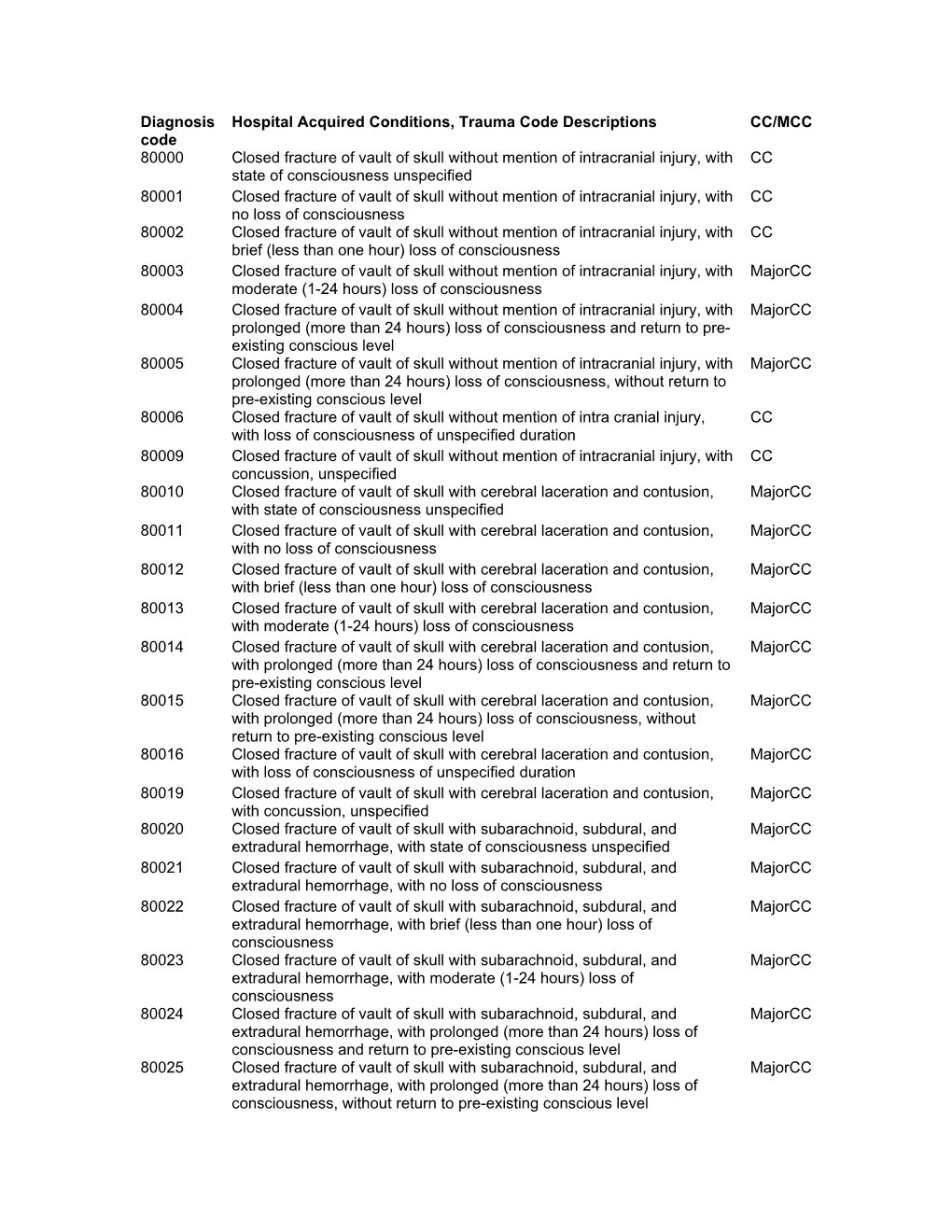
Diagnosis Code Hospital Acquired Conditions, Trauma Code Descriptions CC/MCC 80000 Closed Fracture of Vault of Skull Without
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
PSI Appendix G Version 6.0 Patient Safety Indicators Appendices
AHRQ QI™ ICD-9-CM Specification Version 6.0 Patient Safety Indicators Appendices www.qualityindicators.ahrq.gov APPENDIX G: Trauma Diagnosis Codes Trauma diagnosis codes: (TRAUMID) 80000 Closed skull vault fx 85184 Brain lac nec-proln coma 80001 Cl skull vlt fx w/o coma 85185 Brain lac nec-deep coma 80002 Cl skull vlt fx-brf coma 85186 Brain lacer nec-coma nos 80003 Cl skull vlt fx-mod coma 85189 Brain lacer nec-concuss 80004 Cl skl vlt fx-proln coma 85190 Brain lac nec w open wnd 80005 Cl skul vlt fx-deep coma 85191 Opn brain lacer w/o coma 80006 Cl skull vlt fx-coma nos 85192 Opn brain lac-brief coma 80009 Cl skl vlt fx-concus nos 85193 Opn brain lacer-mod coma 80010 Cl skl vlt fx/cerebr lac 85194 Opn brain lac-proln coma 80011 Cl skull vlt fx w/o coma 85195 Open brain lac-deep coma 80012 Cl skull vlt fx-brf coma 85196 Opn brain lacer-coma nos 80013 Cl skull vlt fx-mod coma 85199 Open brain lacer-concuss 80014 Cl skl vlt fx-proln coma 85200 Traum subarachnoid hem 80015 Cl skul vlt fx-deep coma 85201 Subarachnoid hem-no coma 80016 Cl skull vlt fx-coma nos 85202 Subarach hem-brief coma 80019 Cl skl vlt fx-concus nos 85203 Subarach hem-mod coma 80020 Cl skl vlt fx/mening hem 85204 Subarach hem-prolng coma 80021 Cl skull vlt fx w/o coma 85205 Subarach hem-deep coma 80022 Cl skull vlt fx-brf coma 85206 Subarach hem-coma nos 80023 Cl skull vlt fx-mod coma 85209 Subarach hem-concussion 80024 Cl skl vlt fx-proln coma 85210 Subarach hem w opn wound 80025 Cl skul vlt fx-deep coma 85211 Opn subarach hem-no coma 80026 Cl skull vlt fx-coma nos 85212 -

Management of Pediatric Forearm Torus Fractures: a Systematic
ORIGINAL ARTICLE Management of Pediatric Forearm Torus Fractures A Systematic Review and Meta-Analysis Nan Jiang, MD,*† Zhen-hua Cao, MD,*‡ Yun-fei Ma, MD,*† Zhen Lin, MD,§ and Bin Yu, MD*† many disadvantages, such as heavy, bulky, and requires a second Objectives: Pediatric forearm torus fracture, a frequent reason for emer- visit to the hospital for removal. These flaws of cast may bring gency department visits, can be immobilized by both rigid cast and non- inconvenience to children as well as their families. In recent years, rigid methods. However, controversy still exists regarding the optimal many pediatric clinicians reported other methods to instead tradi- treatment of the disease. The aim of this study was to compare, in a system- tionally used cast, including soft cast,9,10 Futuro wrist splint,8,11 atic review, clinical efficacy of rigid cast with nonrigid methods for immo- and double Tubigrip.11 Although patients that suffered from fore- bilization of the pediatric forearm torus fractures. arm torus fractures can be immobilized by both rigid cast and non- Methods: Literature search was performed of PubMed and Cochrane Li- rigid materials, controversy still exists in the optimal treatment of brary by 2 independent reviewers to identify randomized controlled trials this fracture. comparing rigid cast with nonrigid methods for pediatric forearm torus The aim of this study was to, in a systematic review and fractures from inception to December 31, 2013, without limitation of publi- meta-analysis, compare clinical efficacy of recently used nonrigid cation language. Trial quality was assessed using the modified Jadad scale. immobilization methods with rigid cast. -

