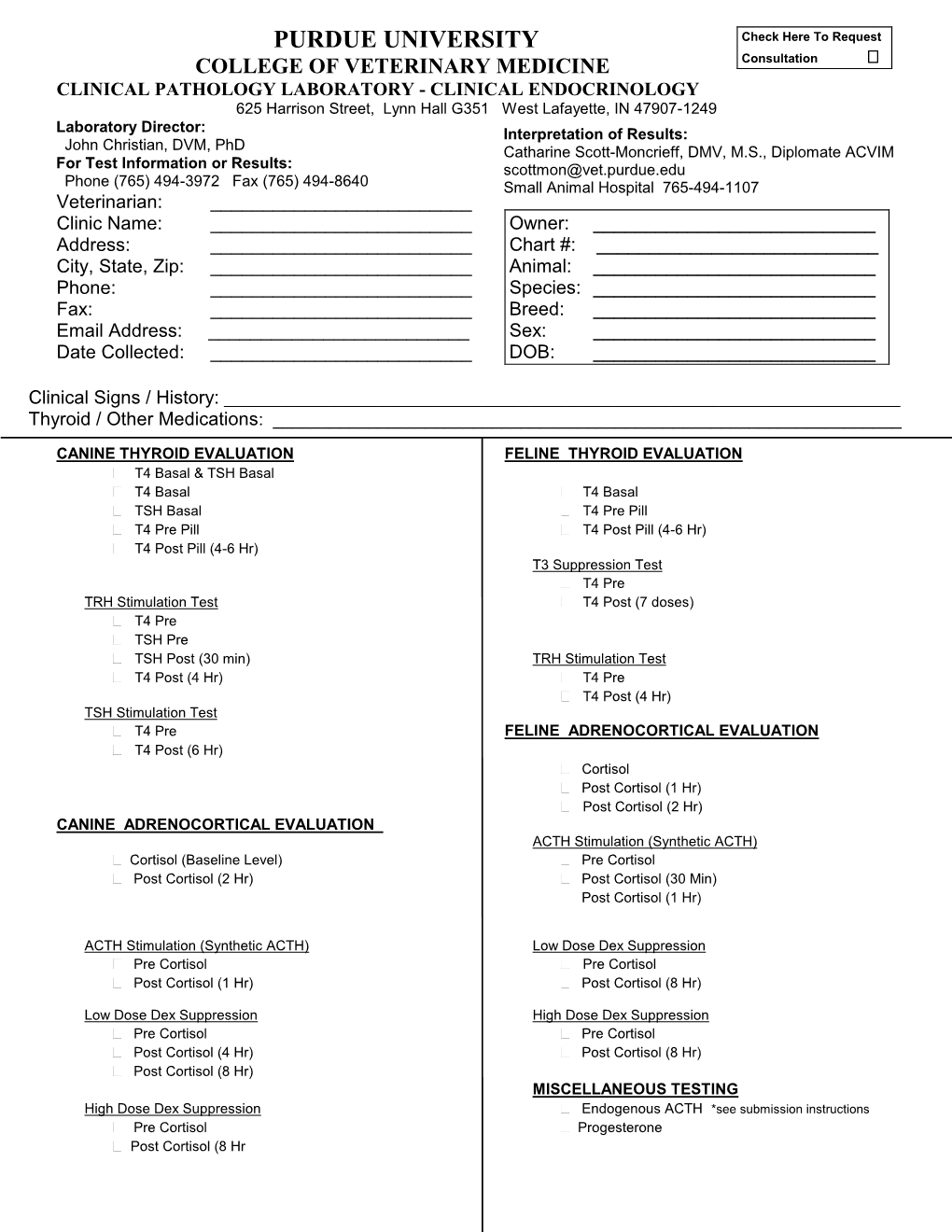
Small Animal Endocrinology Form
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

