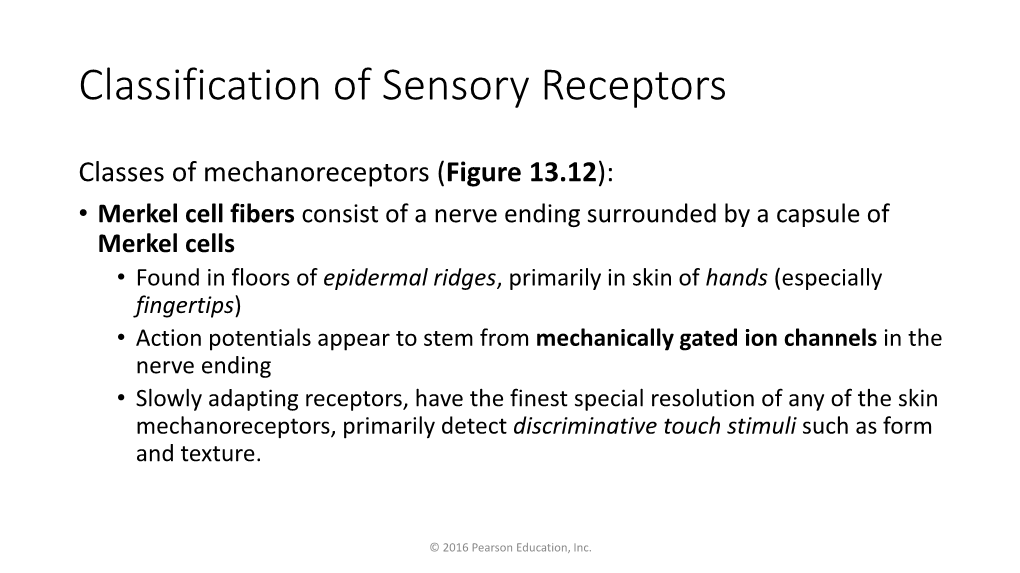
Muscle Spindles and Golgi Tendon Organs
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Download Edissertation
The Human Nociceptive Withdrawal Reflex The Human Nociceptive Withdrawal Reflex Improved Understanding and Optimization of Reflex Elicitation and Recording PhD Thesis by Ken Steffen Frahm Center for Sensory-Motor Interaction, Department of Health Science and Technology, Aalborg University, Denmark ISBN 978-87-92982-69-8 (paperback) ISBN 978-87-92982-68-1 (e-book) Published, sold and distributed by: River Publishers Niels Jernes Vej 10 9220 Aalborg Ø Denmark Tel.: +45369953197 www.riverpublishers.com Copyright for this work belongs to the author, River Publishers have the sole right to distribute this work commercially. All rights reserved c 2013 Ken Steffen Frahm. No part of this work may be reproduced, stored in a retrieval system, or trans- mitted in any form or by any means, electronic, mechanical, photocopying, microfilming, recording or otherwise, without prior written permission from the Publisher. Contents Preface vii Acknowledgements ix English summary xi Danish summary xiii List of abbreviations xv Introduction 1 1.1 The Nociceptive Withdrawal Reflex ......................................... 2 Aims 7 2.1 Overview of study aims ............................................................. 9 2.2 Papers ...................................................................................... 10 Methods 11 3.1 Reflex monitoring (study I) ..................................................... 11 3.2 Noxious stimulation (study I & II) .......................................... 15 3.3 Mapping the neural activation in the sole of the foot (study -
Chapter 2 Test Review
Unit III, Modules 9-13 Test Review • See also the Unit III notes and pages 76-122 • About 45 m.c., plus two essays; one on brain functioning, the other review concepts from previous units. • Some practice questions are embedded in this presentation • Other practice questions are available at the textbook website and in the textbook after each module. Neuron Order of a transmission: dendrite, cell body, axon, synapse (see arrow below) Neural Communication Neurons, 80 Neural Communication • (a)Dendrite – the bushy, branching extensions of a neuron that receive messages and conduct impulses toward the (b)cell body • (c)Axon – the extension of a neuron, ending in branching terminal fibers, through which messages are sent to other neurons or to muscles or glands • Myelin [MY-uh-lin] Sheath – a layer of fatty cells segmentally encasing the fibers of many neurons – makes possible vastly greater transmission speed of neutral impulses, – Damage to can lead to Multiple sclerosis Neural Communication • Action Potential – a neural impulse; a brief electrical charge that travels down an axon; DEPOLARIZED – generated by the movement of positively charges atoms in and out of channels in the axon’s membrane • Threshold – the level of stimulation required to trigger a neural impulse Action Potential A neural impulse. A brief electrical charge that travels down an axon and is generated by the movement of positively charged atoms in and out of channels in the axon’s membrane. Practice question • Multiple sclerosis is a disease that is most directly associated with the degeneration of: a. the myelin sheath. b. the pituitary gland. -