Vanderbilt Sports Medicine
Alabama AAP Fall Meeting Sept.19-20, 2009 Pediatric Fracture Care for the Pediatrician Andrew Gregory, MD, FAAP, FACSM Assistant Professor Orthopedics & Pediatrics Program Director, Sports Medicine Fellowship Vanderbilt University Vanderbilt Sports Medicine Disclosure No conflict of interest - unfortunately for me, I have no financial relationships with companies making products regarding this topic to disclose Objectives Review briefly the differences of pediatric bone Review Pediatric Fracture Classification Discuss subtle fractures in kids Discuss a few other pediatric only conditions 1 Pediatric Skeleton Bone is relatively elastic and rubbery Periosteum is quite thick & active Ligaments are strong relative to the bone Presence of the physis - “weak link” Ligament injuries & dislocations are rare – “kids don’t sprain stuff” Fractures heal quickly and have the capacity to remodel Anatomy of Pediatric Bone Epiphysis Physis Metaphysis Diaphysis Apophysis Pediatric Fracture Classification Plastic Deformation – Bowing usually of fibula or ulna Buckle/ Torus – compression, stable Greenstick – unicortical tension Complete – Spiral, Oblique, Transverse Physeal – Salter-Harris Apophyseal avulsion 2 Plastic deformation Bowing without fracture Often deformed requiring reduction Buckle (Torus) Fracture Buckled Periosteum – Metaphyseal/ diaphyseal junction Greenstick Fracture Cortex Broken on Only One Side – Incomplete 3 Complete Fractures Transverse – Perpendicular to the bone Oblique – Across the bone at 45-60 o – Unstable Spiral – Rotational -

Pediatric Orthopedic Injuries… … from an ED State of Mind
Traumatic Orthopedics Peds RC Exam Review February 28, 2019 Dr. Naminder Sandhu, FRCPC Pediatric Emergency Medicine Objectives to cover today • Normal bone growth and function • Common radiographic abnormalities in MSK diseases • Part 1: Atraumatic – Congenital abnormalities – Joint and limb pain – Joint deformities – MSK infections – Bone tumors – Common gait disorders • Part 2: Traumatic – Common pediatric fractures and soft tissue injuries by site Overview of traumatic MSK pain Acute injuries • Fractures • Joint dislocations – Most common in ED: patella, digits, shoulder, elbow • Muscle strains – Eg. groin/adductors • Ligament sprains – Eg. Ankle, ACL/MCL, acromioclavicular joint separation Chronic/ overuse injuries • Stress fractures • Tendonitis • Bursitis • Fasciitis • Apophysitis Overuse injuries in the athlete WHY do they happen?? Extrinsic factors: • Errors in training • Inappropriate footwear Overuse injuries Intrinsic: • Poor conditioning – increased injuries early in season • Muscle imbalances – Weak muscle near strong (vastus medialus vs lateralus patellofemoral pain) – Excessive tightness: IT band, gastroc/soleus Sever disease • Anatomic misalignments – eg. pes planus, genu valgum or varum • Growth – strength and flexibility imbalances • Nutrition – eg. female athlete triad Misalignment – an intrinsic factor Apophysitis • *Apophysis = natural protruberance from a bone (2ndary ossification centres, often where tendons attach) • Examples – Sever disease (Calcaneal) – Osgood Schlatter disease (Tibial tubercle) – Sinding-Larsen-Johansson -

Traumatic Brain Injury(Tbi)