ACTH Stimulation Tests for the Diagnosis of Adrenal Insufficiency: Systematic Review and Meta-Analysis
ORIGINAL ARTICLE ACTH Stimulation Tests for the Diagnosis of Adrenal Insufficiency: Systematic Review and Meta-Analysis Naykky Singh Ospina,* Alaa Al Nofal,* Irina Bancos, Asma Javed, Khalid Benkhadra, Ekta Kapoor, Aida N. Lteif, Neena Natt, and M. Hassan Murad Evidence-Based Practice Research Program (N.S.O., A.A.N., K.B., M.H.M.), Mayo Clinic, Rochester, Downloaded from https://academic.oup.com/jcem/article/101/2/427/2810551 by guest on 29 September 2021 Minnesota; Knowledge and Evaluation Research Unit (N.S.O., K.B., M.H.M.), Mayo Clinic, Rochester, Minnesota; Division of Endocrinology, Diabetes, Metabolism, and Nutrition (N.S.O., N.N., I.B.), Mayo Clinic, Rochester, Minnesota; Division of Pediatric Endocrinology and Metabolism (A.A.N., A.J., A.N.L.), Mayo Clinic, Rochester, Minnesota; Division of General Internal Medicine (E.K.), Mayo Clinic, Rochester, Minnesota 55905 Context: The diagnosis of adrenal insufficiency is clinically challenging and often requires ACTH stimulation tests. Objective: To determine the diagnostic accuracy of the high- (250 mcg) and low- (1 mcg) dose ACTH stimulation tests in the diagnosis of adrenal insufficiency. Methods: We searched six databases through February 2014. Pairs of independent reviewers se- lected studies and appraised the risk of bias. Diagnostic association measures were pooled across studies using a bivariate model. Data Synthesis: For secondary adrenal insufficiency, we included 30 studies enrolling 1209 adults and 228 children. High- and low-dose ACTH stimulation tests had similar diagnostic accuracy in adults and children using different peak serum cortisol cutoffs. In general, both tests had low sensitivity and high specificity resulting in reasonable likelihood ratios for a positive test (adults: high dose, 9.1; low dose, 5.9; children: high dose, 43.5; low dose, 7.7), but a fairly suboptimal likelihood ratio for a negative test (adults: high dose, 0.39; low dose, 0.19; children: high dose, 0.65; low dose, 0.34). -

SNAP Cortisol Testing Guide
SNAP® Cortisol Testing Guide Diagnosing and Treating Cases of Suspected Canine Hyperadrenocorticism or Addison’s Disease IMPORTANT: Review history of any administration of corticosteroids as these may influence the reported results. Diagnose ACTH Stimulation Test Diagnostic Protocol for Cases of Suspected Canine Hyperadrenocorticism or Addison’s Disease History, physical exam, CBC, chemistry panel, electrolytes and urinalysis consistent with Canine Hyperadrenocorticism or Addison’s disease Draw baseline cortisol sample. Perform an ACTH stimulation test with Cortrosyn® 5 µg/kg IV or ACTH gel 2.2 U/kg IM. Draw 1-hour cortisol (Cortrosyn®) or 1 and 2-hour cortisol (ACTH gel). Pre-ACTH: 2–6 µg/dL Pre- and Post-ACTH Post-ACTH Post-ACTH Post-ACTH 2 6 µg/dL >22 µg/dL <2 µg/dL – Post-ACTH: 6–18 µg/dL 18–22 µg/dL If both results are <2 µg/dL, results are Equivocal, Consistent Inconclusive consistent with Normal Cushing’s possible with Cushing’s hypoadrenocorticism Perform high-dose dexamethasone* Begin treatment with suppression to mineralocorticoid discriminate between and/or glucocorticoid PDH and ATH, as appropriate. ACTH level and/or abdominal ultrasound. * Do not exceed 0.1 mg/kg of dexamethasone. Diagnose Low-Dose Dexamethasone Suppression Protocol For Cases of Suspected Canine Hyperadrenocorticism History, physical exam, CBC, chemistry panel, electrolytes and urinalysis consistent with Canine Hyperadrenocorticism Draw baseline cortisol sample. Perform a low-dose dexamethasone suppression test with 0.01 mg/kg of dexamethasone IV. Draw 4-hour -

