................................................................................................................. iv LIST OF TABLES .......................................................................................................................... v LIST OF CHARTS (FIGURES) .................................................................................................... vi LIST OF MAPS ............................................................................................................................. vi FOREWORD ................................................................................................................................ vii EXECUTIVE SUMMARY ........................................................................................................ -

Press Release Organisation of Mobile Clinic
PRESS RELEASE ORGANISATION OF MOBILE CLINIC ACTIVITIES IN THE SOUTH WEST REGION Buea, February 16th, 2021 - The United Nations Populations Fund (UNFPA) and the Ministry of Public Health in partnership with the Cameroon Baptist Convention Hospital Services will on Thursday February 25th, 2021 set up a mobile clinic in the village of Kosala in the Kumba II Subdivision of Meme Division, South West Region of Cameroon at 7am. The event which falls under the World Bank Pandemic Emergency Financing Facility (PEF) Project run in the North West and South West Regions,aims at: • Reducing preventable maternal and new-born morbidities and mortalities in the North West Region (NWR) within the covid-19 pandemic and ongoing humanitarian crisis. • Reducing unmet need for Family planning in underserved populations and communities in the North West and South West Regions (NWSW) Insecurity, destruction of health infrastructure and ‘ghost towns’ have significantly reduced access to basic health services. During 2018, 175/368 (47%) and 184/368 (50%) facilities reported being affected by the crisis in the first and second half of the year respectively in the NW region (displacement of staff, destruction, difficulties in the supply of medical products, and difficulties in geographical access due to the destruction of roads or barricades/checkpoints). As of December 31, 2019, 9% (33/368) of health facilities in the NW were non-functional, with the health districts of Ako (50%), Batibo (21%), Nkambe (16%) and Bafut (16%) being the most affected, and 3% were partially