TRAUMATIC BRAIN INJURY(TBI) B.K NANDA, LECTURER(PHYSIOTHERAPY) S. K. HALDAR, SR. OCCUPATIONAL THERAPIST CUM JR. LECTURER What is Traumatic Brain injury? Traumatic brain injury is defined as damage to the brain resulting from external mechanical force, such as rapid acceleration or deceleration impact, blast waves, or penetration by a projectile, leading to temporary or permanent impairment of brain function. Traumatic brain injury (TBI) has a dramatic impact on the health of the nation: it accounts for 15–20% of deaths in people aged 5–35 yr old, and is responsible for 1% of all adult deaths. TBI is a major cause of death and disability worldwide, especially in children and young adults. Males sustain traumatic brain injuries more frequently than do females. Approximately 1.4 million people in the UK suffer a head injury every year, resulting in nearly 150 000 hospital admissions per year. Of these, approximately 3500 patients require admission to ICU. The overall mortality in severe TBI, defined as a post-resuscitation Glasgow Coma Score (GCS) ≤8, is 23%. In addition to the high mortality, approximately 60% of survivors have significant ongoing deficits including cognitive competency, major activity, and leisure and recreation. This has a severe financial, emotional, and social impact on survivors left with lifelong disability and on their families. It is well established that the major determinant of outcome from TBI is the severity of the primary injury, which is irreversible. However, secondary injury, primarily cerebral ischaemia, occurring in the post-injury phase, may be due to intracranial hypertension, systemic hypotension, hypoxia, hyperpyrexia, hypocapnia and hypoglycaemia, all of which have been shown to independently worsen survival after TBI. -

MDS Round-Up 2018! Ronald Orth, RN, CHC, CMAC September 2018
MDS Round-Up 2018! Ronald Orth, RN, CHC, CMAC September 2018 Presented by Presenter • Ronald Orth, RN, CMAC, CHC obtained a nursing degree from Milwaukee Area Technical College in 1985 and a B. A. in Health Care Administration from Concordia University in 1996. Mr. Orth possess over 30 years of nursing experience with over 20 of those in the Skilled Nursing industry. Mr. Orth has extensive experience in teaching Medicare regulations to healthcare providers both in the US and internationally. Mr. Orth is currently the Senior SNF Regulatory Analyst at Relias Learning and is certified in Healthcare Compliance through the Compliance Certification Board (CCB). Ron is also an approved ICD-10-CM trainer with AHIMA. 2 Interview Clarifications Timing of Interviews • Section C (BIMS) – Conducted during the 7 day lookback period, preferably on the ARD or the day before. • Section D (PHQ-9) - Conducted during the 7-day lookback period. Preferably on the ARD or the day before. • Section F (Activities/Preferences) – During the 7-day lookback period. • Section J (Pain) – Conducted anytime during the 5-day lookback period. It is PREFERRED to conduct on the ARD or the day before. 3 Interview Clarifications • Applies to all interview sections • Section C – BIMS • Section D – PHQ-9 • Section F – Activities and Preferences • Section J – Pain • Staff interview should not be completed in place of resident interview if the resident interview should have been completed. • Answer “Gateway” question as “yes” • Dash interview items • B0700 should NOT be coded as “Rarely/Never Understood” if any of the resident interviews were completed. 4 Section I New Item – I0020 • Resident’s primary medical condition • Provides check boxes for 14 different items 5 Section I • Select the condition that represents the primary condition that resulted in resident’s admission to the nursing facility. -

Torus (Buckle) Fracture Discharge Advice