Adrenal Incidentalomas with Supraphysiologic Response to ACTH Stimulus: a Case Report
Hindawi Publishing Corporation Case Reports in Endocrinology Volume 2012, Article ID 503290, 4 pages doi:10.1155/2012/503290 Case Report Adrenal Incidentalomas with Supraphysiologic Response to ACTH Stimulus: A Case Report Marianna Antonopoulou1 and Asya Perelstein2 1 SUNY Downstate Medical Center, 450 Clarkson Avenue, Box 1205, Brooklyn, NY 11203, USA 2 VA Medical Center, 800 Poly Place, New York, NY 11209, USA Correspondence should be addressed to Marianna Antonopoulou, [email protected] Received 7 August 2012; Accepted 20 September 2012 Academic Editors: I. Broom, C. Capella, and T. Konrad Copyright © 2012 M. Antonopoulou and A. Perelstein. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. We present the diagnostic approach of a patient with adrenal incidentalomas. A 72-year-old African American male had a CT scan of the abdomen showing right and left adrenal masses measuring 5 × 3.5 cm and 3.7 × 2.9 cm, respectively. The patient had negative hormonal workup. The radiologist insisted that the CT findings are consistent with adrenal hyperplasia, and therefore he underwent ACTH stimulation to rule out late-onset congenital adrenal hyperplasia (CAH). The stimulation test revealed that 17-hydroxyprogesterone and 11-deoxycortisol increased to levels high enough to confirm CAH, but cortisol had exaggerated response as well, thus making the diagnosis of CAH unlikely where metabolism is shifted to precursors. Subsequently, the patient underwent screening for Cushing’s syndrome (CS) with a dexamethasone suppression test. Patient failed the suppresion test, raising the issue for subclinical CS (SCS), likely due to ACTH-independent macronodular adrenal hyperplasia. -

Poster Presentations
______________________________________ P1-d1-164 Adrenals and HPA Axis 1 Arterial hypertension in children: alterations in mineralocorticoid and glucocorticoid axis and their impact on pro-inflammatory, endothelial damage, and oxidative stress parameters Carmen Campino1; Rodrigo Bancalari2; Alejandro Martinez-Aguayo2; Poster Presentations Marlene Aglony2; Hernan Garcia2; Carolina Avalos2; Lilian Bolte2; Carolina Loureiro2; Cristian Carvajal1; Lorena Garcia3; Sergio Lavanderos3; Carlos Fardella1 1Pontificia Universidad Catolica, Endocrinology, and Millennium Institute of Immunology and Immunotherapy, Santiago, Chile; 2Pontificia Universidad Catolica, pediatrics, Santiago, Chile; 3Universidad de Chile, School of Chemical Sciences, Santiago, Chile Background and aims: The pathogenesis of arterial hypertension and its impact and determining factors with respect to cardiovascular damage in chil- dren is poorly understood. We evaluated the prevalence of alterations in the mineralocorticoid and glucocorticoid axes and their impact on pro-inflam- matory, endothelial damage and oxidative stress parameters in hypertensive children. Methods: 306 children (5-16 years old); Group 1: Hypertensives (n=111); Group 2: normotensives with hypertensive parents (n=101); Group 3: normotensives with normotensives parents (n= 95). Fasting blood samples were drawn for hormone measurements (aldosterone, plasma renin activity (PRA), cortisol (F), cortisone (E)); inflammation vari- ______________________________________ ables (hsRCP, adiponectin, IL-6, IL-8, TNF-α); endothelial damage (PAI-I, P1-d1-163 Adrenals and HPA Axis 1 MMP9 and MMP2 activities) and oxidative stress (malondialdehyde). Famil- The role of S-palmitoylation of human ial hyperaldosteronism type 1 (FH-1) was diagnosed when aldosterone/PRA ratio >10 was associated with the chimeric CYP11B1/CYP11B2 gene. The glucocorticoid receptor in mediating the non- 11β-HSD2 activity was considered altered when the F/E ratio exceeded the genomic actions of glucocorticoids mean + 2 SD with respect to group 3. -

Endocrine Test Selection and Interpretation
The Quest Diagnostics Manual Endocrinology Test Selection and Interpretation Fourth Edition The Quest Diagnostics Manual Endocrinology Test Selection and Interpretation Fourth Edition Edited by: Delbert A. Fisher, MD Senior Science Officer Quest Diagnostics Nichols Institute Professor Emeritus, Pediatrics and Medicine UCLA School of Medicine Consulting Editors: Wael Salameh, MD, FACP Medical Director, Endocrinology/Metabolism Quest Diagnostics Nichols Institute San Juan Capistrano, CA Associate Clinical Professor of Medicine, David Geffen School of Medicine at UCLA Richard W. Furlanetto, MD, PhD Medical Director, Endocrinology/Metabolism Quest Diagnostics Nichols Institute Chantilly, VA ©2007 Quest Diagnostics Incorporated. All rights reserved. Fourth Edition Printed in the United States of America Quest, Quest Diagnostics, the associated logo, Nichols Institute, and all associated Quest Diagnostics marks are the trademarks of Quest Diagnostics. All third party marks − ®' and ™' − are the property of their respective owners. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, and information storage and retrieval system, without permission in writing from the publisher. Address inquiries to the Medical Information Department, Quest Diagnostics Nichols Institute, 33608 Ortega Highway, San Juan Capistrano, CA 92690-6130. Previous editions copyrighted in 1996, 1998, and 2004. Re-order # IG1984 Forward Quest Diagnostics Nichols Institute has been -