Focusing on the Re-Emergence of Primitive Reflexes Following Acquired Brain Injuries
33 Focusing on The Re-Emergence of Primitive Reflexes Following Acquired Brain Injuries Resiliency Through Reconnections - Reflex Integration Following Brain Injury Alex Andrich, OD, FCOVD Scottsdale, Arizona Patti Andrich, MA, OTR/L, COVT, CINPP September 19, 2019 Alex Andrich, OD, FCOVD Patti Andrich, MA, OTR/L, COVT, CINPP © 2019 Sensory Focus No Pictures or Videos of Patients The contents of this presentation are the property of Sensory Focus / The VISION Development Team and may not be reproduced or shared in any format without express written permission. Disclosure: BINOVI The patients shown today have given us permission to use their pictures and videos for educational purposes only. They would not want their images/videos distributed or shared. We are not receiving any financial compensation for mentioning any other device, equipment, or services that are mentioned during this presentation. Objectives – Advanced Course Objectives Detail what primitive reflexes (PR) are Learn how to effectively screen for the presence of PRs Why they re-emerge following a brain injury Learn how to reintegrate these reflexes to improve patient How they affect sensory-motor integration outcomes How integration techniques can be used in the treatment Current research regarding PR integration and brain of brain injuries injuries will be highlighted Cases will be presented Pioneers to Present Day Leaders Getting Back to Life After Brain Injury (BI) Descartes (1596-1650) What is Vision? Neuro-Optometric Testing Vision writes spatial equations -

Improvement and Neuroplasticity After Combined Rehabilitation to Forced Grasping
Hindawi Case Reports in Neurological Medicine Volume 2017, Article ID 1028390, 7 pages https://doi.org/10.1155/2017/1028390 Case Report Improvement and Neuroplasticity after Combined Rehabilitation to Forced Grasping Michiko Arima, Atsuko Ogata, Kazumi Kawahira, and Megumi Shimodozono Department of Rehabilitation and Physical Medicine, Kagoshima University Graduate School of Medical and Dental Sciences, Kagoshima, Japan Correspondence should be addressed to Michiko Arima; [email protected] Received 20 September 2016; Revised 31 December 2016; Accepted 9 January 2017; Published 6 February 2017 Academic Editor: Pablo Mir Copyright © 2017 Michiko Arima et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. The grasp reflex is a distressing symptom but the need to treat or suppress it has rarely been discussed in the literature. We report the case of a 17-year-old man who had suffered cerebral infarction of the right putamen and temporal lobe 10 years previously. Forced grasping of the hemiparetic left upper limb was improved after a unique combined treatment. Botulinum toxin typeA (BTX-A) was first injected into the left biceps, wrist flexor muscles, and finger flexor muscles. Forced grasping was reduced along with spasticity of the upper limb. In addition, repetitive facilitative exercise and object-related training were performed under low-amplitude continuous neuromuscular electrical stimulation. Since this 2-week treatment improved upper limb function, we compared brain activities, as measured by near-infrared spectroscopy during finger pinching, before and after the combined treatment. -