Torus (Buckle) Fracture Discharge Advice Information for you Follow us on Twitter @NHSaaa Find us on Facebook at www.facebook.com/nhsaaa Visit our website: www.nhsaaa.net All our publications are available in other formats What has happened? Your child has sustained a torus fracture, also known as a “buckle” fracture, of the radius and/or ulna (the long bones at the wrist). The bone “buckles” on one side rather than actually breaks and is commonly seen in children as their bones are soft and flexible. Will my child need a cast? Torus fractures heal well without any long-term complications. They do not require any operations or to be placed in a cast. However, using a wrist splint provides comfort and reduces the risk of further injury. It should be worn at all times but can be removed for washing and showering without any risk to the fracture. Simple painkillers such as paracetamol and/or ibuprofen can also be used to reduce discomfort. How long should my child wear the splint for? In general, the older the child is, the longer they will need to wear the splint. We recommend that children under five years old should wear the splint for one week, those age five to ten years should wear it for two weeks and those over ten years should wear it for three weeks. If your child removes the splint before this time but is comfortable and moving their wrist freely then there is no need to insist that they wear the splint for longer. However, if your child is still sore and reluctant to use their wrist when the splint is removed, then you 2 may reapply the splint. -

Musculoskeletal System Imaging
SUMPh “N. Testemitanu” Radiology and Medical imaging department MUSCULOSKELETAL SYSTEM IMAGING M. Crivceanschii, assistant professor GOALS AND OBJECTIVES • to be aware of the role of modern diagnostic imaging modalities • to be familiar with main radiological signs and syndromes • tips and tricks in musculoskeletal imaging IMAGING MODALITIES • that every student should now IMAGING MODALITIES • Conventional Radiography • Fluoroscopy • Arthrography • Computed Tomography • Magnetic Resonance Imaging • Ultrasound • Scintigraphy PLAIN X-RAY FILM • First line study for most medical issues • Excellent for fractures/bony detail • Very limited for soft tissues (ligaments, tendons, muscles) • Only a screening tool in the spine • The radiologist should obtain at least two (2) views of the bone involved at 90° angles to each other • with each view including two adjacent joints FLUOROSCOPY • Arthrography • Tenography • Arteriography • Percutaneous Bone or Soft Tissue Biopsy CT SCANNING • Excellent for bony structural anatomy in the setting of complicated fracture • Less effective than MR for soft tissues and active processes • High radiation Dose • Interventional options MRI SCANNING • Excellent for soft tissue pathology • Good-excellent for bone pathology • No ionizing radiation • NOT patient friendly • Some absolute and relative contraindications ULTRASOUND • Reproducible in trained hands • Excellent for superficial soft tissue elements including tendons and muscles • No ionizing radiation • Patient friendly SCINTIGRAPHY • Image the entire skeleton at once • It provides a metabolic picture • It is particularly helpful in condition such as fibrous dysplasia, Langerhans Cell Histocytosis or metastatic cancer. CONGENITAL SKELETAL ANOMALIES CONGENITAL SKELETAL ANOMALIES • Chromosomal disorders (e. g. Down’s syndrome, Marfan syndrome, Turner’s syndrome, etc.) • Dwarfism (rhizomelic – proximal segments shortening, mesomelic – middle segments, acromelic – distal segments) • Skeletal dysplasias (e. -