Diagnosis and Management of the Patient with Non-Classic CAH Due to 21-Hydroxylase Deficiency
3 180 A Nordenström and Diagnosis and management of 180:3 R127–R145 Review H Falhammar NCAH MANAGEMENT OF ENDOCRINE DISEASE Diagnosis and management of the patient with non-classic CAH due to 21-hydroxylase deficiency Anna Nordenström1,2 and Henrik Falhammar3,4 1Department of Women’s and Children’s Health, Karolinska Institutet, 2Department of Paediatric Endocrinology, Correspondence Astrid Lindgren Children Hospital, Karolinska University Hospital, 3Department of Endocrinology, Metabolism and should be addressed Diabetes, Karolinska University Hospital, and 4Department of Molecular Medicine and Surgery, Karolinska Institutet, to A Nordenström Stockholm, Sweden Email [email protected] Abstract Non-classic congenital adrenal hyperplasia (NCAH) is a relatively common disorder regardless of ethnicity, but most cases are never diagnosed, especially in males. A baseline 17-hydroxyprogesterone measurement may be used for screening, but 17-hydroxyprogesterone measurement after ACTH stimulation is the gold standard. We advocate a CYP21A2 mutation analysis to verify the diagnosis, for genetic counselling and for better prognostic and treatment guidance. Most patients are diagnosed in adolescence and adult life with hirsutism, acne, a PCOS-like picture and fertility issues. Many men with NCAH never seek medical attention and escape diagnosis. Although treatment is somewhat controversial, an early diagnosis and start of treatment may have positive implications on growth and be relevant for preventing and ameliorating the symptoms and consequences of androgen excess that develop over time, including fertility issues. Long-term treatment with glucocorticoids will improve the androgen symptoms but may result in long-term complications, such as obesity, insulin resistance, hypertension, osteoporosis and fractures. European Journal of Endocrinology The glucocorticoid doses should be kept low. -

Scientific Proceedings 2018 CVMA Convention
Scientific Proceedings 2018 CVMA Convention Table of Contents THURSDAY, JULY 5, 2018. .................................................................................................................................................... 5 Business Management Track .............................................................................................................................................. 5 How to Train Your Millennial ................................................................................................................................................... 5 Show Me the Money! ................................................................................................................................................................ 7 Don’t Fear the Feedback .......................................................................................................................................................... 11 It’s All in the Family: Creating a Team Culture ...................................................................................................................... 15 Becoming a Loving Leader ..................................................................................................................................................... 17 FRIDAY, JULY 6, 2018. ......................................................................................................................................................... 22 Companion Animal: Dentistry ........................................................................................................................................ -

AN UPDATE on ATYPICAL HYPERADRENOCORTICISM Doug Mason, DVM, Dvsc, DACVIM (Small Animal Internal Medicine)
South Clinic: 920 Yonge St, Toronto ON – (416) 920-2002 North Clinic: 280 Sheppard Ave. E., Toronto ON - (416) 226-3663 AN UPDATE ON ATYPICAL HYPERADRENOCORTICISM Doug Mason, DVM, DVSc, DACVIM (Small Animal Internal Medicine) Atypical hyperadrenocorticism is defined as a syndrome in which a dog appears to have hyperadrenocorticism based on history, physical examination and clinicopathologic findings but a low dose dexamethasone suppression test, urine cortisol creatinine ratio test and ACTH stimulation tests fall into the currently accepted reference range. This is an uncommon endocrine disorder, which affects middle aged to older dogs and clinically may mimic the signs of hyperadrenocorticism. This disease is thought to be a result of overproduction of estradiol, androstenedione, progesterone, and 17‐hydroxyprogesterone in addition to cortisol. The disease process may be a result of adrenal hyperplasia, adrenal tumours or a functional pituitary microadenoma. It is more common to have the adrenal form of the disease; however both forms have been documented. Clinical signs may be include polyuria, polydipsia, polyphagia, lethargy, abdominal distension, muscle weakness, or recurrent urinary tract infections. Dogs may also present with dermatological signs as their primary complaint. These dermatological abnormalities may include truncal alopecia, thin skin, comedones, bruising, cutaneous hyperpigmentation, calcinosis cutis, pyoderma, dermal atrophy, secondary demodicosis and seborrhea. Abnormalities to a dogs reproductive status may also be noted and include perianal adenoma in females or castrated males, clitoral hypertrophy in female dogs, behavioural estrus in spayed females, testicular atrophy in intact males, prostomegaly in castrated males or behavioural or physical signs of testosterone excess. Common laboratory abnormalities include an elevated alkaline phosphatise, an elevated ALT, hypercholesterolemia, hyperglycemia, and a decreased BUN. -