Signaling by Sensory Receptors
Signaling by Sensory Receptors David Julius1 and Jeremy Nathans2 1Department of Physiology, University of California School of Medicine, San Francisco, California 94158 2Department of Molecular Biology and Genetics, Johns Hopkins Medical School, Baltimore, Maryland 21205 Correspondence: [email protected] and [email protected] SUMMARY Sensory systems detect small molecules, mechanical perturbations, or radiation via the activa- tion of receptor proteins and downstream signaling cascades in specialized sensory cells. In vertebrates, the two principal categories of sensory receptors are ion channels, which mediate mechanosensation, thermosensation, and acid and salt taste; and G-protein-coupled recep- tors (GPCRs), which mediate vision, olfaction, and sweet, bitter, and umami tastes. GPCR- based signaling in rods and cones illustrates the fundamental principles of rapid activation and inactivation, signal amplification, and gain control. Channel-based sensory systems illus- trate the integration of diverse modulatory signals at the receptor, as seen in the thermosen- sory/pain system, and the rapid response kinetics that are possible with direct mechanical gating of a channel. Comparisons of sensory receptor gene sequences reveal numerous exam- ples in which gene duplication and sequence divergence have created novel sensory specific- ities. This is the evolutionary basis for the observed diversity in temperature- and ligand- dependent gating among thermosensory channels, spectral tuning among visual pigments, and odorant binding among olfactory receptors. The coding of complex external stimuli by a limited number of sensory receptor types has led to the evolution of modality-specific and species-specific patterns of retention or loss of sensory information, a filtering operation that selectively emphasizes features in the stimulus that enhance survival in a particular ecological niche. -

The Grasp Reflex and Moro Reflex in Infants: Hierarchy of Primitive
Hindawi Publishing Corporation International Journal of Pediatrics Volume 2012, Article ID 191562, 10 pages doi:10.1155/2012/191562 Review Article The Grasp Reflex and Moro Reflex in Infants: Hierarchy of Primitive Reflex Responses Yasuyuki Futagi, Yasuhisa Toribe, and Yasuhiro Suzuki Department of Pediatric Neurology, Osaka Medical Center and Research Institute for Maternal and Child Health, 840 Murodo-cho, Izumi, Osaka 594-1101, Japan Correspondence should be addressed to Yasuyuki Futagi, [email protected] Received 27 October 2011; Accepted 30 March 2012 Academic Editor: Sheffali Gulati Copyright © 2012 Yasuyuki Futagi et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. The plantar grasp reflex is of great clinical significance, especially in terms of the detection of spasticity. The palmar grasp reflex also has diagnostic significance. This grasp reflex of the hands and feet is mediated by a spinal reflex mechanism, which appears to be under the regulatory control of nonprimary motor areas through the spinal interneurons. This reflex in human infants can be regarded as a rudiment of phylogenetic function. The absence of the Moro reflex during the neonatal period and early infancy is highly diagnostic, indicating a variety of compromised conditions. The center of the reflex is probably in the lower region of the pons to the medulla. The phylogenetic meaning of the reflex remains unclear. However, the hierarchical interrelation among these primitive reflexes seems to be essential for the arboreal life of monkey newborns, and the possible role of the Moro reflex in these newborns was discussed in relation to the interrelationship. -

Central Nervous System
MCQ : Central Nervous System Section 1 General Functional Organization of the Nervous System 1 ) The central nervous system includes all the following components, except :- a- spinal cord b- medulla oblongata c- autonomic ganglia d- diencephalon 2 ) The central nervous system is connected with the peripheral nervous system by all the following types of nerve fibers, except :- a- postganglionic autonomic fibers b- preganglionic autonomic fibers c- somatic motor fibers d- autonomic sensory fibers 3 ) The sensory system is involved in all the following, except :- a- initiation of reflex movements b- initiation of voluntary movements c- learning processes d- initiation of emotional responses 1 MCQ : Central Nervous System Section 2 Sensory System and Sensory Receptors 1) The two-element sensory receptors differ from other types of receptors in being:- a- more numerous b- more widely spread in the body c- more sensitive d- composed of specialized cells at the sensory nerve terminals 2) Sensory receptors are classified functionally according to the following criteria, except :- a- their location in the body b- the nature of tissues in which they are found c- the nature of stimuli acting on them d- their connection with cerebral coretx 3) Most sensory receptors :- a- are stimulated by different types of stimuli b- are stimulated only by specific stimuli c- posses a high threshold for their specific stimuli d- only ‘b’ and ‘c’ are correct 4) A specific stimulus produces a receptor potential by :- a- inhibiting Na + influx into receptor b- inhibiting -