Assessment of the Severity of Head Injury
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.39.7.647 on 1 July 1976. Downloaded from Journal ofNeurology, Neurosurgery, andPsychiatry, 1976, 39, 647-655 Assessment of the severity of head injury BRYAN JENNETT From the University Department of Neurosurgery, Institute of Neurological Sciences, Glasgow SYNOPSIS Ranking of head injuries by severity is an essential part of clinical management, of prognosis, oftreatment trials, and oflegal assessment for compensation. Various methods ofassessing severity are reviewed. No one scale is appropriate for all types of injury, or in all circumstances. A check list is provided which should enable every injury to be assessed; its use would facilitate comparison between individual cases of head injury, and between reports from different studies. 'Head injury' is used much more commonly than skull, and there is only a possibility ofintracranial the several rubrics of the International Classifica- complications. This accounts for classifications Protected by copyright. tion of Disease (ICD) which it encompasses; yet based on aposteriori evidence-deciding that the the term itself is not recognized as an entity in injury was not severe because the patient has this classification. In practice it can embrace all made a good recovery. Contemporary concepts degrees of severity from a symptomless bump to of the pathological basis of milder injuries have a blow which causes overwhelming brain damage. exposed the fundamental fallacy ofthis argument, Yet what is necessary for an incident to qualify in that mild concussion is now believed to produce as a head injury is by no means self-evident. Such permanent brain damage, albeit of a minor minimum requirements must indeed be arbitrary degree. -
MDS 3.0 Updates 2018
MDS 3.0 Updates 2018 Cassie Crafton R.N., CDP, RAC-CT Objectives • Understand new MDS 3.0 items in Sections GG, I, J, M, N and O that will be effective October 1st, 2018 • Know which MDS 3.0 items that will be removed and language changes Clarifications with Resident Interviews Timing of Interviews • Section C (BIMS)- to be conducted preferably on the ARD or the day before • Section D (PHQ-9)- to be conducted preferably on the ARD or the day before • Section F (Activities/Preferences)- during the 7 day look back period • Section J (Pain)- to be conducted anytime during the 5 day lookback period preferably on the ARD or the day before Clarifications with Resident Interviews • Staff interview should not be completed in place of resident interview IF the resident interview could have been completed • B0700 should NOT be coded as “Rarely/Never Understood” if any of the resident interviews were completed PPS Changes • Section GG changes • Admission and Discharge Assessments • Language Changes Coding Tips • Admission Performance and Discharge Goals are coded on every Admission Assessment (Start of Part A PPS Stay) regardless of length of stay and planned or unplanned discharge • If the resident has an incomplete stay: – Complete admission performance and goals – Discharge self-care and mobility performance items are not required Section GG- Intent • Functional status is assessed based on the need for assistance when performing self - care and mobility activities • Residents in SNFs have self - care and mobility limitations and are at risk for -