The Response of C Δ5-Steroids to ACTH Stimulation And
98) Prague Medical Report / Vol. 117 (2016) No. 2–3, p. 98–107 5 The Response of C19 Δ -steroids to ACTH Stimulation and Hypoglycemia in Insulin Tolerance Test for Adrenal Insufficiency Michaela Dušková1, Lucie Kolátorová Sosvorová1, Martin Hill1, Kateřina Šimůnková1,2, Hana Jandíková1, Hana Pospíšilová1, Monika Šrámková1, Mikuláš Kosák2, Michal Kršek2, Václav Hána2, Luboslav Stárka1 1Institute of Endocrinology, Prague, Czech Republic; 23rd Department of Medicine – Department of Endocrinology and Metabolism, First Faculty of Medicine, Charles University and General University Hospital in Prague, Prague, Czech Republic Received April 7, 2016; Accepted September 2, 2016. Key words: Dehydroepiandrosterone – ACTH test – Insulin tolerance test – Adrenal insufficiency – 7-hydroxy-DHEA – 16-hydroxy-DHEA Abstract: Studies on the time course of ACTH- or insulin-induced hypoglycemia stimulating adrenal androgens are usually limited to dehydroepiandrosterone and/or its sulphate. Our data on dehydroepiandrosterone (DHEA) and its hydroxylated metabolites clearly show that measurements of DHEA and its sulphate (DHEAS) are valuable markers of the integrity of the HPA (hypothalamus-pituitary-adrenal) axis. Assessments of HPA function should rely on measurements of baseline 5 and/or stimulated serum cortisol concentrations, and C19 Δ -steroids may provide additional information. The art of stimulation of 7- and 16-hydroxylated metabolites of DHEA can help our understanding of the formation sequence of these compounds. This study was supported by grant no. NT 11277-6 IGA of the Ministry of Health of the Czech Republic. Mailing Address: Prof. RNDr. Luboslav Stárka, MD., DSc., Institute of Endocrinology, Národní 8, 116 94 Prague 1, Czech Republic; e-mail: [email protected] Duškováhttp://dx.doi.org/ M. -

16Th July 2001
AUSTRALASIAN ASSOCIATION OF CLINICAL BIOCHEMISTS INC 5/85 Bourke Rd, Alexandria NSW, 2015 Telephone: +61 2 9669 6600 Facsimile: +61 2 9669 6607 Email: [email protected] Draft Guideline Title Harmonisation of Endocrine Dynamic Testing (HEDT) Document Number: 2018 DGD02 Publication date: Draft for comment September 2018 Next review date: Owner: ESA/AACB/RCPA HEDT Working Party This draft manual for Harmonisation of Endocrine Dynamic Testing is a joint initiative from ESA/AACB/RCPA and is now open for comment and feedback for 90 days. Information provided is a guide only and needs to be verified and modified according to local procedures (e.g. patient consent, sample type, name of test set). A separate paediatric endocrine dynamic testing protocol is in progress with the HDET-P working party. Please direct comments to the chair of the HEDT working party: Dr Cherie Chiang ([email protected]) with the subject heading " HEDT feedback" 2018 DGD02 Harmonisation of Endocrine Dynamic Testing (HEDT) This manual is a joint initiative from ESA/AACB/RCPA and is freely available as a resource for Endocrinologists and Biochemists. Information provided is a guide only and needs to be verified and modified according to local procedures (e.g. patient consent, sample type, name of test set). Queries can be directed to the chair of the HEDT working party. A separate paediatric endocrine dynamic testing protocol is in progress with the HDET-P working party. 2018 DGD02 Page 1 Table of Contents HEDT Working Group Members: ...........................................................................................................4 -