Retained Neonatal Reflexes | the Chiropractic Office of Dr
Retained Neonatal Reflexes | The Chiropractic Office of Dr. Bob Apol 12/24/16, 1:56 PM Temper tantrums Hypersensitive to touch, sound, change in visual field Moro Reflex The Moro Reflex is present at 9-12 weeks after conception and is normally fully developed at birth. It is the baby’s “danger signal”. The baby is ill-equipped to determine whether a signal is threatening or not, and will undergo instantaneous arousal. This may be due to sudden unexpected occurrences such as change in head position, noise, sudden movement or change of light or even pain or temperature change. This activates the stress response system of “fight or flight”. If the Moro Reflex is present after 6 months of age, the following signs may be present: Reaction to foods Poor regulation of blood sugar Fatigues easily, if adrenalin stores have been depleted Anxiety Mood swings, tense muscles and tone, inability to accept criticism Hyperactivity Low self-esteem and insecurity Juvenile Suck Reflex This is active together with the “Rooting Reflex” which allows the baby to feed and suck. If this reflex is not sufficiently integrated, the baby will continue to thrust their tongue forward, pushing on the upper jaw and causing an overbite. This by nature affects the jaw and bite position. This may affect: Chewing Difficulties with solid foods Dribbling Rooting Reflex Light touch around the mouth and cheek causes the baby’s head to turn to the stimulation, the mouth to open and tongue extended in preparation for feeding. It is present from birth usually to 4 months. -

The Corneomandibular Reflex1
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.34.3.236 on 1 June 1971. Downloaded from J. Neurol. Neurosurg. Psychiat., 1971, 34, 236-242 The corneomandibular reflex1 ROBERT M. GORDON2 AND MORRIS B. BENDER From the Department of Neurology, the Mount Sinai Hospital, New York, U.S.A. SUMMARY Seven patients are presented in whom a prominent corneomandibular reflex was observed. These patients all had severe cerebral and/or brain-stem disease with altered states of consciousness. Two additional patients with less prominent and inconstant corneomandibular reflexes were seen; one had bulbar amyotrophic lateral sclerosis and one had no evidence of brain disease. The corneomandibular reflex, when found to be prominent, reflects an exaggeration of the normal. Therefore one may consider the corneomandibular hyper-reflexia as possibly due to disease of the corticobulbar system. The corneomandibular reflex consists of an involun- weak bilateral response on a few occasions. This tary contralateral deviation and protrusion of the was a woman with bulbar and spinal amyotrophic lower jaw during corneal stimulation. It is not a lateral sclerosis. The other seven patients hadProtected by copyright. common phenomenon and has been rediscovered prominent and consistently elicited corneo- several times since its initial description by Von mandibular reflexes. The clinical features common to Solder in 1902. It is found mostly in patients with these patients were (1) the presence of bilateral brain-stem or bilateral cerebral lesions who are in corneomandibular reflexes, in some cases more coma or semicomatose. prominent on one side; (2) a depressed state of con- There have been differing opinions as to the sciousness, usually coma; and (3) the presence of incidence, anatomical basis, and clinical significance severe neurological abnormalities, usually motor, of this reflex. -

Vocabulario De Morfoloxía, Anatomía E Citoloxía Veterinaria
Vocabulario de Morfoloxía, anatomía e citoloxía veterinaria (galego-español-inglés) Servizo de Normalización Lingüística Universidade de Santiago de Compostela COLECCIÓN VOCABULARIOS TEMÁTICOS N.º 4 SERVIZO DE NORMALIZACIÓN LINGÜÍSTICA Vocabulario de Morfoloxía, anatomía e citoloxía veterinaria (galego-español-inglés) 2008 UNIVERSIDADE DE SANTIAGO DE COMPOSTELA VOCABULARIO de morfoloxía, anatomía e citoloxía veterinaria : (galego-español- inglés) / coordinador Xusto A. Rodríguez Río, Servizo de Normalización Lingüística ; autores Matilde Lombardero Fernández ... [et al.]. – Santiago de Compostela : Universidade de Santiago de Compostela, Servizo de Publicacións e Intercambio Científico, 2008. – 369 p. ; 21 cm. – (Vocabularios temáticos ; 4). - D.L. C 2458-2008. – ISBN 978-84-9887-018-3 1.Medicina �������������������������������������������������������������������������veterinaria-Diccionarios�������������������������������������������������. 2.Galego (Lingua)-Glosarios, vocabularios, etc. políglotas. I.Lombardero Fernández, Matilde. II.Rodríguez Rio, Xusto A. coord. III. Universidade de Santiago de Compostela. Servizo de Normalización Lingüística, coord. IV.Universidade de Santiago de Compostela. Servizo de Publicacións e Intercambio Científico, ed. V.Serie. 591.4(038)=699=60=20 Coordinador Xusto A. Rodríguez Río (Área de Terminoloxía. Servizo de Normalización Lingüística. Universidade de Santiago de Compostela) Autoras/res Matilde Lombardero Fernández (doutora en Veterinaria e profesora do Departamento de Anatomía e Produción Animal. -