Appendix 1. ICD-9-CM Codes for Defining Non-Fatal Abusive Head Trauma in Children Under the Age of 5 Years Code Meaning 361.00 R
Appendix 1. ICD-9-CM Codes for Defining Non-Fatal Abusive Head Trauma in Children under the Age of 5 Years Code Meaning 361.00 Retinal detachment with retinal defect, unspecified 361.01 Recent detachment, partial, with single defect 361.02 Recent detachment, partial, with multiple defects 361.03 Recent detachment, partial, with giant tear 361.04 Recent detachment, partial, with retinal dialysis 361.05 Recent detachment, total or subtotal 361.10 Retinoschisis, unspecified 361.30 Retinal defect, unspecified 361.33 Multiple defects of retina without detachment 361.8 Retinal detachments and defects- other forms of retinal detachment 361.81 Traction detachment of retina 361.89 Other - Traction detachment with vitreoretinal organization 361.9 Unspecified retinal detachment 362.40 Retinal layer separation, unspecified 362.81 Retinal hemorrhage 780.0 General symptoms- alteration of consciousness 780.01 Coma 780.02 Transient alteration of awareness 780.03 Persistent vegetative state 780.09 Other 780.39 Other convulsions 781.0 Abnormal involuntary movements 781.1 Disturbances of sensation of smell and taste 781.2 Abnormality of gait 781.3 Lack of coordination 781.4 Transient paralysis of limb 781.8 Neurologic neglect syndrome 800.0 Fracture of vault of skull- Closed without mention of intracranial injury 800.00 Closed without mention of intracranial injury- unspecified state of consciousness 800.01 Closed without mention of intracranial injury- with no loss of consciousness 800.02 Closed without mention of intracranial injury- with brief [less -

Useful Markers to Assess Traumatic and Hypoxic Brain Injury
Rom J Leg Med [25] 146-151 [2017] DOI: 10.4323/rjlm.2017.146 © 2017 Romanian Society of Legal Medicine FUNDAMENTAL RESEARCH Useful markers to assess traumatic and hypoxic brain injury Violeta Ionela Chirica1,* _________________________________________________________________________________________ Abstract: Traumatic Brain Injury, TBI, is a very important health issue world wide. Many traumatic events are not witnessed and not declared, especially in mild TBI, mTBI, and therefore not known, not treated or cured. At autopsy the diagnosis of brain injury is in many cases a challenge especially in children with physical abuse. Quite often the judicial system ask for scientific proofs of objectivity in determining the cause of death in head trauma. Sometimes legal medicine is called to determine the extent of the brain injuries following anoxia or hypoxia after a CA resuscitated. Pathology and anatomic pathology sometimes may offer important clues for diagnosis but often there are time consuming. The use of biomarkers in predictive way for prognosis and for diagnosis is a very potent and useful tool in legal medicine. Some of the brain injury biomarkers express the integrity of neurons or neurologic network, including astrocytes, and therefore express the structural integrity of the nervous system. The cutoff limit of these markers is in scientific debates and legal medicine may offer a support for their research. Some biomarkers are studied and presented such as biofluid biomarkers of astroglial injury, S100Beta, Glial Fibrillary acid protein (GFAP), biofluid biomarkers of neuronal injury, Neuron-specific enolase (NSE), Ubiquitin C-terminal hydrolase-L1 (UCH-L1), CK0BB, Brain-derived neurotrophic factor, BDNF, Biofluid biomarkers of axonal injury, Alpha-II spectrin, Tau protein, Neurofilaments, N-Cam or selectins.