Adrenal Androgenic Response to 2-Hour ACTH Stimulation Test in Women with PCOS
Cynecol Eizdocrinol 1998;1222.3-229 Adrenal androgenic response to 2-hour ACTH stimulation test in women with PCOS C. T. Erel, L. M. Senturk, E. Oral, U. Colgar and E. Ertungealp Istanbul University, Cerrahpasa School of Medicine, Department of Obstetrics and Gynecology, Division of Reproductive Endocrinology, Istanbul, Turkey Key words: POLYCYSTIC 0VAF.Y SYNDROME, .4CTH STIMULATION TEST,21 -HYDKOXYLASE DEFICIENCY, HIKSUTISM ABSTRACT Adrenal function may be abnormal in women with with PCOS than those of healthy controls (p < 0.05, polycystic ovary syndrome (PCOS). This study aims to p < 0.002, p < 0.001, p < 0.015, p < 0.018, evaluate adrenal steroid response lo the adrenocorticotropic respectively). However, the incremental changes in hormone (ACTH) stimulation test and tojnd out the serum 1 7-OHPxto, 1 7-0HPho-0, 1 7-OH&+O, eflect of high serum testosterone levels on adrenal response. 17-OHP12,&0, and the summed rate ofchange in serum We have also investigated any subtle enzyme dqkiency 17-OHP and progesterone in women with PCOS were by extending blood sampling to 2 h with 30 min iritewals not d@erent from those in healthy controls. The incremen- following ACTH administration. Twenty-eight women tal response in terms oj' serum progesterone, DHEAS, For personal use only. with PCOS and 18 healthy controls without hirsutism and testosterone levels to the ACTH stimulation test for and oligomenorrhea were included in the study. After each 30 min interval was not dflerent in women with determining their serum basaj levels of luteinizing PCOS than in healthy controls. We were not able to hormone (LH), follicle-stiMiulating hornzone (FSH), show any critical value for serum basal testosterone and testosterone, dehydroepiandrosterone sulfate (DHEAS), DHEAS levels that would efect response to ACTH 17-hydroxyprogesterone (1 7-OHP), and progesterone, stimulation in terms of 17-OHP levels. -

Technical Details Influence the Diagnostic Accuracy of the 1 Mg
European Journal of Endocrinology (2010) 162 109–113 ISSN 0804-4643 CLINICAL STUDY Technical details influence the diagnostic accuracy of the 1 mg ACTH stimulation test Matthew Wade1, Smita Baid1, Karim Calis2, Hershel Raff3, Ninet Sinaii4 and Lynnette Nieman1 1Program in Reproductive and Adult Endocrinology, National Institute of Child Health and Human Development and 2Pharmacy Department, National Institutes of Health, Clinical Center, Building 10, CRC, 1 East, Room 1-3140, 10 Center Drive, MSC 1109, 53215 Bethesda, Maryland, USA, 3Endocrine Research Laboratory, Medical College of Wisconsin, Aurora St Luke’s Medical Center, Milwaukee, Wisconsin, USA and 4Biostatistics and Clinical Epidemiology Service, National Institutes of Health, Clinical Center, Bethesda, Maryland, USA (Correspondence should be addressed to L Nieman; Email: [email protected]) Abstract Objective: To examine the factors causing inadequate cortisol responses to the 1 mg ACTH stimulation test. Design: Random test assignment (by age and gender) at 0800 or 1600 h. Methods: We recruited 20 healthy adults to each of the three age groups (!40 years, 40–55 years, and O55 years; half females in each group). ACTH stimulation tests were performed in an outpatient clinic at the NIH Clinical Research Center. Plasma cortisol was measured just before, and 30 and 60 min after the administration of 1 mg ACTH (1–24). The ACTH concentration in diluted and administered solutions was measured. Results: Twenty-five volunteers (19 at 1600 h) had a subnormal cortisol response (peak cortisol 10.4–17.5 mg/dl), using a criterion !18 mg/dl (497 nmol/l), for a specificity of 58% (confidence interval (CI) 45–71%).