What's the Connection?
WHAT’S THE CONNECTION? Sharon Winter Lake Washington High School Directions for Teachers 12033 NE 80th Street Kirkland, WA 98033 SYNOPSIS Students elicit and observe reflex responses and distinguish between types STUDENT PRIOR KNOWL- of reflexes. They then design and conduct experiments to learn more about EDGE reflexes and their control by the nervous system. Before participating in this LEVEL activity students should be able to: Exploration, Concept/Term Introduction Phases ■ Describe the parts of a Application Phase neuron and explain their functions. ■ Distinguish between sensory and motor neurons. Getting Ready ■ Describe briefly the See sidebars for additional information regarding preparation of this lab. organization of the nervous system. Directions for Setting Up the Lab General: INTEGRATION Into the Biology Curriculum ■ Make an “X” on the chalkboard for the teacher-led introduction. ■ Health ■ Photocopy the Directions for Students pages. ■ Biology I, II ■ Human Anatomy and Teacher Background Physiology A reflex is an involuntary neural response to a specific sensory stimulus ■ AP Biology that threatens the survival or homeostatic state of an organism. Reflexes Across the Curriculum exist in the most primitive of species, usually with a protective function for ■ Mathematics animals when they encounter external and internal stimuli. A primitive ■ Physics ■ example of this protective reflex is the gill withdrawal reflex of the sea slug Psychology Aplysia. In humans and other vertebrates, protective reflexes have been OBJECTIVES maintained and expanded in number. Examples are the gag reflex that At the end of this activity, occurs when objects touch the sides students will be able to: or the back of the throat, and the carotid sinus reflex that restores blood ■ Identify common reflexes pressure to normal when baroreceptors detect an increase in blood pressure. -

Normal Plantar Response: Integration of Flexor and Extensor Reflex Components
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.26.1.39 on 1 February 1963. Downloaded from J. Neurol. Neurosurg. Psychiat., 1963, 26, 39 Normal plantar response: integration of flexor and extensor reflex components LENNART GRIMBY From the Department of Neurology, Karolinska Institute, Serafimerlasarettet, Stockholm, Sweden The reflexes elicited by painful stimulation of the the suprasegmental control of the reflex centres, the plantar surface of the foot have been studied receptive field of the reflex is limited to the skin area extensively for a long time and the relation between where it is adequate for protective purposes, viz., the reflexes obtained in normal and in pathological the ball of the great toe. cases has been the subject of considerable debate. An Previous investigations (Eklund et al., 1959; excellent survey of previous investigations is to be Kugelberg et al., 1960) have shown that the main found in the review by Walshe (1956). As in most difference between the electromyographic pattern of studies of human reflexes, the technique commonly a flexor plantar response and that of an extensor used has, however, not permitted an exact deter- plantar response is that the reflex plantar flexion of mination of the latency values of the reflexes, and the great toe is associated with activity in the short it has thus not been possible to judge with certainty hallux flexor and reciprocal inhibition of the guest. Protected by copyright. to what extent the movements studied have been voluntary activity in the short hallux extensor, purely spinal and to what extent of cerebral origin. whereas, conversely, reflex dorsiflexion of the great By means of brief electric stimuli and an electro- toe is accompanied by activity in the short hallux myographic recording technique these latency values extensor and reciprocal inhibition of the voluntary can, however, be exactly determined, and in this way activity in the short hallux flexor.